

Coronary Calcium Score: CAC Test
Jan 07, 2023
Coronary Artery Calcium Score Test (CAC Test)
There's been a lot of debate regarding the accuracy of CT calcium scoring and what it actually means. I've received a lot of questions from people saying, "Since my calcium score is 0, that means I'm good, right?"
Definitely not!
Another question I get a lot of is, "My LDL is 350, but my calcium score is 0, so I'm good?"
Not at all!
A CT scanner, which is used to give you a calcium score, can not see soft plaque. It only sees mature, hardened, calcified plaque.
The coronary artery calcium score is often called a CAC Test.
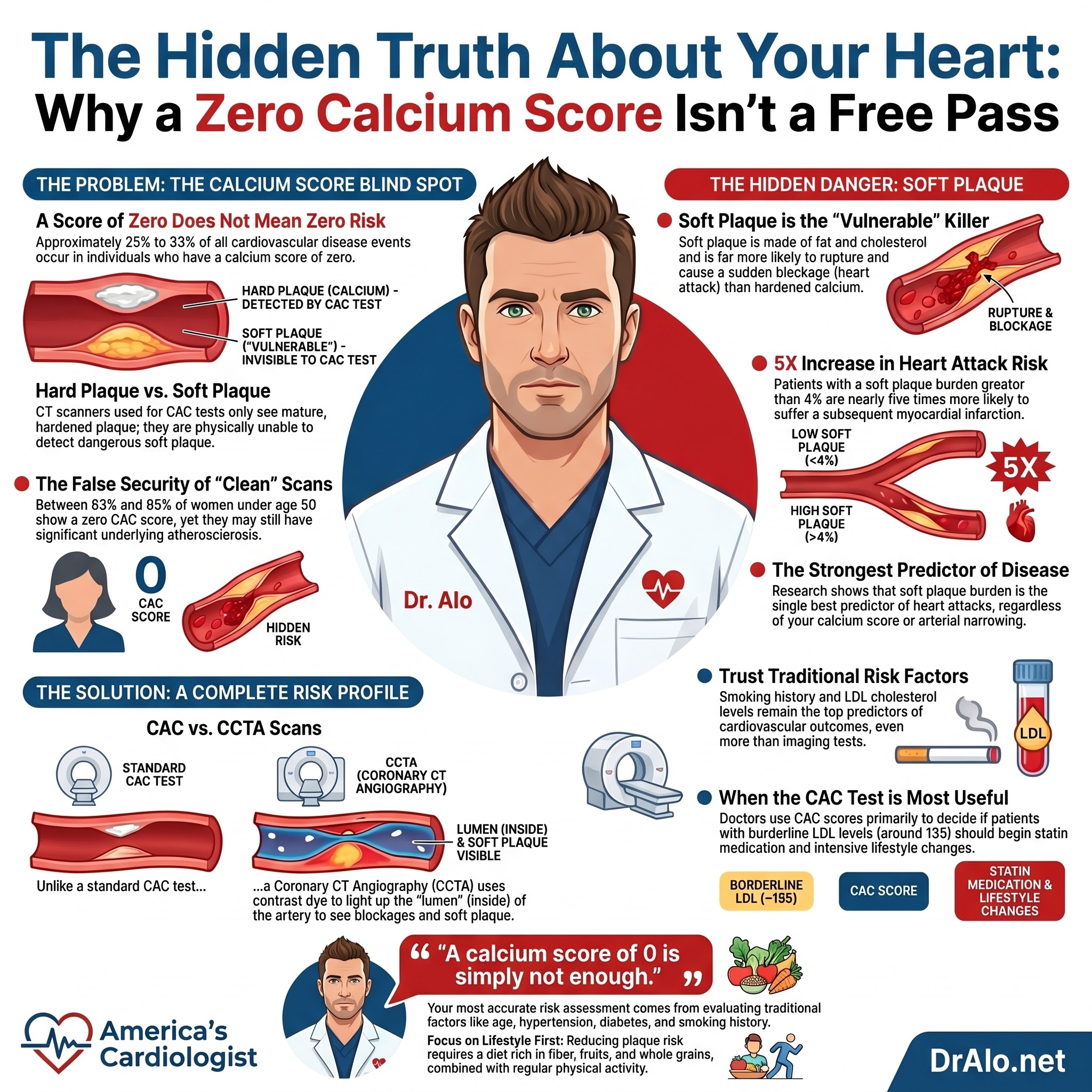
CAC Infographic Summary:
Life Expectancy With High Calcium Score
As a cardiologist, I get this question every day on social media. How long will I live with a high calcium score? Is it possible to live a long, normal life? What should I watch out for? What should be doing? What's my life expectancy with a high calcium score?
Great questions! Let's dive right in!
I've published tons of videos on this topic on my social media accounts, so now is a good time to do an in depth review.

