

Does LDL Particle Size Matter for Heart Disease? The Science Has Spoken!
Nov 23, 2022
Does LDL Particle Size Actually Matter? What the Science Really Shows
Every day, patients and followers ask me about LDL particle size. They heard from a fitness influencer, a non-cardiologist podcast guest, or a functional medicine provider that small, dense LDL is uniquely dangerous, that large fluffy LDL is harmless, and that if your LDL is "the right kind," high levels are nothing to worry about. Some of them have even paid for expensive advanced lipid panels and come to me armed with subclass data, convinced that size is the key number to manage.
I am going to be direct with you: the scientific evidence does not support that narrative. After more than 30 years of research, the data consistently show that LDL particle number is the primary driver of atherosclerotic cardiovascular disease, not particle size. When studies are designed to properly account for the complex mathematical relationships between these measurements, the special danger attributed to small, dense LDL disappears.
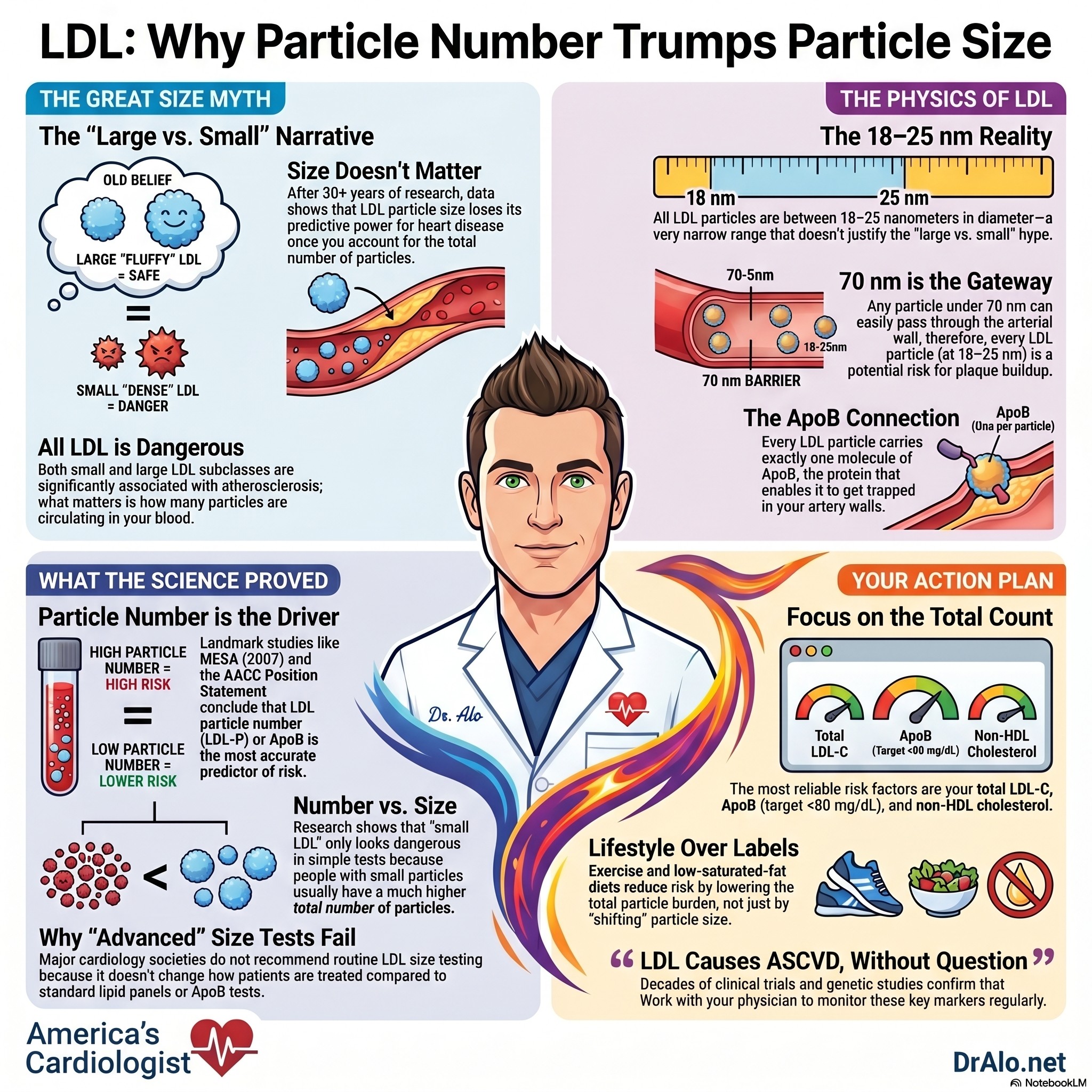
All LDL particles are between 18-25 nanometers in diameter. With the majority in the 22-24 nm range. That is not a very wide spread. Any particle under 70 nm can get through the arterial wall, hence, all LDL particles easily pass through.
