

Is Extremely Low LDL Dangerous? Super Low, Super Good?
Jan 25, 2026
Is Extremely Low LDL Cholesterol Dangerous?
Is extremely low LDL cholesterol good for you or dangerous? Luckily we have studies to answer this very question!
Many online influencers want to scare you into thinking that very low levels of LDL cholesterol are dangerous and that you will have a ton of side effects or bad outcomes. This is not true. There is no evidence for this in the literature. The data suggests the opposite.
Very Low Cholesterol Levels
The FOURIER OLE trial showed that with PCSK9 inhibitors we can now get patients to incredibly low levels of LDL cholesterol with no adverse outcomes. Many of the participants achieved LDL-C levels in the 20-25 mg/dL range with further reduction in cardiovascular outcomes and no adverse events.
About 10% of participants in FOURIER had LDL-C levels below 0.5 mmol/L which is 19 mg/dL in the way we report it in the United States.
Infographic summary:
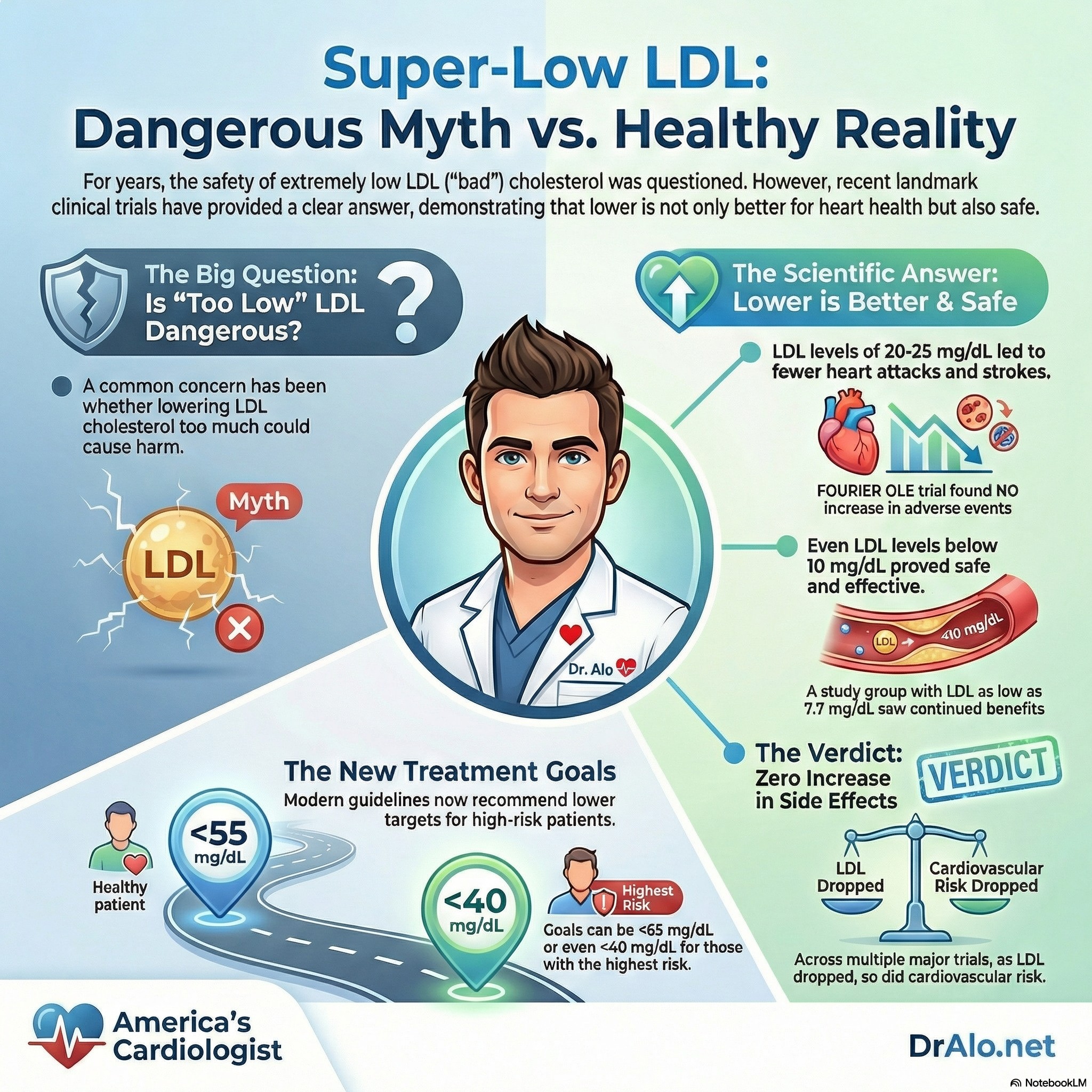
What About LDL Cholesterol Below 10 mg/dL?
