

Reverse Causality: Why “Low LDL Causes Cancer” Is Misleading
Mar 02, 2026
Does Low LDL Cause Cancer?
You've seen the headlines, "Low LDL Causes Cancer". This is obviously is not true. But how can you explain this? This is due to phenomenon called, "Reverse Causality".
What Is Reverse Causality?
Reverse causality is when scientists think A causes B, but it actually turns out that B causes A, cause and effect are backwards from what they expected.
This is a common problem in medical research, especially in studies that look at people at just one point in time rather than following them over many years. For example, researchers might notice that people with low body weight have higher death rates and think "being thin must be dangerous." But the real explanation could be reverse causality: serious illnesses, like cancer, cause people to lose weight before they die, so the sickness causes the weight loss, not the other way around. Similarly, in heart failure patients, low blood pressure might seem harmful, but it's actually just a sign that the heart is already failing badly.
Reverse Causality Infographic Summary:
Low LDL Increase Mortality?
Patients with end stage cancer, who are dying of cancer, have no appetite, cant' eat much, lose a lot of weight and have a very low BMI and then die. Does that mean the low BMI (low body weight) caused their death? No. They died from cancer. It just so happens, cancer causes low body weight.
The same goes for end stage cancer patients, COPD patients, kidney disease and many other conditions that lead to very low LDL levels... and ultimately, death. The end stage cancer killed them, not the low LDL.
Reverse Causality And Incorrect Conclusions
Reverse causality can lead to wrong conclusions about what actually causes disease. To avoid this problem, researchers try several approaches. They might exclude people who are already sick at the start of the study, or they might ignore data from the first few years of the study to make sure the disease didn't start before the supposed "cause." You can also add a 2 year delay, or "lag" to help eliminate some of the reverse causality effect.
Some scientists use genetic studies to figure out the true direction of cause and effect. However, all these methods have downsides, for instance, excluding sick people or early data can mean throwing away most of the information.
The key difference between reverse causality and other research problems is that the timeline is actually flipped, what looks like the cause is really the effect. Understanding reverse causality helps doctors avoid recommending treatments that target warning signs of disease rather than the actual causes.
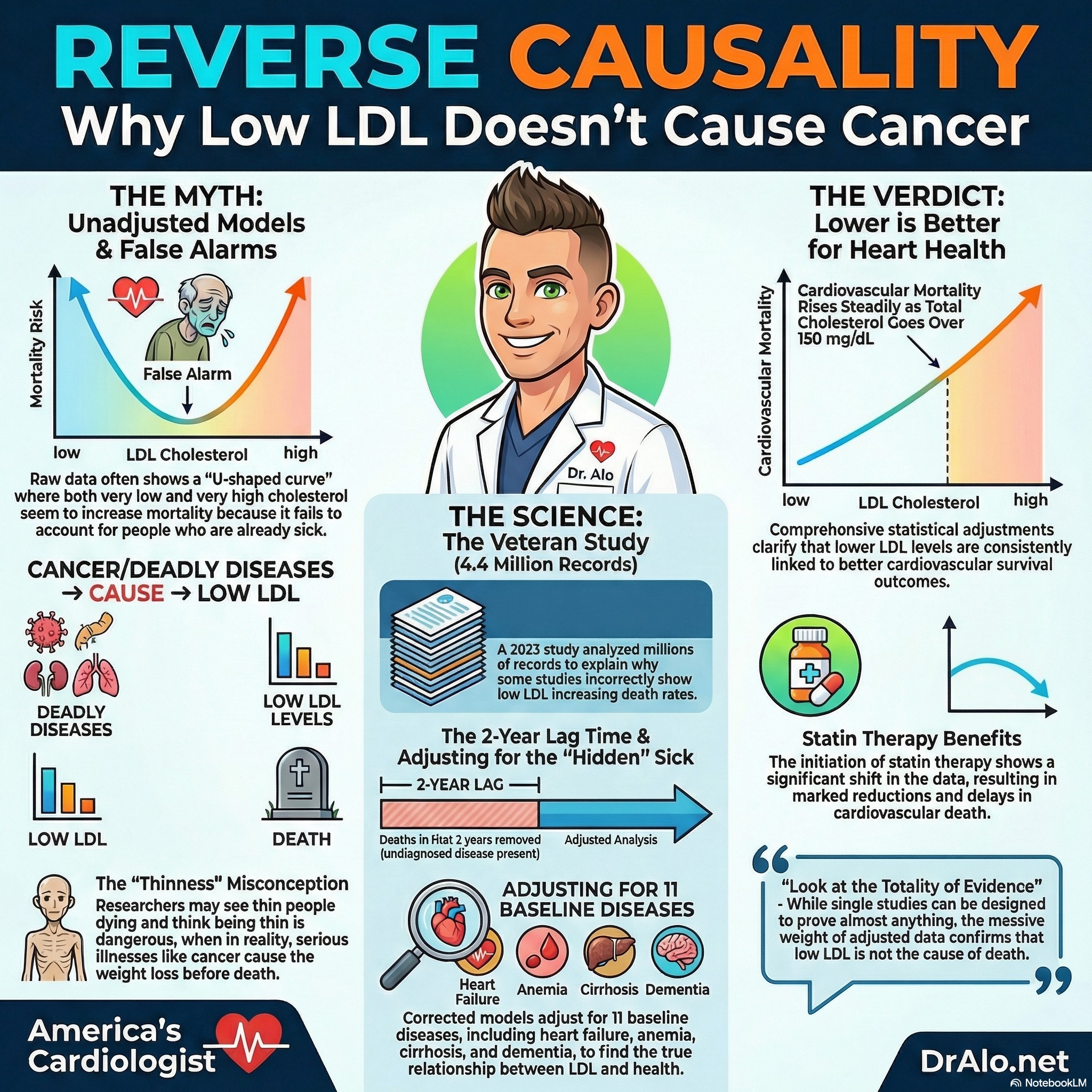
Low Cholesterol And Reverse Causality
A recent article from October 2023 looked at 4.4 million Veterans and the association between high and low cholesterol levels and explained the phenomenon of reverse causation. They did an excellent job of explaining why, in some of these studies, it looks like low LDL-C may increase death rates. The article has brilliant graphics, charts, and a great discussion section explaining why you may see this relationship in these large studies.