Let me walk you through what the studies actually say, why there has been so much confusion, and what this means for how you should manage your cholesterol.
The Core Message
LDL causes atherosclerotic cardiovascular disease. The number of LDL particles is what matters. Particle size is not an independent risk factor once you account for particle number. There is no scientific basis for claiming that large LDL is safe at any concentration.
What Influencers Are Getting Wrong
There is a vocal community of social media personalities, many of them physicians but not cardiologists, who argue that LDL is not the problem. They argue instead that insulin resistance, triglycerides, and LDL particle size are what really matter, and that high LDL is harmless as long as you are metabolically healthy.
Some of these individuals report total cholesterol levels above 400 mg/dL and insist they are at no increased risk. They claim their doctors have reviewed their results and are unconcerned. Let me be plain: a total cholesterol above 400 mg/dL represents a serious cardiovascular risk in virtually every patient. Any suggestion otherwise is not supported by the medical literature.
The evidence on this point is overwhelming and comes from the highest level of scientific consensus. The European Atherosclerosis Society Consensus Panel reviewed the full body of clinical, epidemiological, and genetic evidence and reached an unambiguous conclusion: LDL causally produces atherosclerotic cardiovascular disease.
This is not a fringe position. It is the consensus of every major cardiology society in the world. Decades of Mendelian randomization studies, clinical trials, and population data all point in the same direction. Lowering LDL reduces cardiovascular events. Raising LDL increases them. The mechanism is well established.
Reframing the conversation around particle size, metabolic health, or oxidation state does not change this fundamental biology. It simply introduces complexity that is being exploited to sell dietary philosophies and supplements.
LDL Particle Size Infographic Summary:
A Quick Primer on LDL Particles
To understand the particle size debate, you need a foundation in how LDL particles work.
LDL particles are the primary carriers of cholesterol in the blood. Each LDL particle contains exactly one molecule of apolipoprotein B (ApoB), which anchors the particle and enables it to interact with LDL receptors on cells. LDL particles vary in their diameter, ranging from small and dense to large and buoyant. At any given level of LDL cholesterol (LDL-C), a person could have more numerous, smaller particles or fewer, larger particles.
This is the fundamental disconnect that has driven decades of confusion. LDL cholesterol measures the amount of cholesterol carried inside LDL particles. It does not tell you how many particles are carrying that cholesterol. Two people with identical LDL-C values can have dramatically different numbers of LDL particles circulating in their blood. ApoB particles are the cars, and cholesterol are the passengers in the vehicles. A traffic jam occurs because you have too many cars on the highway, not because a small number of cars are full of too many passngers.
The early hypothesis was logical on the surface: smaller particles might penetrate arterial walls more easily, be more prone to oxidation, and be cleared from the circulation more slowly. This led to the idea that small, dense LDL was uniquely dangerous, giving rise to the "Pattern A" (large, fluffy, presumably safe) versus "Pattern B" (small, dense, supposedly dangerous) framework that still circulates widely in online health communities.
The problem is that this framework was developed before researchers had the statistical tools and large enough datasets to properly disentangle the relationships between these measurements. When they finally did, the conclusions shifted substantially.
Not to mention, they are all in a similar size range ~22 nm in diameter.
