

What Is Lipoprotein a?
Apr 10, 2025
Lipoprotein(a): The "Hidden" Genetic Cholesterol That Could Be Putting You at Risk
What is lipoprotein a and what can we do about it? One of the most common topics and questions I get at medical conferences is, "Can you tell us more about lipoprotein little a?"
What is my life expectancy with lipoprotein a?
Lipoprotein little a, commonly known as Lp(a) or LPa. It is a type of lipoprotein that carries cholesterol and other fats through the bloodstream. Lp(a) is considered one of the most dangerous and potent risk factors for cardiovascular disease, stroke, aortic stenosis, peripheral artery disease, heart failure, and other related conditions.
Let's dive deep and discuss the structure, function, and medical significance of Lp(a), including its effects on health and how it can be managed and treated.
Life Expectancy With High Lipoprotein(a): What the Research Says
The most compelling data comes from a massive Danish study that followed nearly 70,000 people over many years. The researchers found that people with very high Lp(a) levels (above 93 mg/dL) lived about 1.2 years less on average than those with lower levels. That might not sound like a lot, but consider that this is an average across an entire population — for individuals who actually suffer a heart attack or stroke because of their elevated Lp(a), the impact is obviously much greater.
The numbers break down like this: people with the highest Lp(a) levels had a 50% greater risk of dying from cardiovascular disease and a 20% greater risk of dying from any cause compared to those with the lowest levels.
How Much Does High Lp(a) Shorten Your Life? The Data
A separate study used a clever genetic technique called Mendelian randomization, essentially using people's DNA as a natural experiment, to confirm these findings. Using data from the UK Biobank, researchers showed that for every 50 mg/dL increase in genetically predicted Lp(a), the odds of achieving exceptional longevity (living into the top 1% of survival for your birth year) dropped by 8–11%.
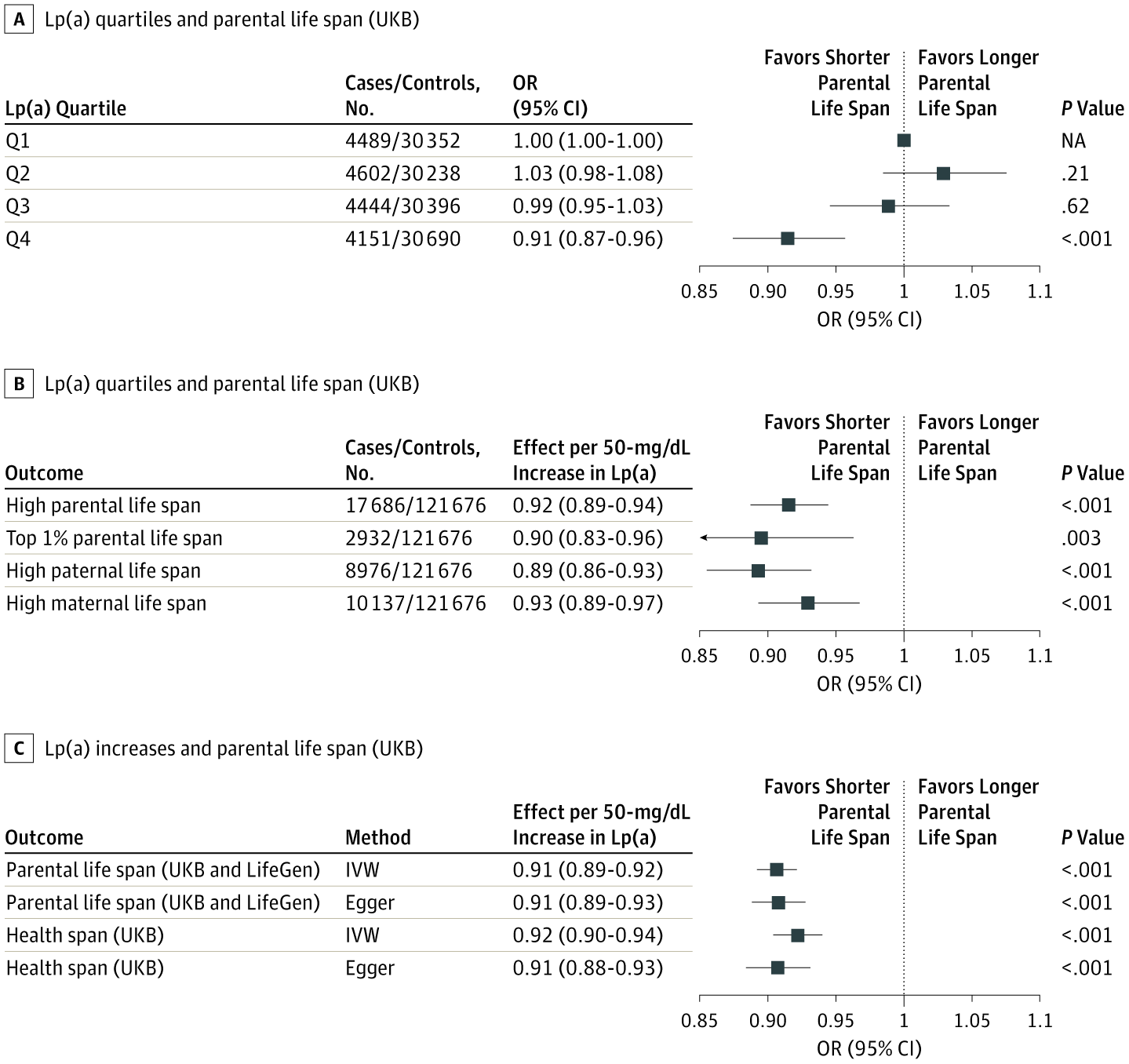
Figure 1. Association Between the Lp(a) Genetic Instruments, Parental Life Span, and Health Span
A, High parental life span in participants of the UK Biobank (UKB) separated into quartiles of the Lp(a) weighted genetic risk score (wGRS) from Burgess et al.16 B, High parental life span, top 1% parental life span, high paternal life span, and high maternal life span associated with a 50-mg/dL increase in the LPA wGRS in the UK Biobank from Burgess et al.16 C, Parental life span and age at the end of the health span. Models were adjusted for age, sex, and the 10 first ancestry-based principal components. IVW indicates inverse-variance weighted; Lp(a), lipoprotein(a); NA, not applicable; OR, odds ratio; and Q, quartile. Error bars indicate 95% CIs.
