Why You Should Care About Non-HDL-Cholesterol More Than LDL
Jan 05, 2025
Non-HDL Cholesterol: What It Is and Normal Levels
If you have ever looked at your cholesterol panel and noticed a number called non-HDL cholesterol, you might have wondered what it means and why your doctor cares about it. In many ways, non-HDL cholesterol is a more complete picture of your cardiovascular risk than LDL cholesterol alone. In this article, I am going to explain exactly what non-HDL cholesterol is, what a healthy level looks like, who needs to pay closest attention to it, and how to lower it.
What Is Non-HDL Cholesterol?
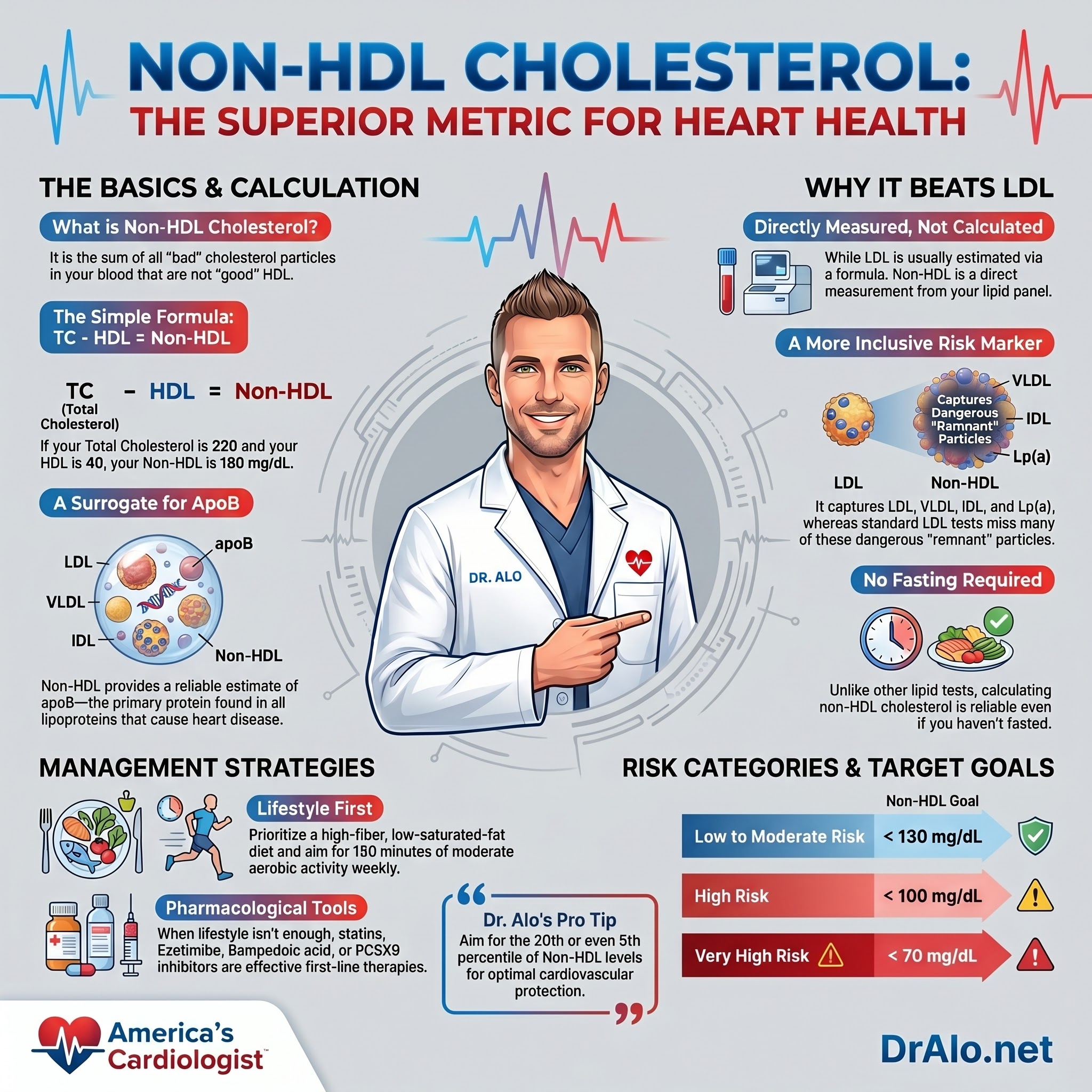
Non-HDL cholesterol is exactly what it sounds like: it is all of the cholesterol in your blood that is not carried by HDL particles. The formula is simple.