The above image demonstrates calcium in the left anterior descending (LAD) artery. The image on the left shows no calcium in the left anterior descending artery. This is called the "widowmaker".
CT Calcium Score and Soft Plaque
The biggest downside to CT calcium scoring has been the inability to measure soft plaque. Soft plaque is what actually kills you and causes the vast majority of heart attacks.
A coronary artery calcium score (CAC test) is a measure of the amount of calcium in the plaque that has accumulated in the coronary arteries. Calcium usually accumulates on the outside of the arteries, not in the arteries. Hence, it's not usually an indicator or good predictor of outcomes or occlusions.
Coronary calcium starts accumulating in the arterial wall, not in the lumen of the arteries. So, it may be decades before the plaque actually encroaches on eth lumen. So, you are measuring a very late stage finding in the process of atherosclerosis and an even later stage development before it encroaches on the lumen and causes symptoms.
The presence of calcium in the plaque generally means that the plaque is hard, calcified, and has been there for a very long period of time (decades). Calcified plaques are less likely to rupture. A higher coronary calcium score is associated with an increased risk of heart disease and can be an indicator of future cardiovascular events, such as heart attacks or strokes mainly because it indicates pre-existing soft, vulnerable plaque as well.
Coronary calcium scores are typically measured by a computed tomography (CT) scan, which uses X-rays to create detailed images of the inside of the body. While CT scans can accurately measure the amount of calcium in the plaque, they are not able to detect soft plaque, or plaque that is not calcified. This has left the cardiology community debating it's usefulness for years. We never really knew when to use the CAC test or if it should be in the guidelines.
A calcium score is used to detect the presence and extent of plaque in the coronary arteries. Plaque is a build-up of cholesterol, calcium, and other substances in the walls of the arteries, which can narrow or block the arteries and increase the risk of cardiovascular disease.
The test is typically performed using a low-dose CT scan, which uses a small amount of radiation to produce the images. The images are then analyzed to determine the presence and extent of plaque in the coronary arteries.
Difference Between Coronary Artery Calcium Score (CAC) and Coronary CT Angiography (CCTA)
Coronary calcium score and coronary CT angiography are two non-invasive tests that are used to assess the health of the coronary arteries that supply nutrients and oxygen to the myocardium (heart muscle). While both tests involve the use of a computed tomography (CT) scan to create detailed images of the coronary arteries, they differ in their primary purpose and the information they provide.
A coronary calcium score is a measure of the amount of calcium that has accumulated in the coronary arteries as described earlier. See above for more.
Coronary CT angiography (CCTA) is a detailed image of the coronary arteries that is used to identify blockages or narrowing in the arteries. A CT angiogram (CTA) involves the injection of a contrast agent (dye), which makes the arteries light up and more visible with a CT scanner. This allows us to see the inside of the arteries, the lumen.
Coronary CT angiography can provide detailed information on the location and extent of blockages in the coronary arteries, as well as the overall shape and size of the arteries. Because we can look inside the lumen of the arteries, this gives us much more information.
The biggest difference between CAC and CTA is that coronary calcium score only measures the amount of calcium in the plaque but can not detect soft plaque. It's the soft plaque that causes the majority of heart attacks.
Soft plaque is made up of fat, cholesterol, and other substances, and is often referred to as "vulnerable" plaque because it is more prone to rupturing and causing a heart attack or stroke.
While a high coronary calcium score can be a predictor of future cardiovascular events, the presence of soft plaque in the arteries is the most important risk factor.