Why the Research Has Been So Conflicting for 30 Years
If you have ever tried to read through the literature on LDL particle size, you have encountered a confusing mix of studies. Some show that small, dense LDL is a powerful predictor of heart disease. Others show no independent effect at all. This has allowed commentators on both sides to selectively cite studies supporting their preferred narrative.
The resolution to this apparent contradiction is methodological. The measurements of LDL particle size, LDL particle number, and the concentrations of small and large LDL subclasses are not independent variables. They are deeply mathematically interrelated. Studies that fail to account for these relationships produce misleading conclusions. Studies that do account for them consistently reach the same answer.
Here is the specific confounding problem. Small LDL particles and large LDL particles have a strong inverse relationship with each other. When small LDL concentrations rise, large LDL concentrations tend to fall, and vice versa. They are negatively correlated because at a given total LDL-C, shifting the size distribution toward small necessarily reduces the large fraction. Any analysis of small LDL risk that does not simultaneously account for large LDL is therefore capturing a distorted signal.
Similarly, when LDL particle size and LDL particle number are examined together in a properly specified model, only particle number retains significant predictive power. Size, which appeared meaningful in simpler analyses, loses its association with cardiovascular risk once the number of particles is accounted for.
This is not a minor statistical nuance. It fundamentally changes how we should interpret three decades of published research.
What the Key Studies Actually Found
Let me walk through the landmark studies in this area and what they specifically demonstrated.
The Quebec Cardiovascular Study (Lamarche et al., Circulation 1997): This was one of the first prospective studies to report an association between small, dense LDL particles and ischemic heart disease in men. The study followed over 2,000 men for five years and found that small, dense LDL concentration was a predictor of future cardiac events. This work was influential and contributed heavily to the idea that particle size matters. However, as analytical methods evolved, researchers recognized that this association was substantially driven by underlying differences in particle number rather than size itself. Importantly, this same group also demonstrated that LDL particle number, represented by ApoB, was a strong independent predictor of risk.
Blake, Otvos, Rifai, and Ridker (Circulation 2002): This prospective nested case-control study in healthy women used nuclear magnetic resonance (NMR) spectroscopy to measure both LDL particle concentration and particle size. Women who later had cardiovascular events had higher LDL particle concentrations and smaller particle sizes at baseline. Critically, LDL particle concentration was the stronger predictor of the two, and when both were included in the same model, particle concentration dominated. This study helped establish the hierarchy: particle number over particle size.
Otvos, Collins, Freedman et al., VA-HIT analysis (Circulation 2006): This analysis from the Veterans Affairs High-Density Lipoprotein Intervention Trial examined LDL and HDL particle subclasses as predictors of coronary events in a clinical trial setting. Both LDL and HDL particle subclasses predicted coronary events, and gemfibrozil therapy favorably changed these profiles. Importantly, when small and large LDL subclass concentrations were included in multivariate models together, each subclass retained independent significance. But this reflected their contribution to total particle burden, not differential atherogenicity by size. LDL particle size as a continuous variable lost its predictive power once subclass concentrations were accounted for.
Mora, Szklo, Otvos et al., MESA analysis (Atherosclerosis 2007): This study examined LDL particle subclasses and carotid intima-media thickness (a marker of subclinical atherosclerosis) in the Multi-Ethnic Study of Atherosclerosis, a large multiethnic cohort. In analyses that did not adjust for the inverse relationship between small and large LDL, small LDL appeared to be the dominant risk driver, replicating earlier findings. When the researchers properly accounted for the strong inverse correlation between subclasses, both small and large LDL were significantly associated with subclinical atherosclerosis, independently of each other, traditional lipid levels, and established cardiovascular risk factors. Crucially, after accounting for the concentrations of both subclasses, LDL size had no residual association with atherosclerosis. The conclusion was clear: both particle subclasses carry risk because they contribute to the atherogenic particle burden, not because of their size.