The More You Have, the Worse It Gets
A large meta-analysis pooling data from over 950,000 people found a clear dose-response relationship: the higher your Lp(a), the greater your risk of dying from cardiovascular disease. Each 50 mg/dL increase was associated with a 31% higher risk of cardiovascular death. There didn't appear to be a "safe" threshold — risk increased in a straight line as Lp(a) went up.
Interestingly, the risk from Lp(a) seems to be amplified when other cardiovascular risk factors are present. A recent U.S. study found that elevated Lp(a) was most dangerous in people who already had high blood pressure, diabetes, or other traditional risk factors. In people with low baseline risk, high Lp(a) didn't seem to move the needle as much.
An Evolutionary Puzzle
Here's a fascinating twist: if Lp(a) is so harmful, why do humans have it at all? Scientists believe that Lp(a) may have provided a survival advantage earlier in human history. Its ability to inhibit clot breakdown could have helped our ancestors survive traumatic injuries by promoting wound healing. The catch is that this benefit matters most in younger people — the harmful cardiovascular effects don't really kick in until after age 50, well past the age of reproduction. Evolution doesn't "care" much about what happens to you after you've already passed on your genes.
Even more intriguingly, the apolipoprotein(a) protein evolved independently in two completely unrelated groups of animals — hedgehogs and Old World primates (including humans) — suggesting that it conferred a strong enough survival advantage to evolve twice.
What Can You Do About It?
This is where things get tricky. Because Lp(a) is genetically determined, diet and exercise don't meaningfully lower it. Most standard cholesterol-lowering drugs, including statins, don't reduce Lp(a) either, and some may even raise it slightly.
However, there's reason for optimism. Several drugs specifically designed to lower Lp(a) are currently in late-stage clinical trials. These include medications like pelacarsen and olpasiran, which use cutting-edge RNA-based technology to reduce Lp(a) production in the liver by up to 90%. If these trials show that lowering Lp(a) actually prevents heart attacks and strokes, not just lowers the number on a lab test, it could open up an entirely new frontier in cardiovascular prevention.
What Is Lipoprotein Little a?
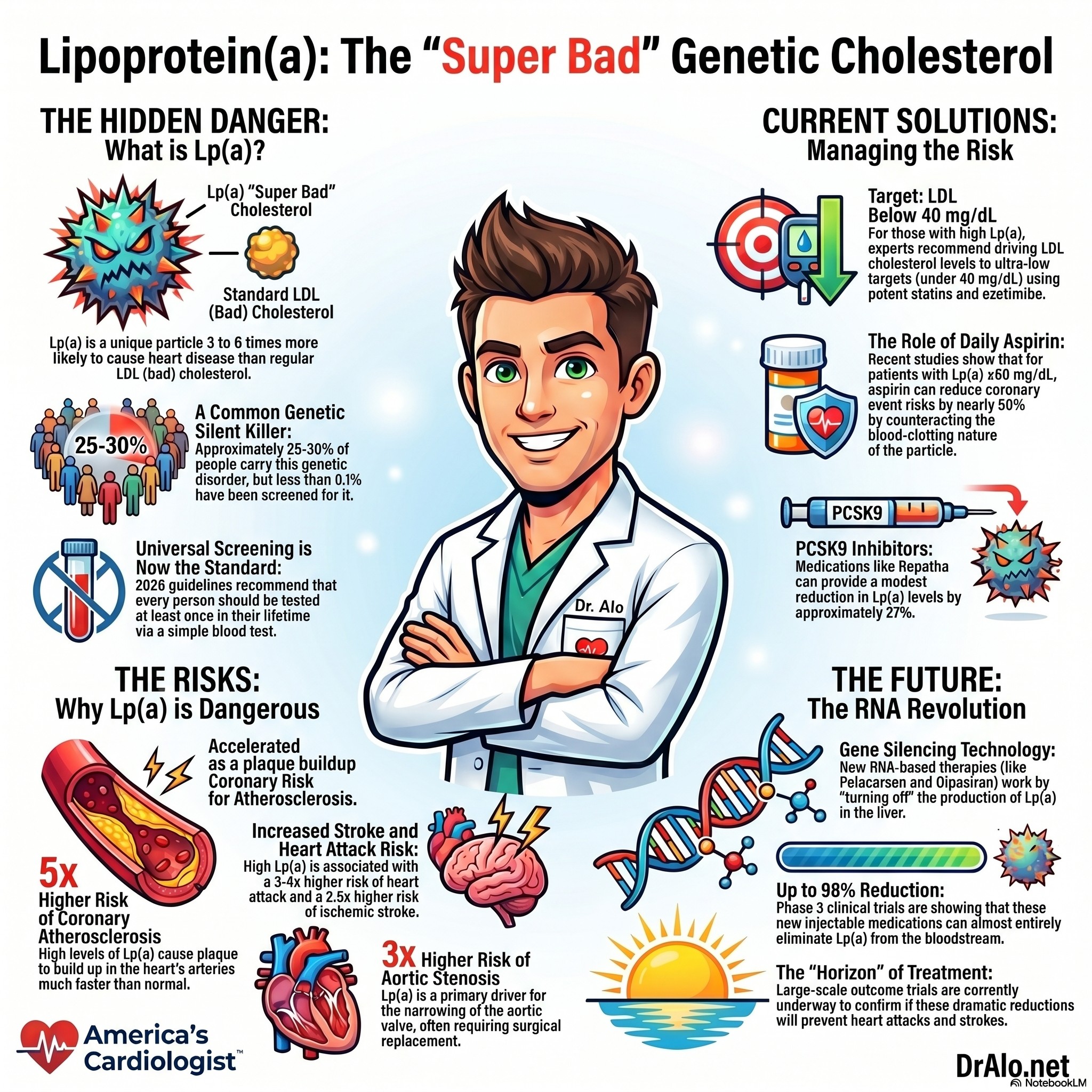
Lipoprotein a is a very atherogenic type of cholesterol. Everyone knows that LDL is "bad cholesterol", well lipoprotein a is "super bad cholesterol". It is three to six times more atherogenic than the regular bad cholesterol.