A significant subset also achieved LDL-C of 0.2 mmol/L or less, which is 7.7 mg/dL. With no adverse outcomes and a significant reduction in all major cardiovascular event rates.
That does not mean we should try to lower everyone’s LDL-C to 7.7 mg/dL. The studies on PCSK9 inhibitors were quite long at 11.9 years, most outcome trials are not that long. We will need more long-term data before we make changes to recommendations to drive LDL-C to below 10 mg/dL. Based on long term studies and outcomes, we may never decide that 10 mg/dL is a desired outcome. That may change now that we have medications that can accomplish such low levels!
Take a look a the graphic below:
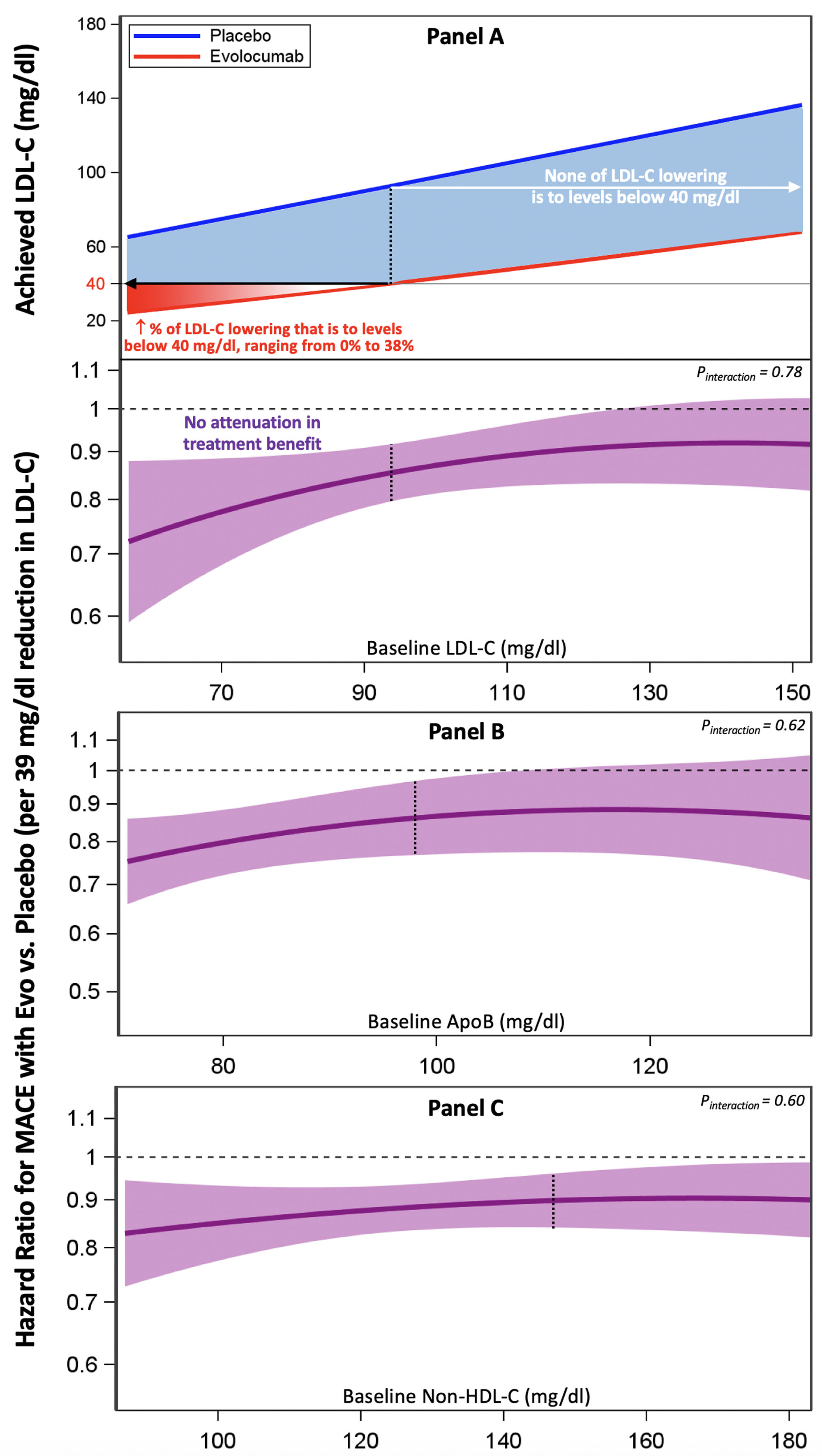
Cardiovascular benefit of continued LDL-C lowering below 40 mg/dl and equivalent thresholds of apoB and non-HDL-C. A, Top, Achieved low-density lipoprotein cholesterol (LDL-C) at 48 weeks as a function of baseline LDL-C.The shaded area represents the amount of LDL-C lowering that occurred between the treatment arms at a given baseline LDL-C, with blue shading representing LDL-C lowering that occurred above 40 mg/dL and red shading representing LDL-C lowering that occurred below 40 mg/dL. The further baseline LDL-C levels were below 93 mg/dL (black dashed line), the greater the proportion of LDL-C lowering that was below 40 mg/dL, ranging from, on average, 0% at 93 mg/dL to 38% at 58 mg/dL. Bottom, Hazard ratio for evolocumab (Evo) versus placebo for cardiovascular death, myocardial infarction (MI), or stroke per 39 mg/dL (1 mmol/L) reduction in LDL-C as a function of baseline LDL-C. As the proportion of LDL-C lowering below 40 mg/dL increased, there was no evidence of attenuation in treatment effect (P value for treatment interaction = 0.78). B, Hazard ratio for evolocumab versus placebo for cardiovascular death, MI, or stroke per 39 mg/dL (1 mmol/L) reduction in LDL-C as a function of baseline apolipoprotein B (apoB). The further baseline apoB levels were below 98 mg/dL (black dashed line), the greater the proportion of apoB lowering that was below 50 mg/dL. As the proportion of apoB lowering below 50 mg/dL increased, there was no evidence of attenuation in treatment effect (P value for treatment interaction = 0.62). C, Hazard ratio for evolocumab versus placebo for cardiovascular death, MI, or stroke per 39 mg/dL (1 mmol/L) reduction in LDL-C as a function of baseline non–high-density lipoprotein (non-HDL-C). The further baseline non-HDL-C levels were below 147 mg/dL (black dashed line), the greater the proportion of non-HDL-C that was below 70 mg/dL. As the proportion of non-HDL-C lowering below 70 mg/dL increased, there was no evidence of attenuation in treatment effect (P value for treatment interaction = 0.60). MACE indicates major adverse cardiovascular event.
Very Low LDL Cholesterol Levels