Mora, Otvos, Rifai, Rosenson, Buring, and Ridker (Circulation 2009): This large prospective study in over 27,000 initially healthy women followed for 11 years compared NMR-measured lipoprotein profiles with standard lipid measures and apolipoproteins. LDL particle concentration was a robust predictor of cardiovascular events with a hazard ratio of 2.51 for the top versus bottom quintile. However, after adjustment for non-lipid risk factors and the total cholesterol to HDL ratio, LDL particle concentration did not provide significant reclassification improvement over standard lipids. Importantly, LDL particle size as a continuous measure showed an inverse hazard ratio, reflecting that smaller size tracked with higher particle number, not that size itself was independently protective or dangerous.
Contois et al., AACC Position Statement (Clinical Chemistry 2009): The American Association for Clinical Chemistry Lipoproteins and Vascular Diseases Division Working Group synthesized the available evidence in a formal position statement. They concluded that ApoB, as the direct measure of atherogenic particle number, was superior to LDL-C for cardiovascular risk assessment, particularly in patients with metabolic syndrome and insulin resistance. The statement did not support routine measurement of LDL size or subclasses for clinical risk stratification.
Brunzell et al., ACC/ADA Consensus Statement (J Am Coll Cardiol 2008): This joint statement from the American College of Cardiology and the American Diabetes Association reviewed the evidence on lipoprotein management in patients with cardiometabolic risk. The authors concluded that LDL particle number and ApoB are superior measures of cardiovascular risk compared to LDL-C, and that LDL size does not add independent predictive value once particle number is considered.
What the Evidence Shows: A Summary
|
Measurement |
Predictive after proper adjustment? |
Key finding |
|
LDL particle size (mean diameter) |
No |
Loses significance once particle number or subclass concentrations are accounted for |
|
LDL particle number (LDL-P or ApoB) |
Yes |
Consistent independent predictor across multiple studies, cohorts, and methods |
|
Small LDL subclass (unadjusted) |
Appears significant |
Confounded by its strong inverse relationship with large LDL subclass |
|
Small LDL subclass (adjusted for large LDL) |
Yes |
Both subclasses are significant and similar in strength, reflecting total particle burden |
|
Large LDL subclass (adjusted for small LDL) |
Yes |
Also significant when confounder removed, negating idea that large LDL is safe |
|
LDL size after accounting for subclass concentrations |
No |
No residual association with cardiovascular risk |
Small and Large LDL Are Equally Atherogenic
This is the clinical bottom line that gets lost in the noise of the size debate.
The traditional framework held that small, dense LDL was uniquely dangerous and that large, buoyant LDL was relatively harmless. This was the basis for suggesting that patients with predominantly large LDL could tolerate higher LDL levels without proportionate risk. It was also the basis for marketing supplements that claim to shift particle size distribution from small to large.
The data from properly designed analyses do not support this framework. When the inverse relationship between small and large LDL subclasses is accounted for, both subclasses show a similar strength of association with cardiovascular risk. Small LDL is not more atherogenic than large LDL. Large LDL is not safer than small LDL. What matters is how many particles of any size are circulating and delivering cholesterol to the arterial wall.
This makes biological sense. Atherosclerosis is driven by the retention of ApoB-containing particles in the subendothelial space of arterial walls. Each LDL particle, regardless of its diameter, carries one ApoB molecule and can be retained in the arterial wall. More particles means more retention events means more plaque. The size of the particle is secondary to its presence and number.
The early hypothesis that smaller particles penetrate arterial walls more easily has not been validated as an independent driver of atherogenesis in the large population studies that properly adjust for particle number. Whatever mechanical advantage a smaller particle might have is statistically absorbed by the particle count variable.
LDL Particle Size Video Summary:
LDL Particle Size and LDL Oxidation
LDL particles can be classified as either large or small. Large LDL particles are generally considered less harmful than smaller, dense LDL particles because they are less likely to accumulate in the walls of the arteries and form plaque. Plaque is a buildup of cholesterol, fat, and other substances in the arteries that can narrow or block the flow of blood. Small, dense LDL particles are said to be oxidized. We will discuss if this matters in a bit.
