

Does LDL Cholesterol Causes Heart Disease?
Jan 28, 2026
LDL Cholesterol and Heart Disease: Definitive Proof That LDL Causes Atherosclerosis
How do we know that LDL cholesterol causes heart disease? What's the proof? Has LDL met the criteria for causation in the scientific method?
For decades, both physicians and the public have debated the role of Low-Density Lipoprotein (LDL) cholesterol in cardiovascular disease. Is high cholesterol simply a marker of poor lifestyle choices, or is LDL itself a direct biological cause of blocked arteries and heart attacks?
A landmark consensus statement from the European Atherosclerosis Society (EAS) Consensus Panel provides a clear, definitive answer:
LDL cholesterol is a causal factor in atherosclerotic cardiovascular disease (ASCVD).
After reviewing the full body of scientific evidence, including genetics, population studies, and randomized clinical trials, the panel concluded unequivocally that LDL directly causes atherosclerosis, the underlying disease responsible for heart attacks and strokes.
Below is a clear breakdown of the evidence and what it means for long-term heart health.
LDL Causes Heart Disease Infographic Summary:
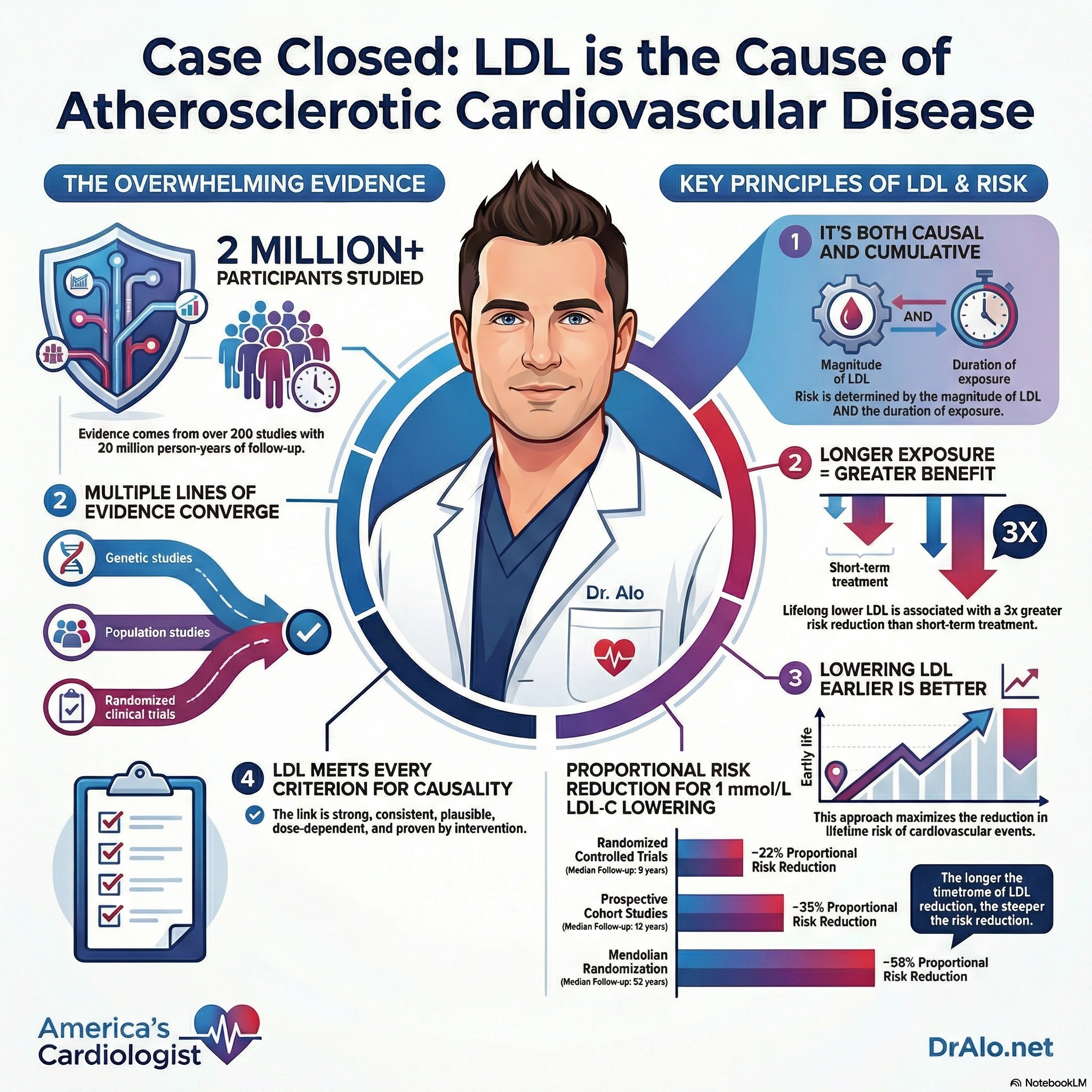
The Scope of the Evidence: One of the Largest Reviews in Cardiovascular Medicine
The EAS Consensus Panel did not rely on a single study. Instead, it analyzed the totality of evidence, including:
- 200+ individual studies
- Over 2 million participants
- More than 20 million person-years of follow-up
- Over 150,000 cardiovascular events
The panel concluded that the relationship between LDL cholesterol and ASCVD satisfies all established criteria for causality, including:
- Biological plausibility
- Strength of association
- Dose–response relationship (biological gradient)
- Consistency across multiple study designs
In other words, this is not correlation, it is causation.