Very low LDL-C levels would mean low VLDL. However, there would still be enough VLDL particles to perform their role and not increase the risk of fatty liver disease. There should not be an increased risk for soluble vitamin deficiency.
Physiologic levels of LDL-C appear to be 20-40 mg/dL and that is likely to be a future target. Persons with recurrent ischemic events should aim for an LDL-C under 40 mg/dL and perhaps lower.
PCSK9 inhibitors revolutionized cardiovascular care and outcomes. For the first time, we can get everyone to their goal without additional adverse effects. Previously the guidelines recommended reducing LDL-C to below 70 mg/dL. But it was very hard to achieve that goal. We only had statins and not everyone could tolerate them, and they couldn’t get everyone down. Even if they tolerated the highest dose statins, we still couldn’t really get LDL-C to below 70 mg/dL.
With PCSK9 inhibitors, we can now significantly lower LDL-C and get everyone to as low as we want. The only exception may be people with severely elevated lipids due to familial hypercholesterolemia.
We can now significantly reduce LDL cholesterol to levels that we could not even imagine previously!
Therapeutic Options For Very Low LDL Matter
What’s the point of setting the speed limit to 250 miles per hour when no car can go 250 mph? The same applies to cholesterol levels. We can't recommend an LDL cholesterol below 40 mg/dL if we don't have medications that can get us that low.
With the addition of PCSK9 inhibitors to statin therapy and Zetia, we can now reduce total cholesterol and LDL-C by 60-90% in most cases. This caused a significant shift in the European and American guidelines.
We now recommend LDL-C below 55 mg/dL in those with the highest degree of ASCVD risk and those who have already had an event. We can also recommend a goal of less than 40 mg/dL now.
European Guidelines For Very Low LDL Cholesterol
The European Society of Cardiology and the European Atherosclerosis Society Dyslipidemia Guidelines suggest that lowering LDL-C well below 40 mg/dL in a wide range of patients with ASCVD would further lower cardiovascular risk.
There is a really nice graphic from the European Guidelines included in the supplemental guide.
You’ll notice that at a level below 40 mg/dL you have a significant reduction in ASCVD and cardiovascular risk.
Read the article in Circulation discussing the European Society of Cardiology Guidelines:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.056536
Read the FOURIER-OLE trial:
https://www.ahajournals.org/doi/abs/10.1161/CIRCULATIONAHA.122.063399
Safety of extremely low cholesterol:
https://pubmed.ncbi.nlm.nih.gov/28859947/
What About LDL Below 50 mg/dL?
Post hoc analysis from 10 ODYSSEY trial showed that LDL-C below 50 mg/dL showed further MACE reductions. Approximately 33% of participants reached those levels and no increase in adverse events nor risks.
