

STEMI versus NSTEMI Two Very Different Types of Heart Attacks
May 12, 2025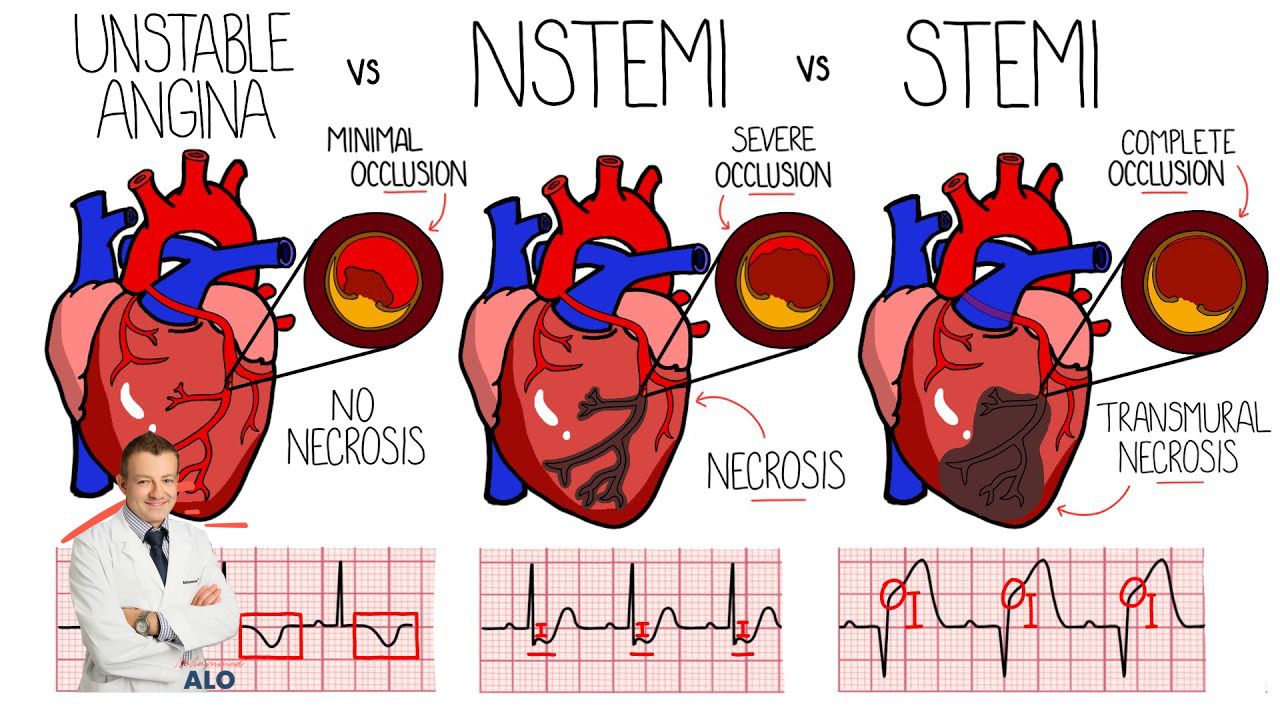
STEMI vs NSTEMI: Key Differences Explained
When I teach medical students, residents, fellows, and practicing cardiologists at conferences, one topic always comes up early: what is the real difference between a STEMI and an NSTEMI, and why does it matter? The answer is straightforward but absolutely critical. One of these diagnoses requires you to activate the cath lab immediately, at 3 in the morning, on a holiday, no exceptions. The other allows for a more measured, risk-stratified approach. Understanding this distinction can be the difference between saving a heart and losing one.
ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI) are both types of heart attacks caused by blocked blood flow to the heart muscle. They share a common underlying mechanism but differ significantly in the degree of blockage, how they appear on an ECG, how troponin behaves, how urgently they need to be treated, and what the mortality data actually shows.