The above is a CT angiogram showing the inside of the coronary arteries. The images can be reconstructed into these 3D models for evaluation.
What about the New Cleerly AI Powered CCTA Heart Scans Review
Below is an image from the Cleerly AI CCTA Scans

This is just a fancier way of reconstructing CT angiogram images using AI technology (which isn't new in radiology). It does provide better imaging and can show progression over time. But some AI assumptions and algorithms overread the plaque, and they aren't "more reliable" than a standard CT. But patients like these images. It's more marketing hype than anything. They are not superior.
The use of CCTA and AI in radiology isn't new. Here is another scan with almost 13 years of data showing plaque burden and plaque progression.

From:
https://pubmed.ncbi.nlm.nih.gov/36435762/
This technology is evolving and can show plaque progression over time, it just isn't very reliable. Future photon counting CT scans will be able to see into the arterial walls ad have much better resolution.
The issue is soft plaque. A CT scanner can not image soft plaque very well. While you can see the lumen narrowing over the years, you can not see intracranial wall lesions.
Soft Plaque More Dangerous and More Predictive of Heart Disease
Soft plaque is composed of fat, cholesterol, and other substances, and is often referred to as "vulnerable" plaque or "hot" plaque because it is more likely to rupture and cause a blockage in the artery, resulting in a heart attack or stroke.
While a high coronary calcium score is also a predictor of future cardiovascular events, the presence of soft plaque in the arteries is the strongest predictor of heart disease. See study below.
A study published in the Journal of the American College of Cardiology (JACC) evaluated the ability of CT scans to detect soft plaque in the coronary arteries. The study followed over 1,000 participants and found that while CT scans were able to accurately measure the amount of calcium in the plaque, they were not able to detect soft plaque.
The study showed that soft plaque was the best predictor of non-fatal myocardial infarction and heart disease. Here's an exact quote from the study results:
"Low-attenuation plaque burden (soft plaque) was the strongest predictor of myocardial infarction (adjusted hazard ratio, 1.60 (95% CI, 1.10–2.34) per doubling; P=0.014), irrespective of cardiovascular risk score, coronary artery calcium score, or coronary artery area stenosis. Patients with low-attenuation plaque burden greater than 4% were nearly 5 times more likely to have subsequent myocardial infarction (hazard ratio, 4.65; 95% CI, 2.06–10.5; P<0.001)."
With a hazard ratio of 1.60, that means soft plaque was 60% more predictive. Soft plaque burden was the best predictor, irrespective of cardiovascular risk score, coronary artery calcium score, or coronary artery stenosis.
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.119.044720
Another study from the New England Journal of Medicine (NEJM) looked at the use of magnetic resonance imaging (MRI) to detect soft plaque in the coronary arteries. The study followed over 300 participants and found that MRI was able to accurately detect soft plaque in the coronary arteries and could possibly be used as an additional tool to assess the risk of heart disease. These new imaging techniques are very promising and may hold the key to unlocking heart disease progression.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4089955/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2709495/