Study:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.116.024604
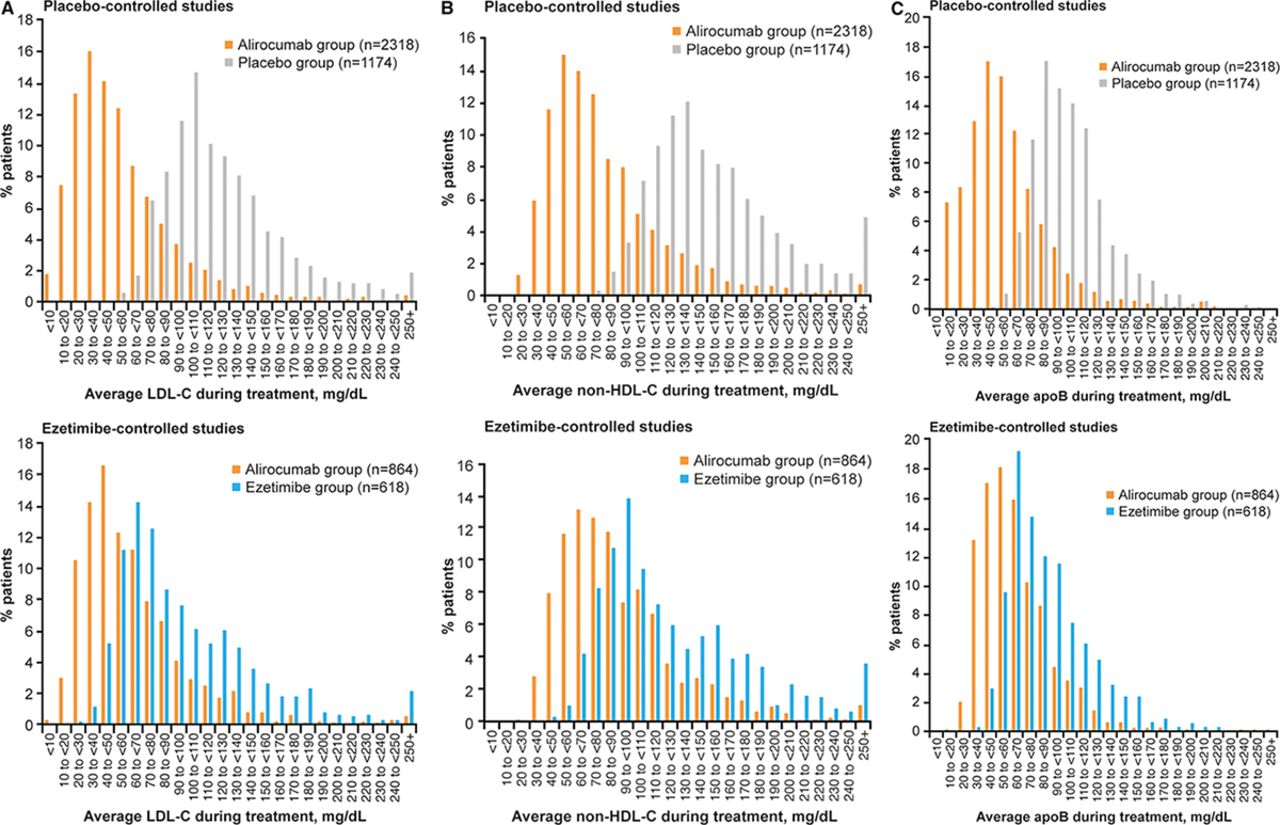
Distribution of achieved levels of low-density lipoprotein cholesterol (LDL-C; A), non–high-density lipoprotein cholesterol (non–HDL-C; B), and apolipoprotein B100 (apoB; C) during treatment stratified by control group. For patients with no postbaseline lipid measurement, baseline values were used. CI indicates confidence interval; and MACE, major adverse cardiovascular event.
In the above linked trial, the bottom lowest percentile had LDL-C concentrations of 0.2 mmol/L which translates into 7.7 mg/dL. That’s incredibly low and they had no adverse effects from being that low. They also had further reduction in cardiovascular events and mortality over 2.2 years of follow up. Please keep in mind that this was a very short trial in patients experiencing acute coronary syndrome. We will need longer term data.
The above is a slide from one of my lectures that I give at medical conferences. The outer ring is the LDL-C goal for most people. You want to be under 100 mg/dL and preferably under 70 mg/dL if you have some risk factors. The inner rings are for people with worse and worsening risk factors. That second ring has a target LDL-C of under 55 mg/dL. The final inner ring is for people that have ASCVD, the worst risk factors, and continue to have repeat ischemic events (heart attacks, strokes, stents, bypass, etc) and we want their LDL-C below 40 mg/dL.
Safety Concerns With very Low LDL
None of the trials showed an increase in adverse events. In fact, the lower the LDL, the lower the risk.
Send this to people who doubt that very low LDL cholesterol is beneficial.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