Infographic Summary
STEMI vs NSTEMI: Side-by-Side Comparison
Here is a reference table covering the most clinically important categories. Every serious cardiology resource includes this comparison, and for good reason. It anchors the entire discussion that follows.
| Category | STEMI | NSTEMI |
|---|---|---|
| Definition | ST-Segment Elevation Myocardial Infarction | Non-ST-Segment Elevation Myocardial Infarction |
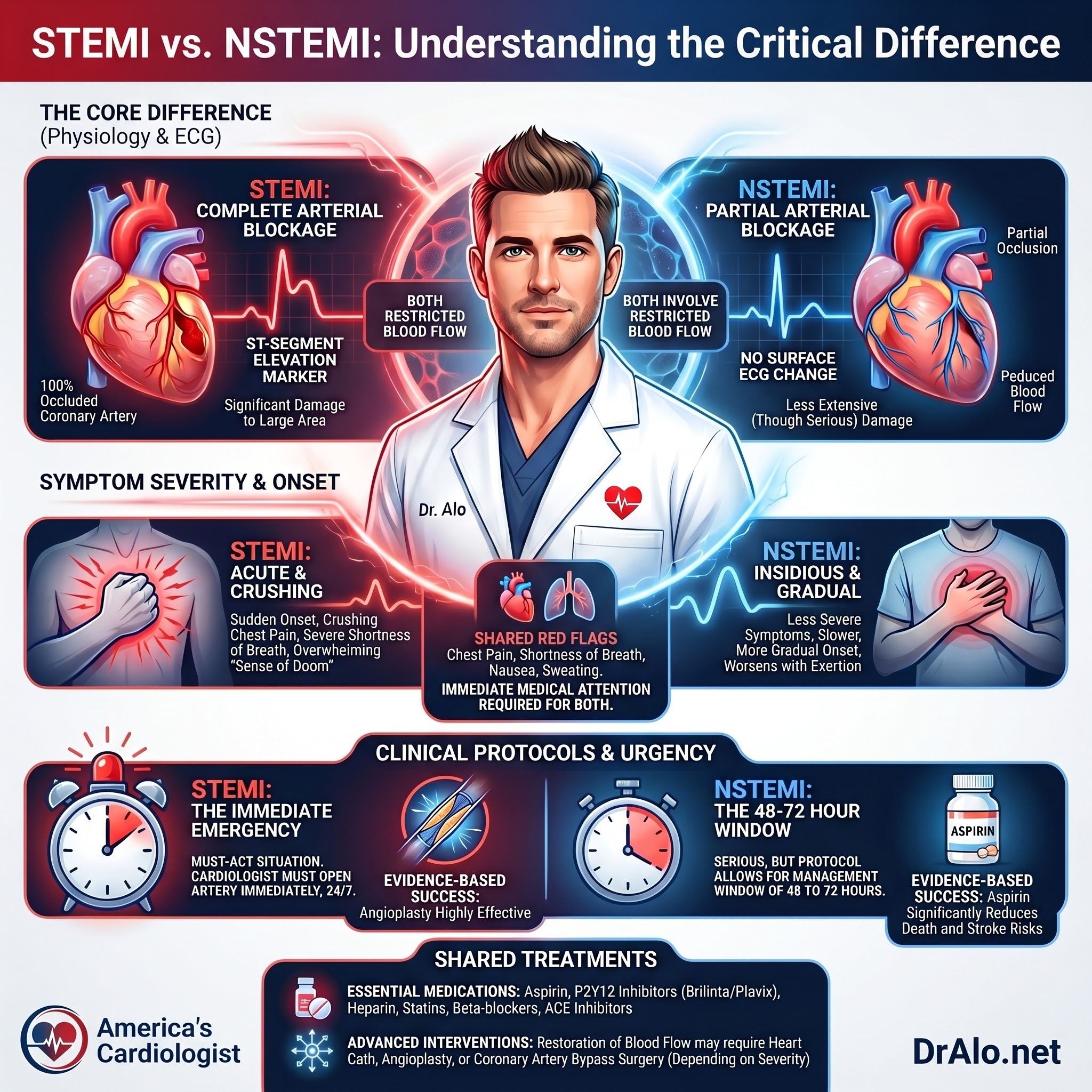
| Coronary Artery Blockage | Complete (100%) occlusion | Partial occlusion |
| ECG Changes | ST elevation in 2+ contiguous leads; new LBBB | ST depression, T-wave inversions, or normal ECG |
| Troponin Elevation | Rapid, massive rise within 1 to 3 hours | Smaller or delayed rise; requires serial testing |
| Severity | Most severe; large area of myocardium at risk | Serious but typically less immediate myocardial damage |
| Urgency of Cath Lab Activation | Immediate (door-to-balloon goal: under 90 minutes) | Risk-stratified: 2 hours if very high-risk, or 24 to 72 hours |
| Typical Symptoms | Sudden crushing chest pain, diaphoresis, sense of doom | More gradual onset; chest pressure or exertional shortness of breath |
| In-Hospital Mortality | Approximately 4 to 7% | Approximately 2 to 5%; higher 6-month and 1-year mortality |
| First-Line Treatment | Immediate primary PCI (angioplasty with stenting) | Dual antiplatelets, anticoagulation, and risk-stratified PCI |
What is a STEMI?