Non-HDL Cholesterol = Total Cholesterol minus HDL Cholesterol
For example, if your total cholesterol is 220 mg/dL and your HDL is 40 mg/dL, your non-HDL cholesterol is 180 mg/dL. Many labs now report this number automatically on a standard lipid panel, so you may already have it.
What makes non-HDL cholesterol clinically powerful is what it captures. It accounts for the cholesterol carried inside every potentially atherogenic lipoprotein in circulation. That includes LDL (low-density lipoprotein), VLDL (very-low-density lipoprotein), IDL (intermediate-density lipoprotein), Lp(a) (lipoprotein(a)), and chylomicron remnants. All of these particles carry the apolipoprotein B protein on their surface. All of them can penetrate the arterial wall and contribute to plaque formation. Non-HDL captures the entire picture in a single number that comes directly off your standard blood draw.
Infographic Summary:
What Is a Normal Non-HDL Cholesterol Level?
This is one of the most commonly searched questions about non-HDL cholesterol, and the answer depends on your individual cardiovascular risk profile.
The general rule endorsed by the American College of Cardiology and the American Heart Association is that your non-HDL target should be 30 mg/dL above your LDL target. This is because the atherogenic lipoproteins beyond LDL (primarily VLDL and its remnants) carry roughly 30 mg/dL worth of additional cholesterol mass in most people.
Here are the standard non-HDL cholesterol goals by risk category:
Low to Moderate Risk: below 130 mg/dL
High Risk (prior heart disease, diabetes, chronic kidney disease): below 100 mg/dL
Very High Risk (multiple cardiac events, very high Lp(a)): below 70 mg/dL
Personally, I do not stop there. I prefer to see my patients in the lowest risk percentiles, ideally below the 20th percentile for their age and sex, and in higher-risk patients, even below the 5th percentile. My own non-HDL, along with my LDL and ApoB, runs in the low 40s to low 50s. That is a target I believe the evidence supports for long-term cardiovascular protection.
Why Non-HDL Cholesterol Is Better Than LDL Cholesterol
LDL cholesterol has been the centerpiece of cardiovascular risk management for decades, but it has a significant limitation: it is almost never directly measured. The LDL number on your standard lipid panel is typically estimated using the Friedewald equation, which calculates LDL from total cholesterol, HDL, and triglycerides. That calculation becomes increasingly inaccurate as triglycerides rise above 150 mg/dL and can dramatically underestimate true atherogenic burden in patients with metabolic disease.
Non-HDL cholesterol is directly measured, not calculated. You subtract one measured value (HDL) from another measured value (total cholesterol). There is no estimation, no formula that breaks down at high triglyceride levels, and no requirement for fasting before the blood draw.

There is also a biological reason why non-HDL matters beyond LDL. LDL particles spend part of their lifespan in a process called reverse cholesterol transport, where they interact with HDL particles through an enzyme called cholesterol ester transfer protein (CETP) and help shuttle cholesterol back to the liver for elimination. So LDL is not purely a villain. VLDL, IDL, and Lp(a), which are also captured in non-HDL, do not have this redemptive function. They are atherogenic from the moment they enter circulation.
When apoB and non-HDL are discordant, meaning they do not agree with each other, cardiovascular risk tracks more closely with apoB. That is why apoB remains the gold standard in my practice. But when apoB is unavailable, non-HDL is the best available surrogate and is strongly validated across multiple outcomes studies.
Non-HDL Cholesterol and Residual Cardiovascular Risk After Statin Therapy
This is a concept that does not get enough attention in primary care settings, and it is one of the main reasons non-HDL cholesterol matters even for patients already on a statin.
Statins are extraordinarily effective at lowering LDL cholesterol. But some patients, even after reaching their LDL goal on a statin, continue to have elevated non-HDL cholesterol. This happens when triglyceride-rich lipoproteins, particularly VLDL and its remnants, remain elevated despite LDL being well controlled. This gap between LDL goal and non-HDL goal is sometimes called residual cardiovascular risk.