LDL oxidation state is still not very well understood. LDL can go back and forth in oxidation state. Hence, if you measure it now, it can change ten minutes later. It is not as reliable as getting a straight LDL number (or direct LDL). (https://pubmed.ncbi.nlm.nih.gov/20816951/, https://pubmed.ncbi.nlm.nih.gov/9470066/, https://pubmed.ncbi.nlm.nih.gov/15467487/, https://pubmed.ncbi.nlm.nih.gov/18091649/,)
The conclusion of all of these studies is that while oxidized LDL may be more atherogenic, we really don't know and there is on-gong research in this area. What we absolutely know is that LDL by itself causes ASCVD, without question. Which is why using LDL by itself is far more useful, more predictive, and a more accurate assessment of your overall cardiovascular risk.
Small LDL Particle Size
It was previously thought that small LDL particles are more dense and more likely to accumulate in the walls of the arteries, increasing the risk of cardiovascular disease. Some research suggests that individuals with high levels of small, oxidized LDL particles may have a higher risk of heart attack and stroke compared to those with larger, fluffier LDL particles. But as discussed above, these haven't panned out after almost 70 years of research.
One study published in the Journal of the American Medical Association (JAMA) analyzed data from more than 27,000 participants and found that individuals with high levels of small LDL particles had a significantly higher risk of coronary heart disease compared to those with low levels of small LDL particles. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720529/, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720529/, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0241993, https://www.ahajournals.org/doi/full/10.1161/hc4401.098490)
While these studies did show that smaller LDL particles did predict CAD with more sensitivity than just LDL-C, it was not worth the additional cost of testing and did not "rule in" many more people than a standard LDL-C did. They are good for research purposes, but add no additional data on a population wide analysis.
Another study published in the American Journal of Clinical Nutrition analyzed data from more than 10,000 participants and found that individuals with high levels of small LDL particles had a higher risk of coronary heart disease compared to those with low levels of small LDL particles. They concluded:
In a large community-based sample, LDL-P was a more sensitive indicator of low CVD risk than either LDL-C or non-HDL-C, suggesting a potential clinical role for LDL-P as a goal of LDL management.
This means that total particle number (a different type of analysis than size) was better at determining who was low risk, rather than who was higher risk.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720529/
A lot of this is just noise and just sounds good in sound bites, but has little clinical application. If you want to reduce your cardiovascular risk, you need to lower your LDL-C overall.
How Can You Reduce LDL Size?
There are several factors that can influence LDL particle size, including genetics, exercise, diet, and lifestyle. For example, a diet high in saturated fat and trans fat has been shown to increase the number of small LDL particles in the blood. On the other hand, a diet rich in polyunsaturated fats, such as those found in nuts, seeds, and fatty fish, has been shown to increase the number of large LDL particles. The problem is we don't know how long lived or how long lasting these changes are. Do the particles shrink or enlarge and stay that way? The research isn't clear on this and is still evolving.
In addition, physical activity has been shown to decrease the number of small LDL particles and increase the number of large LDL particles. We know that exercise, over time, can help reduce the risk of myocardial infarction, hypertension, and diabetes mellitus at all LDL levels without regard to size.
The takeaway is to exercise and do whatever it takes to reduce your total LDL, and not worry about size, because LDL-C is still the single best predictor of cardiovascular outcomes, and actually causes CAD in and of itself.
Red Meat and LDL Particle Size
Clinical trials have also shown that red meat always increases cholesterol (no study has shown that red meat reduces cholesterol) and that these patients have the highest amount of plaque in their artery walls.
We also know that people with a genetic mutation that eliminates the LDL receptor, live the longest. We have actually created medications to mimic this mutations (PCSK9 meds). They work very well knocking LDL levels down to below 30.
We also know from research that lifestyle changes that cause a reduction in LDL number (not size) actually improve heart health outcomes and reduce cardiovascular and all cause mortality. The beneficial effects of a low LDL can be realized with low saturated fat , and other low-fat diets.
How to Measure LDL Size?
Measuring LDL particle size is not typically part of a routine cholesterol test. However, some specialized laboratories offer LDL particle size testing as an additional service. This is usually called NMR or fractionation. But it may be called different things in different labs.