The Four Pillars of Proof That LDL Causes Heart Disease
- Inherited Lipid Disorders (Familial Hypercholesterolemia)
Patients with Familial Hypercholesterolemia (FH), a genetic condition causing extremely high LDL from birth, have a dramatically increased risk of premature coronary artery disease.
Conversely, individuals with rare genetic variants that naturally lower LDL cholesterol experience significantly lower rates of heart disease.
Key insight: LDL exposure from birth directly influences lifetime cardiovascular risk.
- Prospective Epidemiologic Studies
Large population studies consistently show a log-linear relationship between LDL levels and cardiovascular risk.
This means:
- As LDL cholesterol increases,
- The risk of ASCVD rises in a predictable, graded fashion,
- With no clear lower threshold of safety.
Higher LDL = higher risk. Lower LDL = lower risk.
- Mendelian Randomization Studies
Mendelian randomization studies use genetics as a form of natural randomization.
The EAS panel identified variants in more than 50 genes associated with lower LDL cholesterol. Across the board, these variants were linked to lower coronary heart disease risk.
Importantly:
- Genetic variants affecting the same targets as statins, ezetimibe, and PCSK9 inhibitors produced equivalent reductions in cardiovascular risk per unit of LDL lowered.
This confirms that the benefit comes from lowering LDL itself, not from unrelated drug effects.
- Randomized Controlled Trials (RCTs)
Meta-analyses of randomized clinical trials provide the highest level of medical evidence.
Across trials involving:
- Statins
- Ezetimibe
- PCSK9 inhibitors
The findings were remarkably consistent:
A 1 mmol/L (~39 mg/dL) reduction in LDL-C results in ~22% fewer major cardiovascular events over 5 years.
This effect is reproducible, predictable, and proportional to the absolute reduction in LDL.
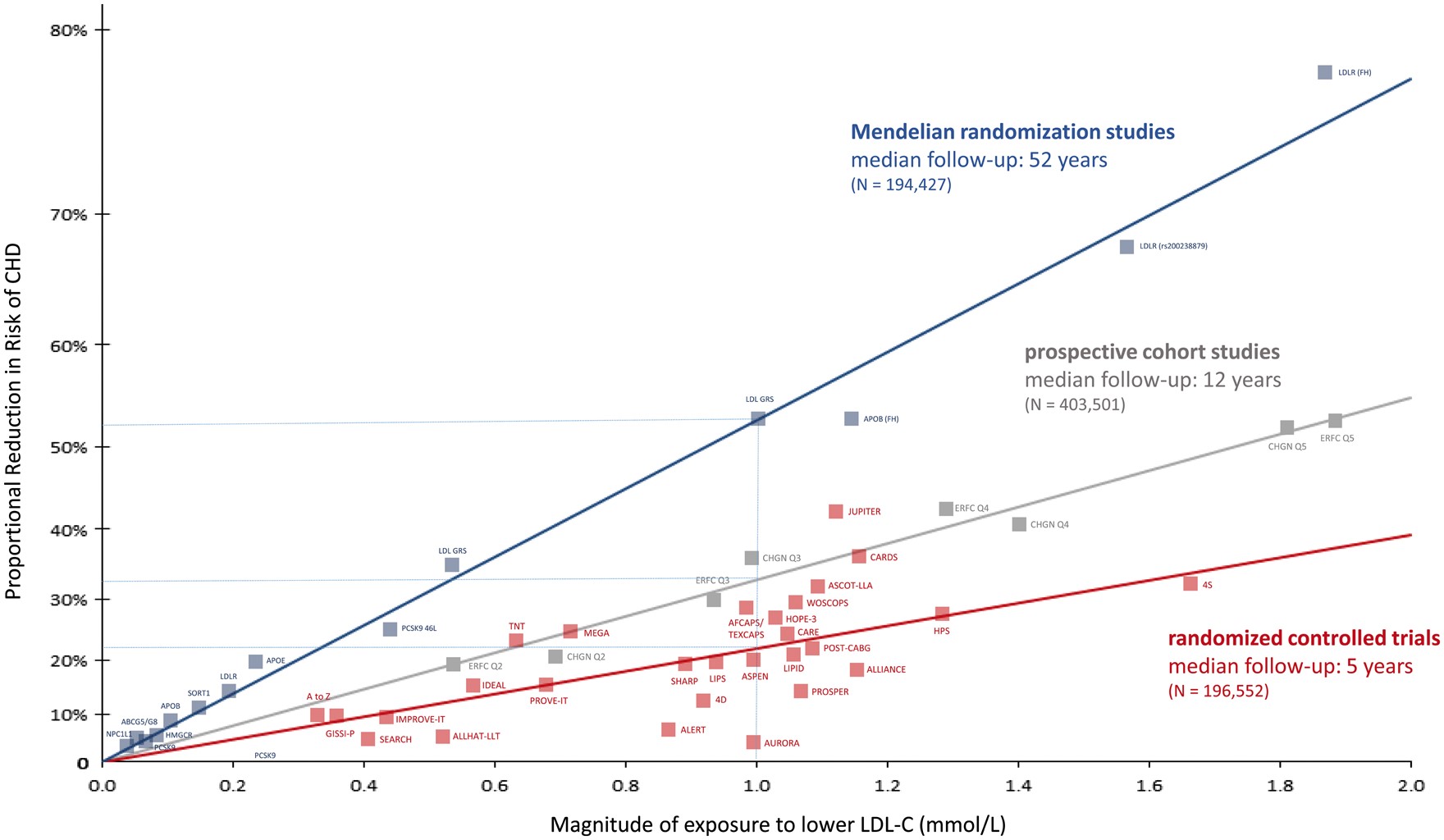
Figure Above: Log-linear association per unit change in low-density lipoprotein cholesterol (LDL-C) and the risk of cardiovascular disease as reported in meta-analyses of Mendelian randomization studies, prospective epidemiologic cohort studies, and randomized trials. The increasingly steeper slope of the log-linear association with increasing length of follow-up time implies that LDL-C has both a causal and a cumulative effect on the risk of cardiovascular disease. The proportional risk reduction (y axis) is calculated as 1−relative risk (as estimated by the odds ratio in Mendelian randomization studies, or the hazard ration in the prospective epidemiologic studies and randomized trials) on the log scale, then exponentiated and converted to a percentage. The included meta-analyses were identified from (i) MEDLINE and EMBASE using the search terms meta-analysis, LDL, and ‘cardiovascular or coronary.