In clinical trials, residual non-HDL elevation after statin therapy is independently associated with continued risk for heart attack and stroke. The statin did its job on LDL, but the atherogenic burden from VLDL remnants and IDL remained elevated and continued driving plaque progression.
This is exactly the scenario where non-HDL cholesterol becomes indispensable as a clinical tool. If a patient's LDL looks great but non-HDL is still above goal, that gap signals ongoing risk that may require additional interventions, including triglyceride-lowering therapy, weight loss, improved glycemic control, or further intensification of lipid-lowering treatment.
Transfer of Cholesterol From HDL To LDL
Below is a diagram showing the transfer of cholesterol from HDL particles to LDL particles in exchange for triglycerides using the CETP.

Who Benefits Most From Non-HDL Cholesterol Testing?
While non-HDL cholesterol is useful for everyone, it is especially superior to LDL cholesterol in specific populations where LDL is most likely to be artificially low or misleading.
Type 2 Diabetes. People with type 2 diabetes frequently have a dyslipidemia pattern characterized by elevated triglycerides, low HDL, and a shift toward small, dense LDL particles. In this setting, the LDL cholesterol number is often deceptively low because each particle carries less cholesterol mass, even though the total particle count (and therefore atherogenic burden) is elevated. Non-HDL captures this burden in a way that LDL cholesterol simply cannot.
Metabolic Syndrome. Metabolic syndrome involves the combination of central obesity, elevated triglycerides, low HDL, elevated blood pressure, and impaired fasting glucose. The lipid profile in metabolic syndrome is almost defined by high VLDL and remnant cholesterol, neither of which shows up adequately in a standard LDL measurement. Non-HDL directly captures these atherogenic remnants.
Obesity. Elevated body weight, particularly visceral adiposity, drives overproduction of VLDL in the liver. Higher VLDL means more cholesterol mass outside the LDL fraction, which means LDL alone misses a significant portion of atherogenic risk. Non-HDL accounts for this VLDL-driven excess.
Hypertriglyceridemia. When triglycerides rise above 150 mg/dL, the Friedewald LDL calculation becomes progressively unreliable. At triglycerides above 400 mg/dL, the formula is considered invalid. Non-HDL bypasses this problem entirely. It does not depend on triglyceride levels for its accuracy.
In all four of these groups, relying on LDL cholesterol alone understates cardiovascular risk. Non-HDL provides a more complete and clinically actionable picture.
More HDL Particles than LDL Particles
One thing to note is that there are about 27 times more HDL particles in circulation than LDL particles. HDL particles are much smaller and hence carry much less cholesterol. That's why your HDL cholesterol is much lower than your LDL cholesterol.

How To Lower Non-HDL Cholesterol
Lowering non-HDL cholesterol follows the same framework as lowering LDL and ApoB. Both lifestyle and pharmacological strategies are effective, and in most patients, both together produce the best outcomes.
Dietary changes. Reduce saturated fat intake, which drives hepatic LDL receptor downregulation and raises apoB-containing lipoproteins. Increase dietary fiber, particularly soluble fiber, which binds bile acids in the gut and forces the liver to pull more cholesterol from circulation. For patients with elevated triglycerides driving high non-HDL, reducing refined carbohydrates and alcohol is especially effective.
Exercise and weight management. Regular aerobic exercise at 150 or more minutes per week improves lipoprotein metabolism, lowers triglycerides, raises HDL, and reduces VLDL output from the liver. Even modest weight loss of 5 to 10 percent of body weight can significantly improve the non-HDL picture in obese patients.
Statins. First-line pharmacological therapy. Statins reduce hepatic cholesterol synthesis, upregulate LDL receptors, and lower LDL, VLDL remnants, and Lp(a) to varying degrees. They reduce non-HDL cholesterol substantially in most patients.