STEMI is the most severe type of heart attack. It occurs when a coronary artery becomes completely and suddenly blocked, cutting off all blood flow to the downstream heart muscle. Without intervention within minutes to hours, that muscle dies. This is not a partial inconvenience. This is a full cardiac emergency.
The complete blockage is almost always triggered by the rupture of a vulnerable atherosclerotic plaque. When that plaque ruptures, a clot forms instantly and occludes the vessel. The area of myocardium supplied by that artery begins to die in real time. This is exactly why the phrase "time is muscle" exists in cardiology. Every minute of delay translates directly into more irreversible damage.
What is an NSTEMI?
NSTEMI occurs when a coronary artery is partially blocked, reducing but not completely stopping blood flow to the heart muscle. Less muscle is at immediate risk, which is why the in-hospital mortality is lower than STEMI. But do not let that number mislead you. NSTEMI is still a heart attack. It still causes myocardial injury. And if left untreated or mismanaged, it can progress to a full STEMI.
One critical distinction that gets missed frequently: NSTEMI and unstable angina look identical on an ECG. The only thing that separates them is troponin. If troponin is elevated, it is an NSTEMI. If troponin is normal, it is unstable angina. This distinction drives treatment urgency and risk stratification, so getting it right matters.
ECG Criteria: How to Tell Them Apart on the Monitor
The 12-lead ECG is the first diagnostic tool used for any patient presenting with chest pain or suspected acute coronary syndrome. Here is exactly what to look for.
STEMI diagnostic criteria:
ST elevation of at least 1mm in two or more contiguous limb leads, or at least 2mm in two or more contiguous precordial (chest) leads. A new left bundle branch block (LBBB) should be treated as a STEMI equivalent until proven otherwise, because LBBB itself obscures normal ST analysis and often indicates a proximal LAD occlusion.
When a patient arrives with LBBB and you cannot confirm whether it is new or old, apply the Sgarbossa criteria. These are three ECG findings that, when present in the setting of LBBB, suggest acute myocardial infarction: concordant ST elevation of 1mm or more in any lead; concordant ST depression of 1mm or more in leads V1 through V3; or excessively discordant ST elevation of 5mm or more. The Smith-modified Sgarbossa criteria refines this further by using a ratio of ST-segment deviation to the depth of the preceding S wave, improving specificity significantly.
NSTEMI ECG findings:
ST depression in two or more contiguous leads, T-wave inversions, or a completely normal ECG. That last point is critical and I want to repeat it: a normal ECG does not rule out NSTEMI. This is where troponin becomes the deciding test. Never discharge a patient with classic symptoms based on a normal ECG alone.
Troponin: The Biomarker That Confirms the Diagnosis
Troponin I and troponin T are proteins released from cardiac muscle cells into the bloodstream when those cells are damaged or dying. Both STEMI and NSTEMI elevate troponin, but the pattern is different and clinically meaningful.
In STEMI, troponin rises rapidly and massively. The complete occlusion destroys a large territory of myocardium quickly, releasing troponin into circulation within one to three hours of symptom onset. The rise is dramatic and unmistakable on serial testing.
In NSTEMI, the troponin rise can be smaller and more delayed. Because blood flow is only partially reduced, the damage builds more slowly. A single normal troponin drawn when the patient first walks in does not rule out NSTEMI if they presented early in their symptom course. Serial testing is mandatory.
Modern emergency departments now use high-sensitivity cardiac troponin assays, specifically hs-cTnI or hs-cTnT. These assays detect troponin at concentrations far below what older conventional assays could identify, which has transformed how quickly we can diagnose or rule out NSTEMI. Two rapid protocols are now widely used. The 0-hour and 1-hour protocol (0h/1h algorithm) draws troponin on arrival and repeats it at exactly 60 minutes. Based on the absolute values and the delta change between draws, patients are stratified into rule-in, observe, or rule-out categories. The 0h/3h protocol is the alternative for centers that have not yet implemented the 0h/1h pathway. Both are endorsed by the ESC guidelines for chest pain evaluation.