Chart Summary:
As you can tell from the above chart, regardless of how LDL was lowered, incidence of heart disease went down. Even when LDL was lowered with diet interventions, these benefits held true. This further supports the causal role LDL plays in heart disease. No matter how you lower LDL, heart disease improves.
It’s Not About the Drug, It’s About the LDL
One of the most important conclusions from the EAS statement is that how LDL is lowered matters far less than how much it is lowered.
Whether LDL is reduced through:
- Statins
- Ezetimibe
- PCSK9 inhibitors
- Or even ileal bypass surgery
- Dietary interventions (eating less saturated fat)
The cardiovascular benefit is consistent, as long as the therapy increases LDL receptor–mediated clearance of cholesterol from the bloodstream.
LDL cholesterol itself is the causal agent.
The Cumulative LDL Exposure Effect: Why Earlier Is Better
Perhaps the most actionable takeaway is the concept of cumulative LDL exposure over time.
Why Duration Matters
- Long-term exposure to lower LDL (as seen in genetic studies) results in up to 3× greater risk reduction than short-term treatment started later in life.
- While a typical 5-year LDL-lowering intervention reduces risk by ~20–25% per mmol/L,
- 40 years of lower LDL exposure is projected to reduce cardiovascular events by 50–55%.
Atherosclerosis is a time-dependent disease. LDL damage accumulates silently for decades.
Key Takeaways for Patients and Clinicians
The European Atherosclerosis Society Consensus Panel makes one conclusion unmistakably clear:
LDL cholesterol is not just a biomarker, it is a direct cause of atherosclerotic cardiovascular disease.
Practical Implications:
- Start earlier: Lowering LDL earlier in life yields far greater lifetime risk reduction than waiting until disease is established.
- Focus on absolute LDL reduction: Cardiovascular benefit is proportional to both the amount of LDL lowered and the duration of exposure.
- LDL is the target: The mechanism matters less than achieving sustained LDL reduction.
LDL Cholesterol And Heart Disease Bottom Line
If you care about preventing heart attacks and strokes, LDL cholesterol matters—causally, quantitatively, and cumulatively. The science is settled, and the opportunity is prevention.
References:
https://academic.oup.com/eurheartj/article/38/32/2459/3745109?login=false#google_vignette
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