It is genetic and about 25-30% of people have this genetic disorder and less than 0.1% ever get screened. It's a simple blood test and everyone should be tested at least once in their lifetime.
The current US and European guidelines recommend that everyone should be screened for this. I have been recommending this for years! The guidelines have finally caught up in 2026.
Lipoprotein a Summary Infographic:
Lipoprotein a Video
Here's a video for those who are more visually inclined:
Structure of Lipoprotein Little a (LPa)

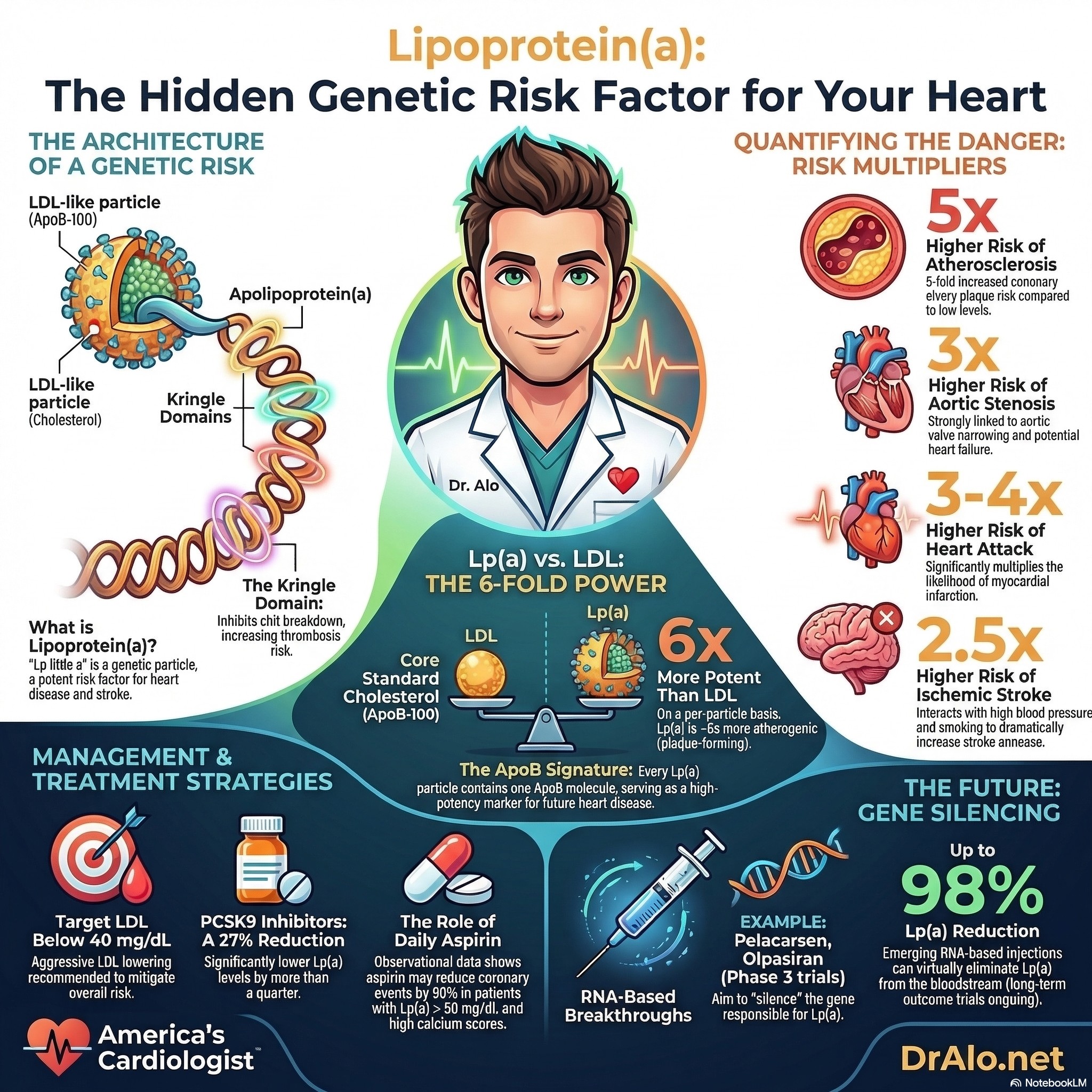
Lipoprotein(a) is composed of two primary components, the apoB-100 protein, and a glycoprotein called apolipoprotein(a). The apoB-100 protein is found in low-density lipoprotein (LDL), which is often referred to as "bad" cholesterol. The apoB-100 protein is found on all LDL particles and all other atherogenic particles, and hence it's a good marker for disease and atherogenicity. The higher the ApoB, the more atherosclerosis you are going to have.
Apolipoprotein(a) is similar in structure to plasminogen, a protein involved in blood clotting. Lp(a) is unique in that it contains a kringle domain, which is a type of protein domain found in many blood-clotting factors. See the diagram above.
The size of Lp(a) can vary, and there are several isoforms, which differ in the number of kringle domains present. The number of kringle domains appears to be an important determinant of Lp(a) function and may influence its potential to cause disease and atherogenicity.
Lipoprotein a Lp(a) Summary Infographic
Function of Lipoprotein(a)
The function of Lp(a) is not entirely clear, but it is thought to play a role in the regulation of blood clotting. Lp(a) has been shown to inhibit the breakdown of blood clots by binding to plasminogen, which prevents it from converting to plasmin, an enzyme that dissolves blood clots. This mechanism may be important in preventing excessive bleeding but may also contribute to the formation of blood clots and blockages in the arteries.

Above is a lipoprotein little a particle with the Kringle chain on the outside.
Medical Significance of Lipoprotein(a)
High levels of Lp(a) in the blood have been associated with an increased risk of cardiovascular disease, stroke, aortic valve disease, and other related conditions. Lp(a) appears to contribute to the development of atherosclerosis, a condition in which plaque builds up in the arteries, causing them to narrow and harden. This can lead to reduced blood flow to the heart, brain, and other organs, increasing the risk of heart attacks, strokes, aortic stenosis, peripheral artery disease, and other serious complications.
Look at the table below. Your chance of having a heart attack is 3-4 times higher. The chance of having aortic stenosis (tight aortic valve) is 3 times higher. The risk of coronary artery atherosclerosis is 5 times higher. The risk of atherosclerosis in any other arterial bed (carotid, iliac, femoral, strokes) are also 1-2 times higher. The risk of heart failure is 1.5 to 2 times higher.