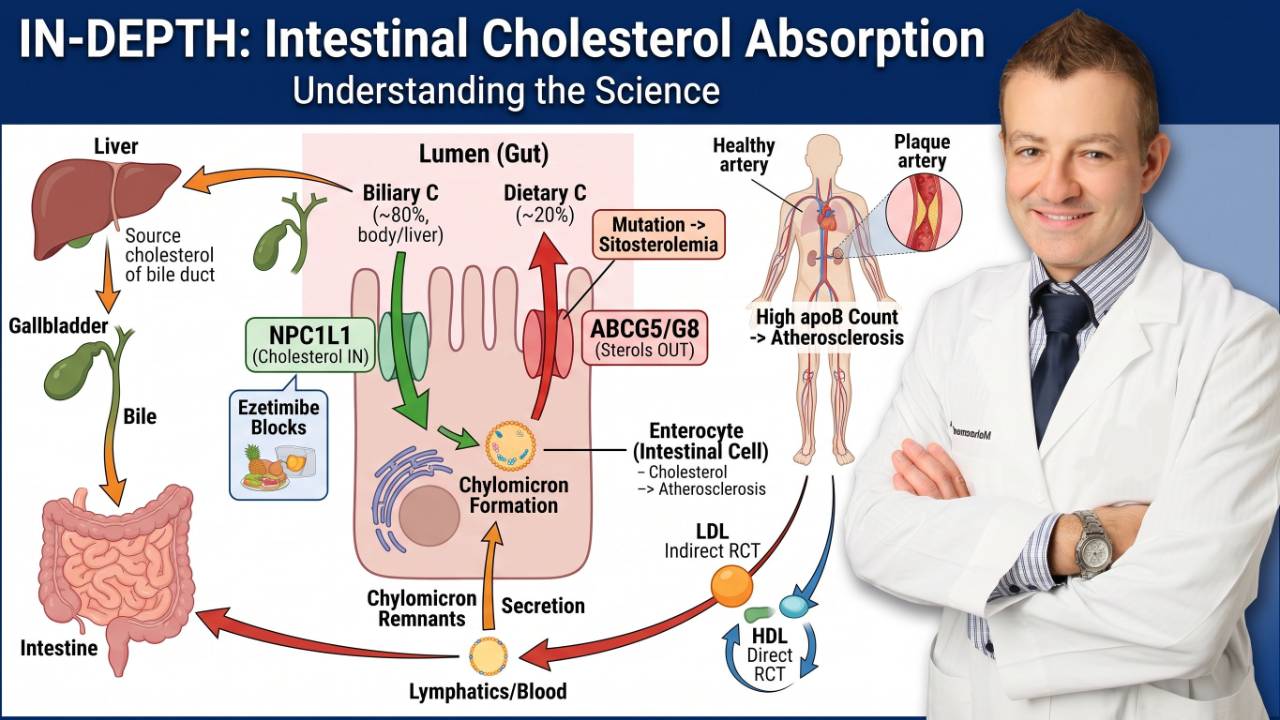
Ezetimibe. Blocks intestinal cholesterol absorption. Added to statin therapy, ezetimibe provides additional non-HDL reduction with minimal side effects. It is an important step before moving to injectable therapies.
PCSK9 inhibitors. Agents like evolocumab (Repatha) and alirocumab (Praluent) dramatically upregulate LDL receptors and can reduce LDL and non-HDL by 50 to 60 percent on top of statin therapy. Inclisiran, an siRNA-based PCSK9 inhibitor, achieves similar reductions with only two injections per year.
Bempedoic acid. An oral non-statin option that inhibits cholesterol synthesis upstream of the statin target. Useful for statin-intolerant patients or as add-on therapy.
The Role of ApoB: When to Go Beyond Non-HDL
Non-HDL cholesterol is a strong surrogate for apoB and is validated across major cardiovascular outcomes trials. But non-HDL and apoB are not always concordant. In cases where they diverge, cardiovascular risk tracks more closely with apoB.
One landmark study in the Journal of Lipid Research demonstrated that even with identical hazard ratios on average, apoB pointed to higher risk in a meaningful subset of individuals where non-HDL underestimated the burden. This is why I order apoB routinely in my practice and consider it the definitive number for lipid risk assessment.
Non-HDL is an excellent tool when apoB is unavailable, and it is validated, accessible, and derived directly from the standard lipid panel every patient already gets. Use non-HDL as a minimum. Use apoB whenever you can.
Understanding Non-HDL Cholesterol: The Cardiologist's Guide
Non-HDL cholesterol has gained significant attention in cardiovascular medicine due to its robust predictive power for atherosclerotic cardiovascular disease (ASCVD). As one of the foremost lipidologists, Dr. Thomas Dayspring emphasizes the importance of non-HDL cholesterol in assessing lipid-related risk beyond traditional measures like LDL cholesterol.