The above image demonstrates the process by which calcium gets into the arteries. It is usually indicative of older, hardened plaque that is less likely to rupture, but it obviously also means you could have more underlying soft plaque.
Using Calcium Scores in Clinical Settings
So why do we need a calcium score? We don't really. Traditional risk factors are still the best predictors of outcomes. Things like age, sex, smoking, obesity, waist circumference, hypertension, diabetes, prior heart attack or stroke, peripheral artery disease, cholesterol, and LDL are still the best predictors of outcomes. Smoking and LDL being the top predictors.
While a coronary calcium score is a useful tool for assessing the risk of heart disease, it does not detect soft plaque. The use of MRI to detect soft plaque in the coronary arteries may provide more useful information on risk of heart disease, but further research is needed to confirm it's role in clinical practice. Cardiac MRI is still quite rare and underutilized. The technology is still being improved.
When to Use Coronary Artery Calcium?
One reason to use a CAC in clinical practice may be to help you decide if a person with borderline LDL should go on a statin. If you have an LDL of 135 and are otherwise healthy, your doctor may elect to have you try lifestyle changes first. But if your calcium score is elevated, they may opt to put you on cholesterol and LDL-lowering medications right away in addition to lifestyle changes because you are in a higher risk category.
Calcium Score of 0 Is Not Enough
A recent article in Circulation stated that a calcium score of 0 is simply not enough. They go on to say that, "About one-fourth to one-third of the total incident cardiovascular disease (CVD) events occur in those with a CAC of zero, despite some use of lipid-lowering therapy at baseline or during follow-up (in MESA [Multi-Ethnic Study of Atherosclerosis] ≈15% at baseline and 44% during follow-up)."
This indicates that a calcium score of 0 means almost nothing when it comes to predicting cardiovascular disease outcomes.
The researchers said, "Calcified plaque (detected as CAC on computed tomography imaging), however, represents a small proportion of the total plaque burden. Hence, there is a disconnection between zero calcium and zero atherosclerosis, which raises concerns about what age a zero CAC starts to be meaningful."
The researchers also stated that women generally have much lower calcium scores than men, but are still at risk for heart disease. They said, Women have also been shown to have significantly lower CAC, with 83% to 95% of younger women (age<50 years) demonstrating a zero CAC."
The researchers cautioned that, "Clinicians should clearly communicate that a score of zero does not imply that their risk for an event is zero or that they have zero atherosclerosis, but that the application of calcium scoring comes with limitations."
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.119.045026
CT Calcium Score and Life Expectancy
Calcium scoring is used to assess an individual's risk of developing cardiovascular disease, as well as to guide treatment decisions. A high calcium score may indicate the presence of significant plaque in the coronary arteries, which may increase the risk of cardiovascular events such as heart attack or stroke. On the other hand, a low calcium score may indicate a lower risk of cardiovascular disease.
Several factors can contribute to the development of plaque in the coronary arteries, including genetics, unhealthy diet, lack of physical activity, and tobacco use. Therefore, it is important to adopt a healthy lifestyle in order to reduce the risk of developing plaque in the coronary arteries. This includes eating a diet rich in fruits, vegetables, fiber, and whole grains, engaging in regular physical activity, and avoiding smoking.
Another study, published in the New England Journal of Medicine, found that calcium scoring was associated with a significant reduction in the risk of cardiovascular events in individuals with intermediate risk. This study also found that individuals with a high calcium score who received intensive medical therapy had a lower risk of cardiovascular events compared to those who received standard therapy.
Note below, that calcium score would not be non negative until the last two stages of atherosclerosis.

Final Word on Calcium Score
Calcium scoring may be useful for assessing your risk of developing cardiovascular disease, but it should not completely replace traditional risk factors. The test is non-invasive and can be used to guide treatment decisions and identify individuals who may benefit from intensive medical therapy.
Multiple studies have demonstrated the usefulness of calcium scoring in predicting the risk of cardiovascular events and guiding treatment decisions. But just be wary that a CAC can not detect soft plaque and you are not "cleared" if you have a calcium score of 0. The most accurate risk assessment is still based on traditional risk factors, especially LDL and smoking history!
I've published several videos on calcium scoring on my socials, check them out as well!
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