Because LP(a) significantly increases the risk of these diseases, we must take this very seriously.

Studies on Lipoprotein a
Several studies have shown that individuals with high levels of Lp(a) are at an increased risk of developing cardiovascular disease, even when other risk factors are taken into account. For example, a study published in the New England Journal of Medicine found that individuals with Lp(a) levels in the top 20% of the population had a 70% increased risk of developing coronary heart disease compared to those in the bottom 20%. (https://www.nejm.org/doi/full/10.1056/NEJMoa0902604)
Lipoprotein a And Stroke Risk
Lp(a) has also been associated with an increased risk of stroke, particularly in individuals with a history of high blood pressure or smoking. A study published in the Journal of the American Medical Association found that individuals with high levels of Lp(a) were at a 2.5-fold increased risk of developing ischemic stroke compared to those with low levels. (https://jamanetwork.com/journals/jama/article-abstract/184315)
More Recent JAMA Evidence Shows Stronger Associations
More recent studies have found stronger associations than the original 2009 meta-analysis. A 2024 JAMA Cardiology study examining pooled data from multiple U.S. cohorts found that among individuals without baseline atherosclerotic disease, those in the highest Lp(a) percentile (91st-100th) had a 75% increased hazard of ischemic stroke (HR 1.75, P = 0.016) compared to the reference group.
Similarly, a 2025 study in The Lancet Neurology examining 30-year stroke risk in healthy women found that women in the highest lipoprotein(a) quintile had a 27% increased risk of ischemic stroke (HR 1.27, 95% CI 1.05-1.55) compared to the lowest quintile. When participants who initiated statin therapy were censored, this association strengthened to a 55% increased risk (HR 1.55, 95% CI 1.18-2.03).
Source:
https://jamanetwork.com/journals/jama/article-abstract/184315
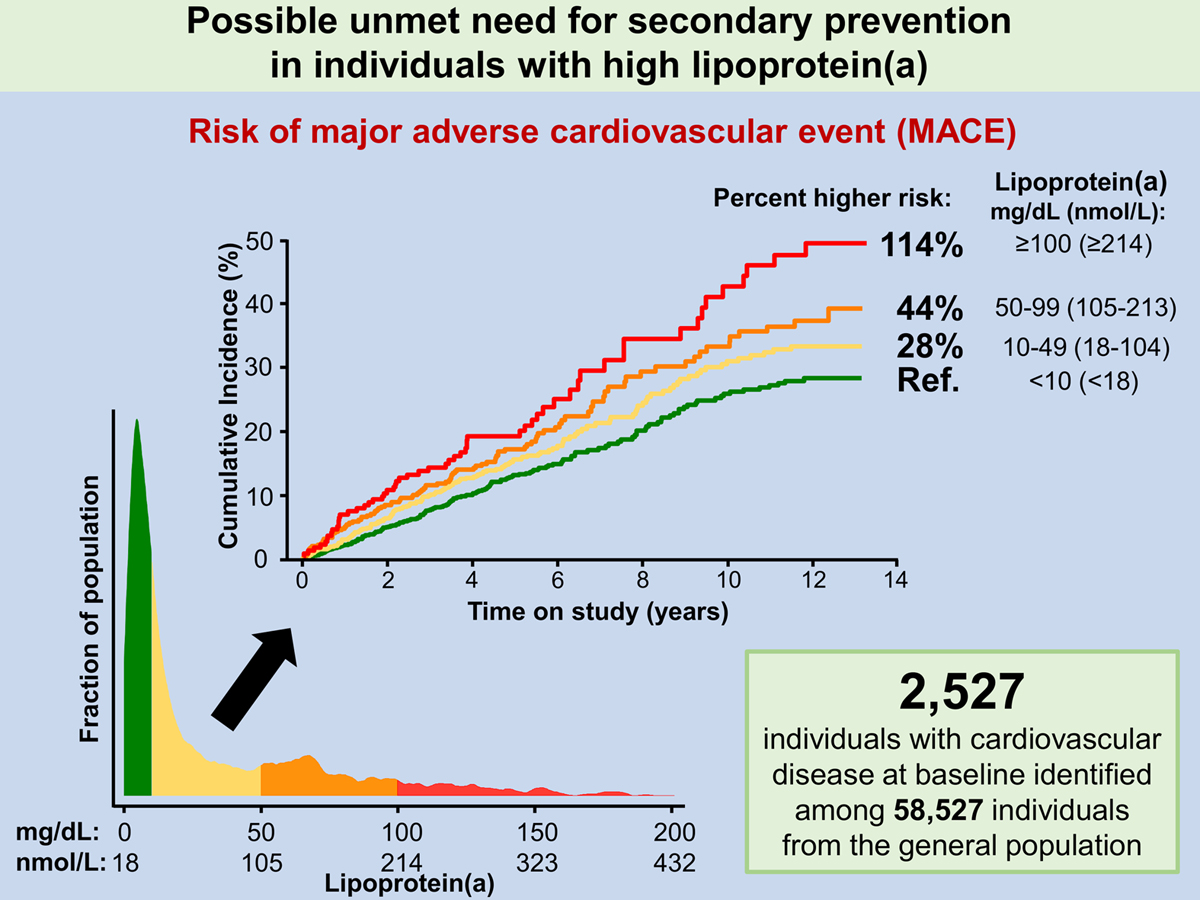
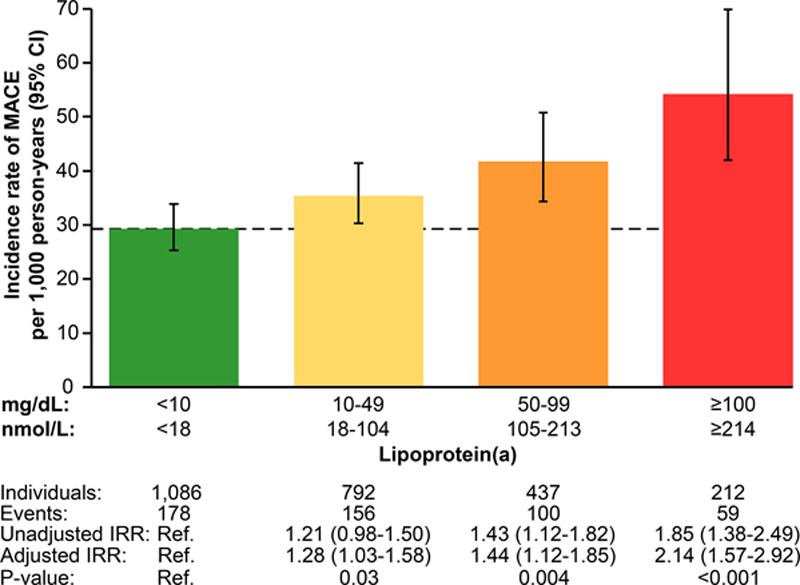
Risk Of MACE with Lp(a) Elevation
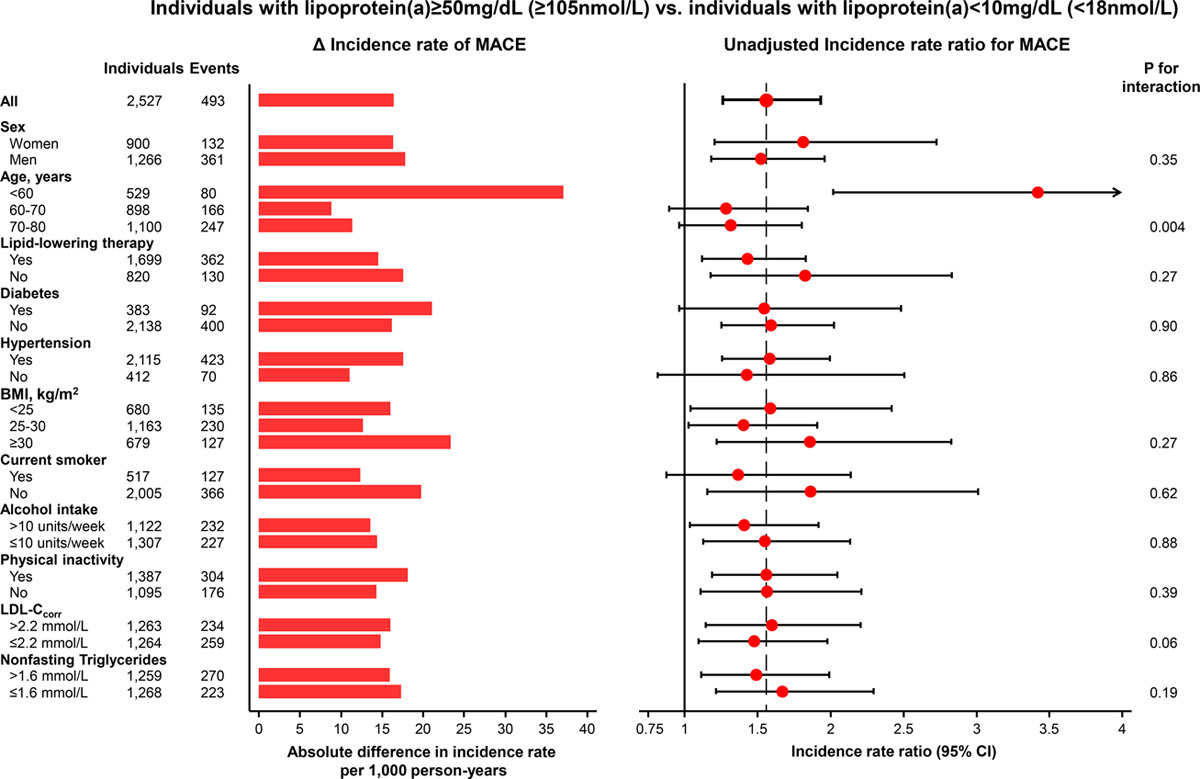