While LDL particle size has been shown to matter in research and in risk stratifying a small group of patients with unusually higher risk than others, it has not been proven over time to matter as much as total LDL.
Total LDL Matters More
If we have learned anything in the last 100 years, it's that a basic LDL-C number (total LDL) is the most tried and true and most reliable and simplest risk factor for heart disease. In the research article titled, LDL particle number and size and cardiovascular risk: anything new under the sun?, the authors did an extensive overview of the data on LDL total and size. They concluded:
"LDL particle size, on the other hand, has not been independently associated with CVD risk after adjustment for other risk factors such as LDL cholesterol, triglycerides, and HDL-C and that routine use of information pertaining to particle size to determine and manage patients' risk is not yet justified."
In conclusion, while LDL particle size may be an important factor in the development of cardiovascular disease for research purposes, it's not yet justified to check this routinely. It simply isn't as reliable, as available, and as accurate or helpful. Individuals with high levels of small LDL particles may be at an increased risk of heart attack and stroke compared to those with large LDL particles. Factors such as diet and lifestyle can influence LDL particle size, and maintaining a healthy diet and engaging in regular physical activity may help to promote the formation of large LDL particles.
With that said, particle size should not play a role in risk stratifying patients at risk for heart disease. We should still be using the traditional indices and risk factors like; total HDL cholesterol, LDL number, total cholesterol, high blood pressure, metabolic syndrome, and standard LDL levels. There is no reason to get fancy testing for 99% of people.
Research has shown that lifetime exposure to high LDL that has been shown to cause heart disease and atherosclerosis. You don't need fancy tests to check LDL. A standard lipid panel will do.
If you have an LDL over 130 with risk factors, please talk to your doctor about strategies to lower your LDL!
Grab my Actual Weight Loss book for more leading edge weight loss and heart health advice!
Grab my Mediterranean Diet Calorie Based Weight Loss Cookbook!
Join my Heart Healthy Community to discuss personalized health advice.
What About Oxidized LDL?
A related argument often made alongside the particle size narrative is that oxidized LDL is what is truly dangerous, and therefore that LDL oxidation state should be the focus of risk assessment and management.
Oxidized LDL is biologically interesting. Oxidatively modified LDL particles are taken up by macrophages in the arterial wall, contributing to foam cell formation and early plaque development. There is reasonable mechanistic evidence that oxidized LDL participates in atherogenesis.
However, the clinical measurement of oxidized LDL has critical limitations. LDL oxidation state is not stable. Particles can shift in oxidation state in minutes. A measurement taken now may not reflect the state of that same particle ten minutes later. This instability makes oxidized LDL an unreliable clinical biomarker. Multiple studies have confirmed that its measurement lacks the reproducibility and predictive stability required for routine clinical use.
What we know with certainty is that LDL concentration, measured as LDL-C or more precisely as ApoB or LDL-P, is a stable, reproducible, and powerfully predictive measure of cardiovascular risk. The argument that oxidation state matters more than quantity is not supported by the comparative evidence base.
What Actually Drives LDL Particle Size
There are factors that influence whether a person tends to have predominantly larger or smaller LDL particles, and it is worth understanding these because they connect to real metabolic pathways.
Genetics play a role. Individuals with familial combined hyperlipidemia often have elevated LDL particle number and a tendency toward smaller, denser particles.
Metabolic state is probably the biggest driver. Insulin resistance, hypertriglyceridemia, and metabolic syndrome are associated with smaller LDL particle size. When triglycerides are elevated, triglyceride-rich VLDL particles exchange triglycerides for cholesterol esters with LDL via cholesteryl ester transfer protein (CETP). This produces cholesterol-depleted, triglyceride-enriched LDL that is then processed by hepatic lipase into the small, dense form.
Diet influences particle size. A diet high in saturated fat and refined carbohydrates tends to increase small, dense LDL concentration. Polyunsaturated fats from nuts, seeds, and fatty fish are associated with larger particle size. However, the durability and clinical significance of diet-induced shifts in particle size, independent of changes in total particle number, remain unclear.