One of the most important points they make is that most of these studies, like the Danish study and the Korean study, did not correctly adjust for covariates. Covariates are medical conditions that exist along with elevated cholesterol.
They adjusted for medical conditions that were newly diagnosed within 3 years before the baseline, these included hypertension, diabetes, atrial fibrillation, heart failure, anemia, coronary artery disease, cancer, stroke, dementia, depression, kidney disease, liver disease or cirrhosis, and lung disease. They also looked at income levels and current or past smoking status.
They also looked at initiation of statin use and at what age the statin was initiated and whether or not the patient stopped statin therapy. They adjusted for age, race, sex, BMI, and the usual demographics as well. They also removed death rates that occurred within the first 2 years of follow up to reduce the potential of reverse causality.
In essence, they found ways of correcting for covariates that were not correctly adjusted for in other trials.
The correctly adjusted models look something like the below graphic.
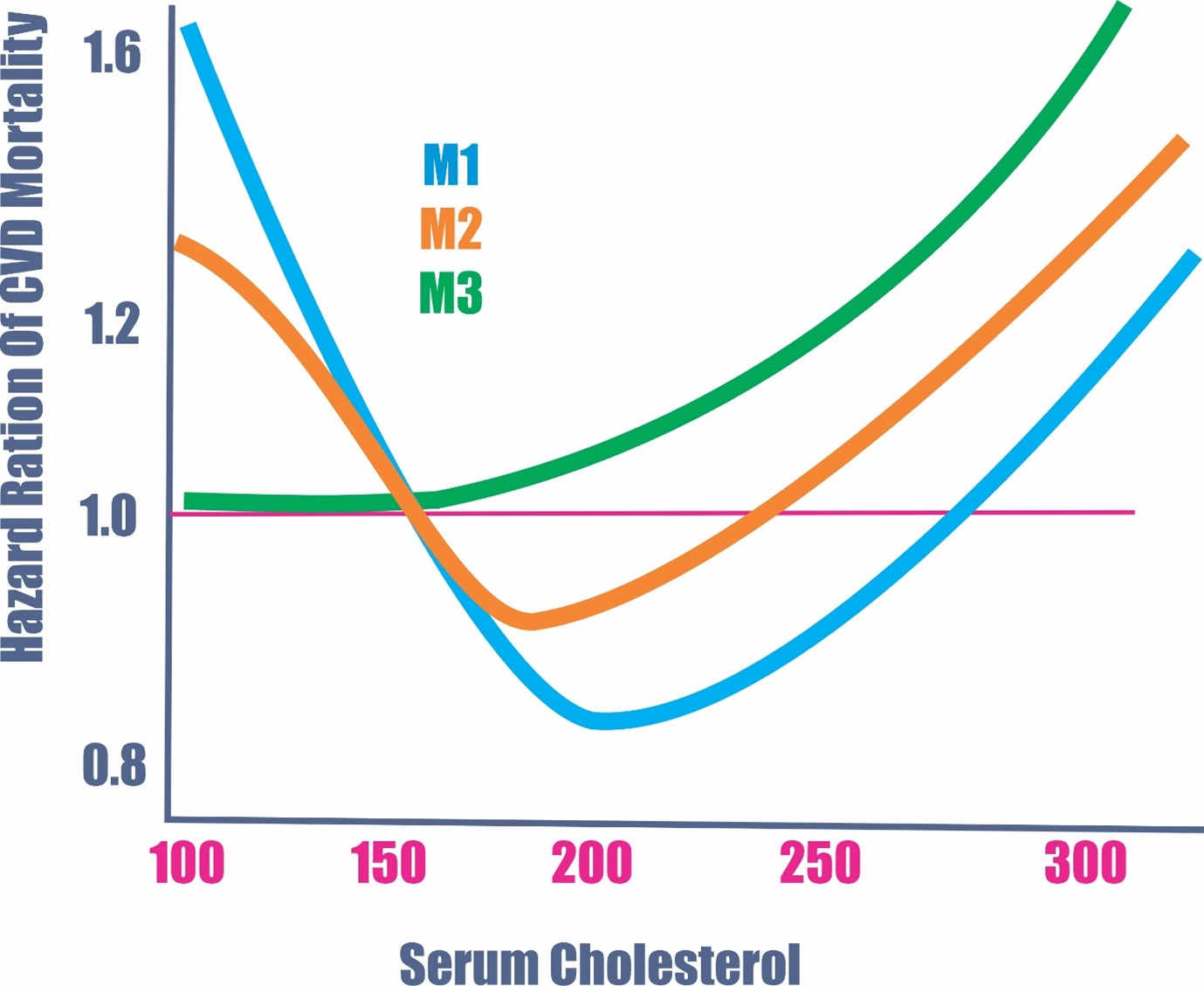
As you can see above, the blue and orange lines are the unadjusted models. You’ll notice that at a total cholesterol around 200 mg/dL, you had the lowest cardiovascular mortality rates. They used this to demonstrate how easy it is to show that low or high cholesterol levels both “increased” death rates with a U-shaped curve.
The blue line (M1) was the first model which only accounted for the covariates of age, race, sex, and smoking status.
The orange model (M2) included everything from M1 and corrected for statin usage, BMI, and hypertension.
However, when you adjust for 11 baseline diseases, as well as M1 and M2, and add a 2-year lag time to reduce the effect of reverse causality, you end up with the green line (M3), which shows, without question, that the higher the total cholesterol, the higher the cardiovascular mortality across all age groups. You’ll also notice that mortality rates start to rise at a total cholesterol of over 150 mg/dL on the adjusted green lines.
This is the correct way to do such an analysis and should eliminate all doubt. There is no way that a properly done study could demonstrate that low LDL-C or total cholesterol would increase cardiovascular mortality.
The study also showed that when statin therapy was initiated, you had a significant rightward shift of the curve with significant reductions and delays in cardiovascular mortality.