Another article published in JAMA sowed that high concentrations of Lp(a) are associated with high risk of recurrent CVD in individuals from the general population. This study suggests that Lp(a)-lowering by 50 mg/dL (105 nmol/L) short-term (ie, 5 years) may reduce CVD by 20% in a secondary prevention setting.
To achieve 20% and 40% MACE risk reduction in secondary prevention, we estimated that plasma Lp(a) should be lowered by 50 mg/dL (95% CI, 27–138; 105 nmol/L [55–297]) and 99 mg/dL (95% CI, 54–273; 212 nmol/L [114–592]) for 5 years.
Is Lipoprotein(a) 3-6 Times More Atherogenic Than LDL Cholesterol?
Yes, lipoprotein(a) is approximately 6-fold more atherogenic than LDL on a per-particle basis, based on recent apolipoprotein B-based genetic analyses. This substantially greater atherogenicity has critical implications for cardiovascular risk assessment and the potential impact of Lp(a)-lowering therapies currently in development.
The Evidence for 6-Fold Greater Atherogenicity
A landmark 2024 genetic analysis published in the Journal of the American College of Cardiology leveraged the fact that both Lp(a) and LDL contain exactly one apolipoprotein B (apoB) molecule per particle to directly compare their relative atherogenicity. Using genome-wide association studies in the UK Biobank population, investigators identified two distinct clusters of genetic variants: 107 variants linked to Lp(a) mass concentration and 143 variants linked to LDL concentration.
The Mendelian randomization analysis revealed that for a 50 nmol/L higher Lp(a)-apoB, the odds ratio for coronary heart disease was 1.28 (95% CI: 1.24-1.33) compared with only 1.04 (95% CI: 1.03-1.05) for the same increment in LDL-apoB. From these data, the investigators estimated that the atherogenicity of Lp(a) is approximately 6.6-fold (95% CI: 5.1-8.8) greater than that of LDL on a per-particle basis.
This finding has been corroborated by multiple independent sources. A 2025 review in Circulation states that "on an equimolar basis, Lp(a) is ~5 to 6 times more atherogenic than particles that have been widely associated with adverse cardiovascular outcomes, such as LDL". Similarly, a 2025 review in Current Opinion in Lipidology notes that "genetic evidence reveals that Lp(a) is six-fold more atherogenic per particle than LDL".