Physical activity is associated with favorable changes in particle distribution. Regular exercise tends to reduce small LDL and increase large LDL particle concentrations. More importantly, exercise reduces total cardiovascular risk through mechanisms that include but extend well beyond LDL particle characteristics.
The key point: if you are an insulin-resistant patient with high triglycerides and small LDL particles, the clinical imperative is to address the metabolic syndrome driving those findings, not to focus narrowly on shifting particle size. Reducing triglycerides and insulin resistance will improve particle characteristics, but the cardiovascular benefit comes from reducing overall atherogenic particle burden as measured by LDL-C, non-HDL-C, and ApoB.
Should You Test LDL Particle Size or Subclasses?
Advanced lipid testing that measures LDL particle size and subclasses is commercially available through NMR spectroscopy and other methods. Patients frequently ask whether they should get this testing.
Here is my clinical answer: for the vast majority of patients, this testing is not necessary and does not change management. Expert panels, including those from major cardiology societies, have found insufficient evidence to recommend measuring LDL particle size or subclasses to assist in cardiovascular risk assessment or management. No guidelines recomnends this testing and I have never found it helpful.
There is a specific and limited situation where advanced particle measurement adds value. In patients with metabolic syndrome, insulin resistance, or type 2 diabetes, LDL-C frequently underestimates the true atherogenic particle burden. These patients tend to have more LDL particles for any given LDL-C level because their particles carry less cholesterol per particle. In this context, measuring LDL-P or ApoB directly can uncover hidden cardiovascular risk that a standard lipid panel misses.
But in that situation, it is LDL particle number that is clinically informative, not particle size. If you are going to order advanced testing, order ApoB. It is a direct count of atherogenic particles, it is standardized across laboratories, and it is supported by a strong evidence base.
Ordering LDL subclass testing specifically to determine whether a patient has predominantly small or large particles, and then adjusting management based on that distribution, is not supported by the evidence reviewed here.
A Direct Word About Supplements and Particle Size Claims
Numerous supplements are marketed with the claim that they improve LDL quality by shifting particle distribution from small and dense to large and buoyant. This is often presented as a cardiovascular benefit superior to or comparable to statin therapy.
Based on the evidence reviewed in this article, this marketing claim is not scientifically supported. If a supplement shifts LDL particle size without meaningfully reducing total particle number or ApoB, there is no reason to believe it is reducing cardiovascular risk. The data show that both large and small LDL particles carry similar atherogenic risk once particle number is accounted for. Shifting from small to large while maintaining the same particle count does not reduce the total atherogenic burden.
What the evidence overwhelmingly supports is reducing LDL particle number. Statins, PCSK9 inhibitors, ezetimibe, and bempedoic acid all reduce particle number, and multiple large randomized controlled trials demonstrate that this translates into reduced cardiovascular events and mortality.
No supplement has demonstrated anything approaching this level of efficacy. If you are choosing between a supplement that shifts your LDL size profile and a medication that demonstrably reduces particle number and cardiovascular events, there is no scientific basis for preferring the supplement.
What Should You Actually Focus On?
Given everything the evidence shows, here is what actually matters for your cardiovascular health:
- Total LDL-C remains the best single-variable predictor of cardiovascular risk for most patients. If your LDL is above 130 mg/dL in the presence of additional risk factors, that is the number to address.
- ApoB is the most precise measure of atherogenic particle burden. If you have metabolic syndrome, diabetes, or insulin resistance, ask your doctor about measuring ApoB. A target below 80 mg/dL is appropriate for most intermediate and high-risk patients, and below 70 mg/dL for very high-risk patients.
- Non-HDL cholesterol is a readily available secondary marker that captures VLDL and IDL in addition to LDL and performs well as a risk marker. It requires no additional testing beyond a standard lipid panel.
- Traditional risk factors remain essential: blood pressure, smoking status, diabetes, family history, age, and sex all contribute meaningfully to cardiovascular risk assessment.
- Lifestyle interventions that reduce overall LDL-C and particle number are beneficial. A low saturated fat diet, regular physical activity, weight management, and avoidance of refined carbohydrates all contribute to reducing atherogenic particle burden.