One important clinical caveat: troponin is a marker of myocardial injury, not a standalone diagnosis. Troponin elevation can also occur in myocarditis, acute heart failure, pulmonary embolism, sepsis, renal failure, and stress cardiomyopathy (Takotsubo syndrome). Clinical context, symptom pattern, and ECG findings always need to be interpreted together.
Symptoms: What Each Type Feels Like
STEMI symptoms tend to be dramatic and unmistakable. Most patients describe a sudden, crushing chest pain that radiates to the left arm, jaw, or neck. Profuse sweating, nausea, and a profound sense of impending doom are common. The onset is typically abrupt and severe. These patients generally know something is catastrophically wrong.
NSTEMI symptoms are often more subtle and insidious. Chest pressure rather than crushing pain. Shortness of breath with minimal exertion. Fatigue that does not improve with rest. Some patients, particularly those with diabetes, elderly individuals, and women, can experience what we call a silent NSTEMI with no chest pain whatsoever. This is one of the main reasons NSTEMI goes undetected or gets delayed, sometimes for hours or even days.
Women more commonly present with jaw pain, back pain, nausea, and extreme fatigue without the classic chest pressure pattern. This atypical presentation increases the risk of misdiagnosis or delayed evaluation. If you are in a high-risk group and something feels wrong, do not wait for textbook chest pain before calling for help.
Mortality and Outcomes: The Real Numbers
Here is where most people get confused, and I want to address it directly.
In-hospital mortality for STEMI in the modern primary PCI era runs approximately 4 to 7 percent depending on the registry and patient population studied. The GRACE registry reported in-hospital mortality of 4.6 percent for STEMI. The OPERA registry data showed 7.8 percent, reflecting a higher-risk cohort. For NSTEMI, in-hospital mortality is generally lower, ranging from approximately 2 to 5 percent in contemporary registries.
Based on those numbers alone, you might conclude NSTEMI is the safer diagnosis. That conclusion would be wrong if you stop at in-hospital data.
Long-term outcomes tell a different story. A landmark analysis published in Circulation followed over 4,000 patients undergoing cardiac catheterization for STEMI and NSTEMI and found that while STEMI carried significantly higher adjusted mortality risk in the first two months after the event, NSTEMI carried a higher adjusted mortality risk after that initial period. GRACE registry data consistently shows higher post-discharge mortality in NSTEMI versus STEMI patients in the months following hospital discharge.
Why does NSTEMI carry worse long-term mortality? Because NSTEMI patients tend to be older, carry more comorbidities including chronic kidney disease, type 2 diabetes, and prior coronary disease, and often have diffuse multi-vessel atherosclerosis rather than a single culprit lesion. The acute event is less dramatic, but the underlying disease burden is often more advanced.
This is why the GRACE score (Global Registry of Acute Coronary Events) is the most widely validated risk stratification tool for NSTEMI. It incorporates eight variables: age, heart rate, systolic blood pressure, serum creatinine, Killip class (a measure of heart failure severity), ST deviation on ECG, elevated cardiac markers, and history of cardiac arrest at presentation. The resulting score stratifies patients into very high risk (angiography within 2 hours), high risk (within 24 hours), and intermediate risk (within 72 hours). A GRACE 2.0 score above 140 is considered high risk and is a guideline-recommended threshold for early invasive strategy.
I never dismiss NSTEMI as just the smaller heart attack. The acute event may be less dramatic, but the long-term trajectory demands the same level of clinical attention.
Treatment: STEMI vs NSTEMI
For STEMI, there is one goal: open the artery as fast as possible. The guideline target is a door-to-balloon time of under 90 minutes from hospital arrival. Primary percutaneous coronary intervention (PCI), meaning angioplasty with coronary stenting, is the standard of care. If PCI-capable facilities are not available within 120 minutes of first medical contact, fibrinolytic (clot-busting) therapy should be administered instead, followed by transfer to a PCI-capable center.
For NSTEMI, the approach is risk-stratified based on the GRACE score and clinical features. All patients receive dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor such as ticagrelor or clopidogrel), anticoagulation with heparin or low-molecular-weight heparin, a high-intensity statin, a beta-blocker, and an ACE inhibitor or ARB when indicated.
The timing of cardiac catheterization for NSTEMI depends entirely on risk category. Very high-risk patients, meaning those with refractory chest pain, hemodynamic instability, severe arrhythmias, or acute heart failure, go to the cath lab immediately regardless of time of day. High-risk patients with a GRACE score above 140 or dynamic ECG changes go within 24 hours. Intermediate-risk patients can be evaluated over 24 to 72 hours.