Source:
https://pubmed.ncbi.nlm.nih.gov/38233012/
https://pubmed.ncbi.nlm.nih.gov/39928714/
https://pubmed.ncbi.nlm.nih.gov/40748007/
Management and Treatment of Lipoprotein(a)
Currently, there are no specific treatments for high Lp(a) levels. There are no medications that reduce Lp(a) directly. Lifestyle modifications, such as a healthy diet have no effect on Lp(a) levels, but can help reduce other risk factors for cardiovascular disease.
With that said, individuals with high Lp(a) are at the highest risk, and hence, I recommend lowering LDL cholesterol to below 40 mg/dL. This is in line with the current European Atherosclerotic Society Guidelines and the American Heart Association and American College of Cardiology guidelines on treating those in the highest risk categories. I also recommend daily aspirin, see below.
Niacin Effects on Lipoprotein a
While niacin may lower Lp(a) levels slightly, it causes more harm than good and is not recommended. Unfortunately, niacin has only shown a very modest decrease and is very difficult to take due to severe side effects, liver toxicity, and it has been shown to make your HDL more atherogenic. Niacin has not reduced cardiovascular outcomes (heart attacks, strokes, death rates) in multiple major trials. (https://pubmed.ncbi.nlm.nih.gov/34134520/ , https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6481429/ , https://pubmed.ncbi.nlm.nih.gov/22085343/, https://pubmed.ncbi.nlm.nih.gov/25014686/, https://www.sciencedirect.com/science/article/pii/S0735109722055942)
Statins Effect on Lipoprotein a
Statins, such as Crestor (rosuvastatin), have been shown to modestly reduce Lp(a) levels, but in other studies, have shown to mildly increase Lp(a) by 10%, but still reduced CVD by 28%. In a study published in the Journal of Clinical Lipidology, treatment with rosuvastatin was associated with a 20% reduction in Lp(a) levels over 12 weeks in individuals with high Lp(a) levels. However, the magnitude of the reduction varied widely among individuals. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8436116/ , https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3946056/
With that said, statins can help reduce LDL cholesterol levels to below 40mg/dL. Especially, potent statins like rosuvastatin. Usually, you will have to use the 20mg or 40mg dose combined with Zetia to get below 40mg/dL.
Ezetimibe Effect on Lipoprotein a
Ezetimibe (Zetia) is another medication that has been shown to modestly lower Lp(a) levels. In a study published in the Journal of Lipid Research, treatment with ezetimibe was associated with a 9% reduction in Lp(a) levels over 12 weeks in individuals with high Lp(a) levels (2). https://jamanetwork.com/journals/jama/fullarticle/184063
PCSK9 Repatha Effect on Lipoprotein a
PCSK9 inhibitors, such as Repatha (evolocumab), are a newer class of medications that have been shown to significantly lower Lp(a) levels. In a study published in the New England Journal of Medicine, treatment with evolocumab was associated with a 27% reduction in Lp(a) levels over 12 weeks in individuals with high Lp(a) levels (3). https://www.nejm.org/doi/full/10.1056/nejmoa1615664
New Medications To Treat Lipoprotein a
There are newer medications that are in phase 3 trials that show a lot of promise in lowering LP(a). Full discussion on these below. But one such medication is hepatocyte-directed antisense oligonucleotide AKCEA-APO(a)-LRx, referred to here as APO(a)-LRx that showed up to an 80% reduction in LP(a). (https://www.nejm.org/doi/full/10.1056/NEJMoa1905239)
It is important to note that while these medications may help to lower Lp(a) levels, their overall impact on cardiovascular risk reduction is still being studied. Individuals with high Lp(a) levels should work with their healthcare providers to determine the best treatment options for managing their overall cardiovascular risk.
Aspirin To Reduce Risk of Lipoprotein a
Several recent studies from 2024-2026 demonstrate that aspirin may reduce cardiovascular events in individuals with elevated lipoprotein(a) ≥50 mg/dL in the primary prevention setting, though the evidence remains observational and requires confirmation in randomized trials.
The most recent findings include a February 2026 study in the European Heart Journal showing that regular aspirin use was associated with dramatically lower risks of aortic valve calcium and severe aortic stenosis in people with high Lp(a). Among those with Lp(a) ≥75 mg/dL, aspirin was associated with a 58% lower risk of aortic valve calcium (HR 0.42) and among those with Lp(a) ≥50 mg/dL, an 87% lower risk of severe aortic stenosis (HR 0.13). Notably, this benefit was specific to elevated Lp(a) and not seen with elevated LDL cholesterol.

A September 2025 study in JACC Advances extended these findings to patients with chronic kidney disease, demonstrating that aspirin use was associated with a 38% reduction in myocardial infarction (HR 0.62) and a 28% reduction in end-stage renal disease (HR 0.72) among those with Lp(a) ≥50 mg/dL, without increased bleeding risk. Importantly, no benefit was observed in those with lower Lp(a) levels.
Earlier observational studies from the Multi-Ethnic Study of Atherosclerosis (MESA) published in 2024 showed aspirin was associated with a 46% reduction in coronary heart disease events (HR 0.54) among individuals with Lp(a) >50 mg/dL without baseline cardiovascular disease. A 2025 review in Current Atherosclerosis Reports noted that recent studies have consistently observed approximately 50% risk reduction for coronary heart disease events with aspirin use among individuals with Lp(a) >50 mg/dL.
However, a large multi-cohort study published in August 2025 analyzing data from ARIC, CHS, and MESA found no evidence that aspirin's association with cardiovascular disease differed by Lp(a) levels, highlighting the conflicting nature of current evidence.
The mechanistic rationale centers on Lp(a)'s prothrombotic and antifibrinolytic properties, which may make it particularly responsive to antiplatelet therapy. Earlier randomized trial data from the ASPREE trial (2022) showed that among older adults with genetic variants associated with elevated Lp(a), aspirin reduced major adverse cardiovascular events by 11.4 events per 1,000 person-years in high-risk carriers without significantly increased bleeding.
Current guidelines acknowledge this emerging area. The 2024 AHA/ASA Stroke Prevention Guidelines specifically identify patients with elevated Lp(a) as a potential subgroup that could benefit from aspirin in primary prevention, though they note additional studies are needed. All current evidence comes from observational studies or post-hoc analyses, and randomized controlled trials are needed to definitively establish whether aspirin should be recommended for primary prevention in individuals with elevated Lp(a).