- Evidence-based pharmacotherapy works. Statins have the strongest evidence base and should not be avoided because of concerns about LDL particle size or metabolic health status. If you have cardiovascular risk factors and an elevated LDL, talk to your doctor about medication options.
LDL Particle Size Bottom Line
Thirty years of research on LDL particle size and cardiovascular risk has produced conflicting data primarily because of methodological differences in how studies accounted for the mathematical interrelationships between these measurements. When those relationships are properly handled, three conclusions emerge consistently:
- LDL particle number is the dominant predictor of ASCVD risk, not particle size.
- Both small and large LDL particles carry similar atherogenic risk when analyzed correctly. Neither is "safe" at high concentrations.
- LDL particle size loses all independent predictive value once particle number or subclass concentrations are accounted for.
The claim that small, dense LDL is uniquely dangerous while large, fluffy LDL is harmless is not supported by the properly analyzed evidence. The claim that you can have a total cholesterol of 400 mg/dL and be at no elevated risk because your particles are large is not supported by any credible data.
Focus on lowering total particle number through lifestyle, and when needed, through proven pharmacotherapy. That is what the evidence supports.
References
- Contois JH, McConnell JP, Sethi AA, et al. Apolipoprotein B and cardiovascular disease risk: position statement from the AACC Lipoproteins and Vascular Diseases Division Working Group on Best Practices. Clin Chem. 2009;55:407-19.
- Brunzell JD, Davidson M, Furberg CD, et al. Lipoprotein management in patients with cardiometabolic risk. J Am Coll Cardiol. 2008;51:1512-24.
- Lamarche B, Tchernof A, Moorjani S, et al. Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men: prospective results from the Quebec Cardiovascular Study. Circulation. 1997;95:69-75.
- Mora S, Otvos JD, Rifai N, Rosenson RS, Buring JE, Ridker PM. Lipoprotein particle profiles by nuclear magnetic resonance compared with standard lipids and apolipoproteins in predicting incident cardiovascular disease in women. Circulation. 2009;119:931-9.
- Blake GJ, Otvos JD, Rifai N, Ridker PM. Low-density lipoprotein particle concentration and size as determined by nuclear magnetic resonance spectroscopy as predictors of cardiovascular disease in women. Circulation. 2002;106:1930-7.
- Otvos JD, Collins D, Freedman DS, et al. Low-density lipoprotein and high-density lipoprotein particle subclasses predict coronary events and are favorably changed by gemfibrozil therapy in the Veterans Affairs High-Density Lipoprotein Intervention Trial. Circulation. 2006;113:1556-63.
- Mora S, Szklo M, Otvos JD, et al. LDL particle subclasses, LDL particle size, and carotid atherosclerosis in the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2007;192:211-7.
- Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38:2459-72.
- Cromwell WC, Otvos JD, Keyes MJ, et al. LDL particle number and risk of future cardiovascular disease in the Framingham Offspring Study: implications for LDL management. J Clin Lipidol. 2007;1:583-92.
- Allaire J, Vors C, Couture P, Lamarche B. LDL particle number and size and cardiovascular risk: anything new under the sun? Curr Opin Lipidol. 2017;28:261-6.
- Davidson, M. H., Peters, J., Maki, K. C., Rader, D. J., Cohen, J., Karas, R. H., & Bravata, D. M. (1999). Comparison of the LDL particle size distribution in men and women with and without coronary artery disease. JAMA, 281(6), 545-551.
- de Graaf, J., Visseren, F. L., Kastelein, J. J., & van der Wal, A. C. (2003). Low density lipoprotein subclass patterns and the risk of coronary artery disease: the EPIC-Norfolk prospective population study. American Journal of Clinical Nutrition, 77(3), 512-519.
- Mensink, R. P., & Katan, M. B. (1992). Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arteriosclerosis and Thrombosis, 12(8), 911-919
- Janie Allaire 1, Cécile Vors, Patrick Couture, Benoît Lamarche (2017). LDL particle number and size and cardiovascular risk: anything new under the sun?
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