Read the article:
https://www.ahajournals.org/doi/10.1161/JAHA.123.030496
We have already gone over the mountains of evidence and data in other parts of this blog on the benefits of lipid lowering therapy.
In science, it’s very important to look at the totality of evidence. You can easily find one study that proves whatever you want. Want to find study that shows that eating green lizards reduces the risk of stroke? There is one. Want a study to show that russet potatoes are harmful to humans? There is one.
In fact, you can design a study or meta-analysis to prove almost anything.
References:
Using Allele Scores to Identify Confounding by Reverse Causation: Studies of Alcohol Consumption as an Exemplar.
International Journal of Epidemiology. 2023. Sallis HM, Palmer T, Tilling K, Davey Smith G, Munafò MR.
Reverse Epidemiology of Conventional Cardiovascular Risk Factors in Patients With Chronic Heart Failure.
Journal of the American College of Cardiology. 2004. Kalantar-Zadeh K, Block G, Horwich T, Fonarow GC.
Association of Breastfeeding and Stunting in Peruvian Toddlers: An Example of Reverse Causality.
International Journal of Epidemiology. 1997. Marquis GS, Habicht JP, Lanata CF, Black RE, Rasmussen KM.
Assessing the Direction of Causality in Cross-Sectional Studies.
American Journal of Epidemiology. 1992. Flanders WD, Lin L, Pirkle JL, Caudill SP.
Reverse Causation and Illness-Related Weight Loss in Observational Studies of Body Weight and Mortality.
American Journal of Epidemiology. 2010. Flegal KM, Graubard BI, Williamson DF, Cooper RS.
Research on Injury Compensation and Health Outcomes: Ignoring the Problem of Reverse Causality Led to a Biased Conclusion.
Journal of Clinical Epidemiology. 2012. Spearing NM, Connelly LB, Nghiem HS, Pobereskin L.
Impact of Follow-Up Time and Analytical Approaches to Account for Reverse Causality on the Association Between Physical Activity and Health Outcomes in UK Biobank.
International Journal of Epidemiology. 2020. Strain T, Wijndaele K, Sharp SJ, et al.
Lifestyle Risk Factors and All-Cause and Cause-Specific Mortality: Assessing the Influence of Reverse Causation in a Prospective Cohort of 457,021 US Adults.
European Journal of Epidemiology. 2021. Rezende LFM, Ferrari G, Lee DH, et al.
Genetics: Implications for Prevention and Management of Coronary Artery Disease.
Journal of the American College of Cardiology. 2016. Assimes TL, Roberts R.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