New Lipoprotein a Medications Are Coming Soon
The most promising therapeutic developments are RNA-based agents that achieve 80-98% sustained Lp(a) reductions through gene silencing of the LPA gene. These include antisense oligonucleotides (pelacarsen) and small interfering RNAs (olpasiran, lepodisiran, zerlasiran, SLN360).
Pelacarsen inhibits mRNA production from the LPA gene in hepatocyte nuclei and is administered by once-monthly subcutaneous injection, achieving approximately 80% Lp(a) reduction. Olpasiran, lepodisiran, and zerlasiran inhibit mRNA production within the cytosol of hepatocytes and are injected subcutaneously two to four times yearly, achieving up to 98% reductions. An alternative approach, muvalaplin, inhibits the attachment of apolipoprotein(a) to apolipoprotein B on LDL particles and achieves approximately 65% reduction with daily oral administration.
Large cardiovascular outcomes trials are currently underway to determine whether these dramatic biochemical reductions translate into meaningful clinical benefits. The Lp(a) HORIZON trial (NCT04023552) of pelacarsen has enrolled 8,323 patients with established atherosclerotic cardiovascular disease and Lp(a) ≥70 mg/dL, with a primary composite endpoint of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and urgent coronary revascularization. Olpasiran and lepodisiran are also being studied in phase 3 cardiovascular outcome trials.
Comparing Potential Benefits: What the Evidence Suggests
Direct comparison between aspirin and RNA-based therapies is impossible without head-to-head trials, but Mendelian randomization analyses provide insight into the magnitude of Lp(a) lowering required for clinical benefit. A 2019 analysis estimated that a 65.7 mg/dL reduction in Lp(a) would be needed to match the coronary heart disease risk reduction achieved by lowering LDL-C by 38.67 mg/dL (approximately 22% risk reduction in short-term trials).
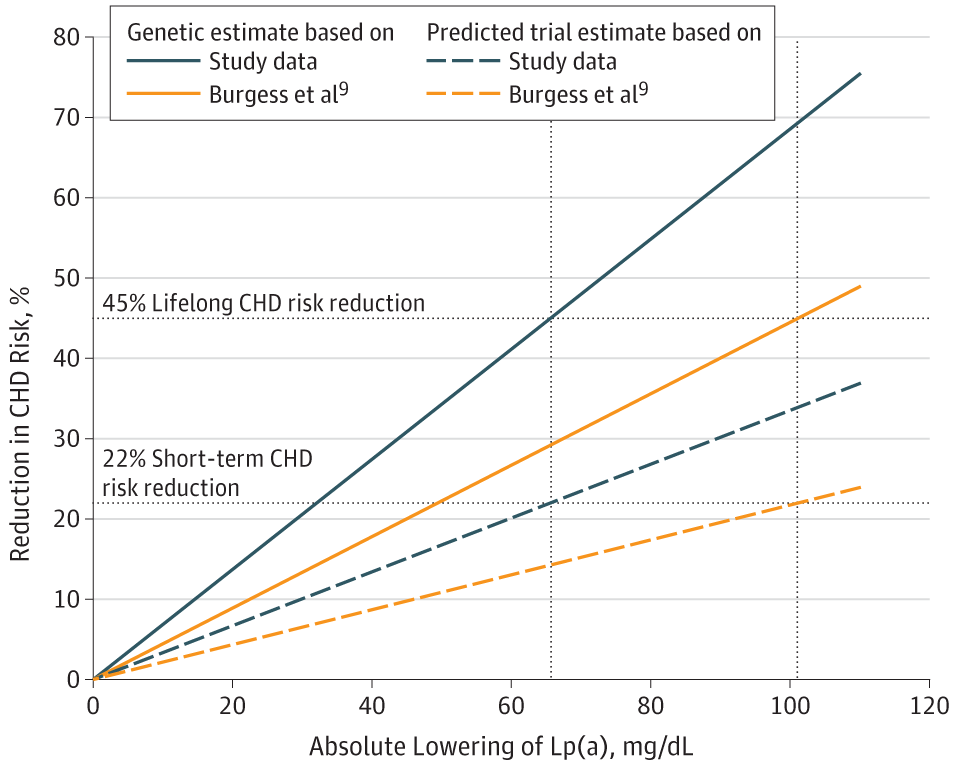
Figure 2. Estimates of Coronary Heart Disease (CHD) Risk Reduction With Lowering of Lipoprotein(a) (Lp[a]) Concentration
Estimation of the Required Lipoprotein(a)-Lowering Therapeutic Effect Size for Reduction in Coronary Heart Disease Outcomes: A Mendelian Randomization Analysis. JAMA Cardiol. May 31, 2019.
This suggests that the 80-98% Lp(a) reductions achieved by RNA-based therapies, which in absolute terms could represent 40-100+ mg/dL reductions in individuals with baseline Lp(a) of 50-100 mg/dL, should theoretically provide substantial cardiovascular benefit if the Mendelian randomization estimates are accurate. By contrast, aspirin does not lower Lp(a) levels (or does so only modestly and inconsistently), so any benefit would derive from antiplatelet effects interacting with Lp(a)'s prothrombotic properties rather than from Lp(a) reduction itself.
The approximately 50% relative risk reduction observed with aspirin in MESA participants with Lp(a) >50 mg/dL is striking but comes from observational data subject to residual confounding.[6] If confirmed in randomized trials, this magnitude of benefit would be clinically meaningful, but the absolute event reduction depends on baseline risk. In ASPREE, aspirin reduced events by 11.4 per 1,000 person-years in rs3798220-C carriers, a substantial absolute benefit in this high-risk genetic subgroup.
What Happens When The New RNA-Based Medications Arrive?
If ongoing trials demonstrate that RNA-based Lp(a)-lowering therapies reduce cardiovascular events, they will likely supersede aspirin as the preferred intervention for high-risk individuals with elevated Lp(a). The magnitude of Lp(a) reduction (80-98%) far exceeds what can be achieved with any currently available therapy, and if Mendelian randomization estimates are accurate, this should translate into substantial cardiovascular benefit.