If the ejection fraction drops below 40 percent after either type of myocardial infarction, additional evidence-based therapies are indicated: ACE inhibitors or ARBs, mineralocorticoid receptor antagonists, SGLT2 inhibitors, and appropriately dosed beta-blockers. These therapies reduce the risk of subsequent heart failure hospitalization and cardiovascular death.
Frequently Asked Questions
Which is worse, STEMI or NSTEMI?
In the short term, STEMI is the more dangerous diagnosis. The complete artery blockage destroys a larger territory of heart muscle quickly, and in-hospital mortality runs approximately 4 to 7 percent in the modern cath lab era. However, NSTEMI patients frequently have worse outcomes over the following six to twelve months because they tend to be older, have more comorbidities, and carry more extensive underlying coronary artery disease. GRACE registry data confirms higher post-discharge mortality in NSTEMI compared to STEMI. Both diagnoses are serious emergencies. Neither should be minimized.
Can NSTEMI become a STEMI?
Yes, and this is one of the most important reasons NSTEMI patients require close in-hospital monitoring and timely catheterization. A partial occlusion can progress to a complete occlusion at any moment, converting an NSTEMI into a STEMI. This escalation significantly increases the risk of death, cardiogenic shock, and major arrhythmias. Delaying evaluation and treatment for NSTEMI is not a neutral decision. Every hour counts.
How long can you have an NSTEMI without knowing?
It depends heavily on the individual. Diabetics, elderly patients, and women are the most likely to experience a silent NSTEMI with minimal or no chest pain due to autonomic neuropathy and altered pain perception. In some cases, the diagnosis is only made when a routine ECG or troponin is ordered for another reason and the results reveal a recent myocardial injury. The ischemic event can go unrecognized for hours to days in these populations. If you are in a high-risk group and experience unusual fatigue, unexplained shortness of breath, jaw pain, or back discomfort, seek medical evaluation promptly. Do not wait for crushing chest pain to be the signal.
What is the difference between STEMI and NSTEMI on an ECG?
A STEMI produces ST elevation of at least 1mm in two or more contiguous limb leads, or at least 2mm in two or more contiguous chest leads. A new left bundle branch block is also treated as a STEMI equivalent and triggers immediate cath lab activation. An NSTEMI typically shows ST depression, T-wave inversions, or a completely normal ECG. The ECG alone cannot diagnose NSTEMI. Elevated troponin on serial testing is what separates NSTEMI from unstable angina when the ECG is non-diagnostic. Never discharge a symptomatic patient based on a normal ECG without serial troponin measurements.
Below is one of my best-performing videos on YouTube, where I discuss the treatment of STEMI versus NSTEMI
Feel free to shoot me questions on here or on YouTube.
Relevant Clinical Studies
The GRACE (Global Registry of Acute Coronary Events) registry, which enrolled over 100,000 patients across multiple countries, established the prognostic model now universally used to guide the timing of angiography in NSTEMI patients. It remains one of the most cited tools in interventional cardiology and is incorporated into both ESC and ACC/AHA guidelines.
A Circulation analysis comparing long-term outcomes in STEMI versus NSTEMI patients undergoing cardiac catheterization found a higher adjusted mortality risk for STEMI in the first two months, but a lower adjusted mortality risk for STEMI beyond that two-month mark, confirming that NSTEMI carries a worse long-term trajectory in many patient populations.
The ISIS-2 trial, published in The Lancet, was foundational in establishing aspirin as a cornerstone of acute MI therapy, demonstrating a significant reduction in 35-day vascular mortality when aspirin was given at the time of presentation.
A study published in the New England Journal of Medicine comparing primary angioplasty versus fibrinolysis in STEMI demonstrated superior outcomes with timely PCI at experienced centers, which cemented primary PCI as the preferred reperfusion strategy when it can be delivered within the appropriate time window.
Final Words
STEMI and NSTEMI are both life-threatening emergencies that require rapid, evidence-based intervention. The distinction between them determines how fast you activate the cath lab, how you sequence your risk stratification tools, and how you structure downstream therapy. Understanding these differences is not academic. It is the foundation of acute coronary syndrome management.
If you or someone near you experiences chest pain, jaw pain, arm pain, unusual fatigue, or unexplained shortness of breath, do not wait. Call 911 immediately. The difference between a good outcome and an irreversible one is often measured in minutes.
References
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