Total cholesterol (TC) represents the cholesterol carried in all the circulating lipoproteins. If one subtracts the cholesterol in HDL particles (HDL-C) from total cholesterol (TC), one would have the cholesterol mass that is not in the HDL particles. This represents apoB-cholesterol and is more conveniently called non-HDL-cholesterol (non-HDL-C). It is a surrogate (guesstimate) of apoB.
Non-HDL-C can be used as a surrogate for apoB (see above graphics). Because this is easy to calculate from any lipid panel, many have advocated for its use.
As an example, your total cholesterol is 220 mg/dL and your HDL is 40 mg/dL. You take 220-40 and your number is 180 mg/dL. So, your non-HDL-C is 180 mg/dL. This is just an example of how you can calculate this yourself. Many labs now report this value in their standard lipid panel results.
What is Non-HDL Cholesterol?
Non-HDL cholesterol refers to the total cholesterol minus HDL cholesterol. It encompasses all the atherogenic lipoproteins, including:
- Low-Density Lipoprotein (LDL)
- Intermediate-Density Lipoprotein (IDL)
- Very-Low-Density Lipoprotein (VLDL)
- Lipoprotein(a) [Lp(a)]
- Chylomicron remnants
Since these particles are directly involved in the formation of atherosclerotic plaques, non-HDL cholesterol is a comprehensive marker for cardiovascular risk.
Why Focus on Non-HDL Cholesterol?
1. Broader Risk Assessment Than LDL Cholesterol
While LDL cholesterol has traditionally been the primary target for therapy, it doesn’t account for other atherogenic lipoproteins. Non-HDL cholesterol bridges this gap, making it a superior predictor of ASCVD risk.
2. Simple and Reliable
Calculating non-HDL cholesterol doesn’t require fasting, unlike other lipid parameters like triglycerides. This simplifies screening and monitoring in clinical practice.
3. Better Alignment with Outcomes
Studies show that non-HDL cholesterol correlates more closely with cardiovascular events than LDL cholesterol, particularly in patients with high triglycerides or diabetes.
Non-HDL More Accurate As A Risk Assessment
The benefit of using non-HDL-C is that it also includes the cholesterol that is not only in LDL particles but also VLDL particles and their smaller, cholesterol-rich remnants which can be especially prominent when triglycerides start to increase above 100 mg/dL and especially when triglycerides are > 150 mg/dL. Neither calculated nor directly measured LDL-C will evaluate VLDL remnants. A better and more accurate name for non-HDL-cholesterol is apoB-cholesterol.
Although, like LDL-C, non-HDL-C, and apoB have high correlation, they can be discordant in which case ASCVD risk better correlates with apoB. There is no way to diagnose LDL-C / non-HDL-C discordance with apoB without obtaining all the values.
Non-HDL-C has been validated as a great risk assessment tool when apoB is not available.
Further reading:
https://pubmed.ncbi.nlm.nih.gov/30595507/
https://pubmed.ncbi.nlm.nih.gov/33736827/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9791017/
When looking at the highest tertile of apoB vs non-HDL-C, apoB was more predictive of CV risk. I highly recommend reading the original article. They corrected for all confounders and covariates.
Study:
https://www.ahajournals.org/doi/10.1161/circulationaha.104.532499
Another study examined the ability of apoB and non-HDL-C to correctly predict risk when the two values were discordant. They found that, “The result is that even with identical overall hazard ratios, apoB points to higher risk in a substantial number of individuals whereas the converse is the case for non- high-density lipoprotein cholesterol”. Risk follows apoB.
Study:
https://www.lipidjournal.com/article/S1933-2874(10)00044-9/fulltext
Dr. Alo's Official Lipid Targets
I prefer to be under the 20th percentile, or even under the 5th percentile depending on your risk factors and medical history.
Personally, my LDL, apoB, and Non-HDL hover in the low 40s to 50s and I have never had a cardiac event or risk factors.

Management Strategies For Lowering non-HDL Cholesterol
1. Lifestyle Modifications
- Diet: Emphasize heart-healthy foods, including vegetables, fruits, whole grains, and lean proteins.
- Exercise: Aim for at least 150 minutes of moderate aerobic activity weekly.
- Weight Management: Achieving a healthy weight can significantly lower non-HDL cholesterol levels.
2. Pharmacological Interventions
- Statins: First-line therapy for lowering atherogenic lipoproteins.