However, several scenarios could preserve a role for aspirin even after RNA-based therapies become available:
- Cost and access limitations: RNA-based therapies will likely be expensive and may not be accessible to all patients who could benefit
- Combination therapy: Aspirin's antiplatelet effects may provide additive benefit beyond Lp(a) lowering alone
- Intermediate-risk populations: RNA-based therapies may be reserved for highest-risk individuals, leaving aspirin as an option for those with moderately elevated Lp(a)
- Negative trial results: If phase 3 trials fail to demonstrate cardiovascular benefit despite dramatic Lp(a) lowering, aspirin might remain the only intervention with suggestive (albeit incomplete) evidence of benefit
Bottom Line On Aspirin and Emerging RNA Based Therapies
Aspirin may provide meaningful cardiovascular benefit in individuals with elevated Lp(a) >50 mg/dL, with observational data suggesting approximately 50% relative risk reduction in select populations. While this evidence is incomplete and guidelines do not currently recommend aspirin solely for elevated Lp(a), the absence of approved targeted therapies creates a therapeutic void that aspirin—a widely available, low-cost intervention, may partially fill through shared decision-making in high-risk individuals.
Emerging RNA-based therapies promise 80-98% Lp(a) reductions that, if translated into proportional cardiovascular benefit, would far exceed aspirin's potential impact. However, these therapies remain years away from approval, and their ultimate efficacy, safety, cost, and accessibility remain uncertain. Until results from ongoing phase 3 trials become available, aspirin represents a reasonable consideration for primary prevention in carefully selected individuals with elevated Lp(a), particularly those with additional high-risk features such as elevated coronary artery calcium, after thorough discussion of potential benefits and bleeding risks.
The next several years will be transformative for Lp(a) management, with definitive answers expected from both aspirin observational studies and RNA-based therapy outcome trials. In the interim, clinicians must navigate uncertainty, balancing the desire to address a prevalent, genetically determined cardiovascular risk factor against the limitations of current evidence and the promise of more effective therapies on the horizon.
Lipoprotein Little a Conclusion
Lipoprotein(a) is a unique lipoprotein that carries cholesterol and other fats through the bloodstream. It appears to play a role in the regulation of blood clotting, but high levels of Lp(a) in the blood have been associated with an increased risk of cardiovascular disease, stroke, and other related conditions. While there are no specific current treatments for high Lp(a) levels, lifestyle modifications and certain medications may help to lower levels and reduce overall risk for related conditions.
There are a few medications in phase III trial that look very promising causing up to an 80% reduction in Lp(a) levels,
Further research is needed to better understand the role of Lp(a) in disease development and to develop more targeted treatments. In the meantime, individuals with high Lp(a) levels should work with their healthcare providers to manage their overall risk for cardiovascular disease and related conditions.
You can also look up some of these phase III trials and see if you can get into a trial to get your numbers down.
Bottom Line
As of today, we can recommend daily aspirin and reducing LDL cholesterol to below 40 mg/dL, and preferably in the single digits if the patient has had multiple ischemic events. If you have had multiple strokes, stents, heart attacks, aortic valve replacement, you need your LDL cholesterol below 40 mg/dL.
Further Reading on Lipoprotein a:
https://www.acc.org/latest-in-cardiology/articles/2019/07/02/08/05/lipoproteina-in-clinical-practice
https://www.ahajournals.org/doi/10.1161/ATV.0000000000000147
Lipoprotein a References:
- Nordestgaard BG, Langsted A. Lipoprotein(a) and Cardiovascular Disease (Lancet, 2024).
- Reyes-Soffer G, Ginsberg HN, Berglund L, et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association (Arteriosclerosis, Thrombosis, and Vascular Biology, 2021).
- Schwartz GG, Ballantyne CM. Existing and Emerging Strategies to Lower Lipoprotein(A) (Atherosclerosis, 2022).
- Lacaze P, Bakshi A, Riaz M, et al. Aspirin for Primary Prevention of Cardiovascular Events in Relation to Lipoprotein(a) Genotypes (Journal of the American College of Cardiology, 2022).
- Razavi AC, Bhatia HS. Role of Aspirin in Reducing Risk for Atherosclerotic Cardiovascular Disease in Individuals With Elevated Lipoprotein(A) (Current Atherosclerosis Reports, 2025).
- Bhatia HS, Trainor P, Carlisle S, et al. Aspirin and Cardiovascular Risk in Individuals With Elevated Lipoprotein(a): The Multi-Ethnic Study of Atherosclerosis (Journal of the American Heart Association, 2024).
- Bhatia HS. Aspirin and Lipoprotein(a) in Primary Prevention (Current Opinion in Lipidology, 2023).
- Kosmas CE, Bousvarou MD, Papakonstantinou EJ, et al. Novel Pharmacological Therapies for the Management of Hyperlipoproteinemia(A) (International Journal of Molecular Sciences, 2023).
- Nissen SE, Linnebjerg H, Shen X, et al. Lepodisiran, an Extended-Duration Short Interfering RNA Targeting Lipoprotein(a): A Randomized Dose-Ascending Clinical Trial (The Journal of the American Medical Association, 2023).
- Lamina C, Kronenberg F, Lp(a)-GWAS-Consortium. Estimation of the Required Lipoprotein(a)-Lowering Therapeutic Effect Size for Reduction in Coronary Heart Disease Outcomes: A Mendelian Randomization Analysis (JAMA Cardiology, 2019).
-
JACC. Advances. 2025.New
- Aspirin and Cardiovascular Risk in Individuals With Elevated Lipoprotein(a): The Multi-Ethnic Study of Atherosclerosis.
-
Journal of the American Heart Association. 2024.
-
Role of Aspirin in Reducing Risk for Atherosclerotic Cardiovascular Disease in Individuals With Elevated Lipoprotein(A).Current Atherosclerosis Reports. 2025.New
-
Aspirin Use and the Risk for Cardiovascular Disease by Lipoprotein(a) Levels: A Multi-Cohort Study.European Journal of Preventive Cardiology. 2025.New
-
Journal of the American College of Cardiology. 2022.
-
2024 Guideline for the Primary Prevention of Stroke: A Guideline From the American Heart Association/American Stroke Association.Stroke. 2024.GuidelineLancet. 2024.ReviewHigh Lipoprotein(a) and High Risk of Mortality.European Heart Journal. 2019.Circulating Lipoprotein (A) and All-Cause and Cause-Specific Mortality: A Systematic Review and Dose-Response Meta-Analysis.European Journal of Epidemiology. 2023.SR
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