- Ezetimibe: Can be added to statin therapy for additional LDL and non-HDL cholesterol reduction.
- PCSK9 Inhibitors: Effective for individuals with genetic lipid disorders or very high cardiovascular risk.
- Bempedoic Acid: Can be added to these and is in pill formation, not an injection
The Role of Advanced Lipid Testing
For individuals with persistent cardiovascular risk despite optimal LDL cholesterol levels, advanced lipid testing can further evaluate:
- Apolipoprotein B (ApoB): Direct measure of atherogenic particle concentration.
- Lipoprotein(a): A genetically inherited lipoprotein associated with increased cardiovascular risk.
Non-HDL Cholesterol: A Paradigm Shift
As Dr. Thomas Dayspring often emphasizes, non-HDL cholesterol represents a shift towards a more inclusive and accurate approach to managing cardiovascular risk. By focusing on all atherogenic lipoproteins, clinicians can better tailor therapies and achieve superior outcomes for their patients.
Final Thoughts:
Non-HDL cholesterol is more than just a number—it’s a critical component of modern cardiovascular risk assessment. By integrating this measure into routine practice, healthcare providers can identify at-risk individuals earlier and more accurately. Whether through lifestyle changes, medications, or advanced testing, managing non-HDL cholesterol is pivotal in the fight against heart disease.
For patients and practitioners alike, understanding and addressing non-HDL cholesterol is a cornerstone of proactive, personalized cardiovascular care.
Frequently Asked Questions About Non-HDL Cholesterol
Is non-HDL cholesterol the same as ApoB?
No, but non-HDL is a close surrogate for apoB. Both measure the burden of atherogenic lipoproteins in your blood. ApoB counts the actual number of lipoprotein particles directly, while non-HDL measures the total cholesterol mass carried inside those particles. They are strongly correlated in most patients, but in certain metabolic conditions they diverge, and when they do, cardiovascular risk follows apoB more closely. If you can get an apoB measured, do it. Non-HDL is the best available alternative when apoB is not reported.
Can I calculate my non-HDL cholesterol at home?
Yes, if you have a copy of any standard lipid panel, you can calculate it yourself. Take your total cholesterol and subtract your HDL cholesterol. The result is your non-HDL cholesterol. No additional tests or formulas are needed. For most adults, a number below 130 mg/dL is considered acceptable, though your individual target may differ based on your risk profile.
Does measuring non-HDL cholesterol require fasting?
No. This is one of the practical advantages of non-HDL over traditional LDL measurement. Because non-HDL is directly calculated from total cholesterol and HDL, both of which are stable in the non-fasting state, a fasting blood draw is not required. This makes non-HDL particularly convenient for routine screening and monitoring.
What causes high non-HDL cholesterol?
High non-HDL cholesterol can be caused by elevated LDL, elevated VLDL from high triglycerides, elevated Lp(a), or some combination of all three. Common drivers include a diet high in saturated fat and refined carbohydrates, excess body weight especially visceral adiposity, type 2 diabetes or insulin resistance, hypothyroidism, chronic kidney disease, and genetic lipid disorders such as familial hypercholesterolemia. Identifying which fraction is driving the elevation shapes the treatment approach.
Is non-HDL cholesterol more important than LDL?
In many patients, yes. Non-HDL captures a broader range of atherogenic lipoproteins than LDL alone, does not depend on a formula that can break down at high triglycerides, and does not require fasting. For patients with diabetes, metabolic syndrome, obesity, or elevated triglycerides, non-HDL is especially superior to LDL as a risk assessment tool. That said, apoB remains the most informative single lipid number for assessing true atherogenic particle burden.
References
Non-HDL Cholesterol and Cardiovascular Risk: Systematic Review:
https://pubmed.ncbi.nlm.nih.gov/30595507/
Non-HDL Cholesterol Versus ApoB in Risk Assessment:
https://pubmed.ncbi.nlm.nih.gov/33736827/
ApoB and Non-HDL in Clinical Practice Review:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9791017/
ApoB vs Non-HDL in Highest Tertile Analysis (Circulation):
https://www.ahajournals.org/doi/10.1161/circulationaha.104.532499
ApoB and Non-HDL Discordance Study (Journal of Clinical Lipidology):
https://www.lipidjournal.com/article/S1933-2874(10)00044-9/fulltext
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine