Swedish AMORIS Cohort Study Debunked By Cardiologist
Feb 09, 2026
Swedish AMORIS Cholesterol Study: The Retraction Story No One Wants to Talk About
In 2023, a study out of Sweden sent the low-carb, keto, and carnivore corners of the internet into a frenzy. The claim? Centenarians, people who lived past 100 years old, had higher cholesterol than people who died younger. To the anti-statin crowd, this was the smoking gun they had been waiting for. Proof that high cholesterol did not kill you. Proof that the pharmaceutical industry had been lying to everyone. Proof that you should throw your statin in the trash.
There was one massive problem.
The authors retracted their own findings.
As a board-certified cardiologist and advanced lipid specialist, I watched this entire episode unfold in real time. I reviewed the data myself and pointed out exactly why the conclusion did not hold up. In this article, I am going to walk you through what the Swedish AMORIS cohort study actually showed, why the headline finding collapsed under scrutiny, and what the real science says about cholesterol and longevity.
What Is the Swedish AMORIS Cohort Study?
The Swedish AMORIS cohort (Apolipoprotein MOrtality Risk) is one of the largest longitudinal biomarker databases in the world. The cohort enrolled 44,636 Swedish participants and followed them for approximately 35 years. Blood samples and biomarkers were collected when participants were between the ages of 64 and 99. Researchers then identified 1,224 individuals who went on to live past 100 years old and compared their baseline biomarker profiles to the non-centenarians.
Of those 1,224 centenarians, 86 percent were women. That demographic skew matters, as we will get to shortly.
The study had three primary objectives: to identify which biomarkers differed between centenarians and non-centenarians, to determine whether those biomarkers predicted exceptional longevity, and to characterize the metabolic and organ-function profile of people who reached age 100.
On its surface, this sounds like an impressive piece of science. And it is a genuinely interesting dataset. The problem was not the data. The problem was what the authors initially concluded from it.
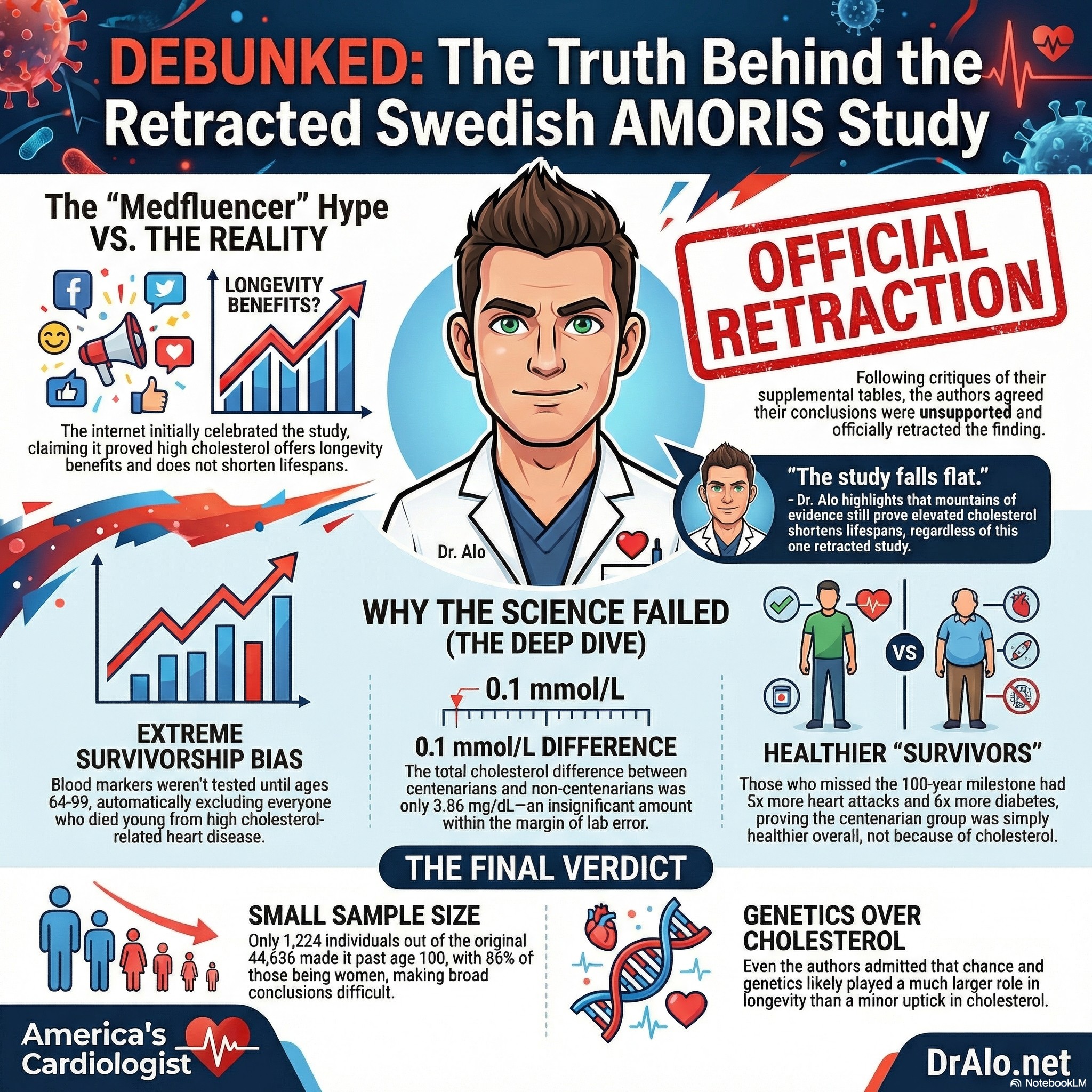
Infographic Summary:
Why Was the Cholesterol and Longevity Finding Retracted?
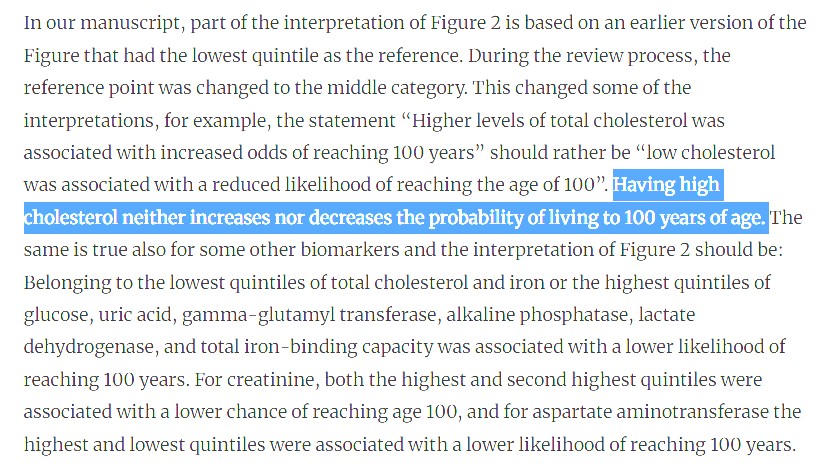
The initial publication suggested that centenarians had higher total cholesterol than non-centenarians. That one sentence was enough to ignite a wildfire of misleading headlines and social media posts claiming that high cholesterol was a longevity marker.
Scientists do what scientists are supposed to do. They reviewed the work. Multiple researchers, myself included, went directly into the supplemental tables provided by the authors and found something glaring: the data did not support the conclusion. The difference in total cholesterol between centenarians and non-centenarians was only 0.1 mmol/L, which converts to 3.86 mg/dL in American units.
Let me put that number in clinical perspective. If you run the same blood sample through the same laboratory machine twice in a row, you can easily see a variation of 3 to 5 mg/dL. That is the inherent measurement error of the test itself. The reported difference between groups was smaller than the margin of error of the instrument used to measure it. No cardiologist or statistician would call that a meaningful finding.
Letters were submitted to the editors. Correspondence went to the authors. To their credit, the authors agreed. They retracted the finding.
The formal retraction notice was published in GeroScience on November 4, 2023 (Vol. 46, No. 2, p. 2793). I have linked to both the original study and the retraction below so you can read them yourself.
Here is their retraction:
Swedish AMORIS Cohort Authors Retracted Findings
Survivorship Bias: The Fatal Flaw in This Line of Reasoning
Even if the authors had never retracted their findings, the study design itself makes the headline conclusion impossible to support. This is textbook survivorship bias, and it is one of the most important concepts in epidemiology for patients to understand.
Here is the core problem. The AMORIS cohort did not collect blood samples at birth or in early adulthood. Biomarkers were collected when participants were between 64 and 99 years old. By the time those blood draws happened, decades of cardiovascular mortality had already occurred. Anyone who had a fatal heart attack at 45, 52, or 58 due to elevated cholesterol was never enrolled in the study. They were already dead. They were never counted. They were never measured.
This matters enormously because of when this cohort was living through its most vulnerable decades. In the 1950s, 1960s, 1970s, and 1980s, the treatment for a heart attack was essentially a hospital bed, morphine, and oxygen. More than 80 percent of heart attack patients did not survive until morning. Interventional cardiology barely existed. Stents were not available. Angioplasty was primitive. And statins, the first truly effective LDL-lowering medications, did not reach patients until 1987.
What this means is that anyone with chronically elevated cholesterol during those decades had no pharmacological protection whatsoever. Their risk was raw and unmitigated. A significant proportion of high-cholesterol individuals were eliminated from the population before the study could ever measure them. The people who survived to age 64 and older with high cholesterol were, by definition, an unusually resilient subset. They may have had protective genetics, lower inflammatory burden, favorable lipoprotein particle characteristics, or other factors that buffered the atherogenic risk of their cholesterol levels.
You cannot look at the survivors of a brutal filter and conclude that the filter was not deadly. That is the logical error at the center of the entire argument.
Survivorship Bias
This study is the ultimate in survivorship bias. They did not collect blood markers until people were between age 64 and 99. This already eliminates a very large portion of society that died young due to elevated cholesterol. Those who survived to 65 had their blood markers tested.
In the 1950s, 60s, 70s, and 80s, most people who were having a heart attack were given a hospital bed, some oxygen and morphine and laid in bed all night. Over 80% would be dead by the morning. It wasn’t until bile acid sequestrants and statins in 1987, that we finally saw a reduction in mortality. Couple that with angioplasty, heart catheterization, and improving stent technology, and that’s when you saw the biggest reductions in mortality.
The Swedish AMORIS cohort study started out with 44,636 individuals, of which, only 1224 made it past 100. Of those 1224, 86% of them were women.
Let’s look at the population make up.
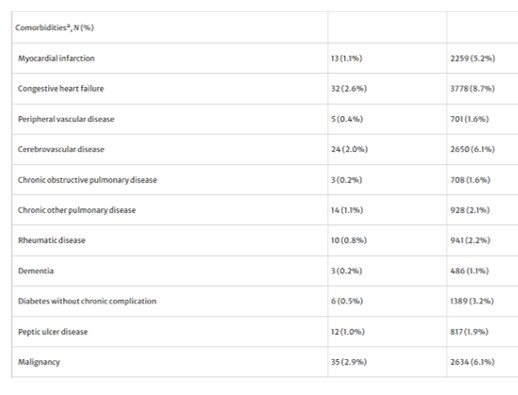
On the far right are non-centenarians. On the left are centenarians. A cursory look will tell you everything you need to know. Those who died before their 100th birthday had 5 times more heart attacks, 4 times more congestive heart failure, 4 times more peripheral artery disease, 8 times more COPD, 6 times more diabetes and the list goes on. This is population bias. The population that did not make it to 100 had more chronic disease. This is also a case of reverse causality.
The ones that made it to 100 years of age, had far less incidence of these horrific diseases.
In the data that was provided in the study and supplemental tables, you will find a different story being told.
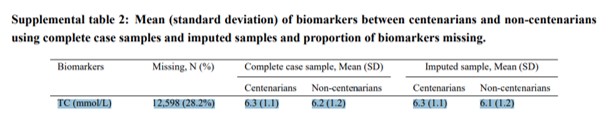
Total Cholesterol (TC) was no different between the centenarians and non-centenarians.
If you look at the supplemental data that was provided, you’ll notice that the difference in total cholesterol between the two groups was only 0.1 mmol/L, which is 3.86 mg/dL in American.
That means one person could have a cholesterol of 197 mg/dL and the other 200 mg/dL. That’s an insignificant difference, especially given the inaccuracy of labs tests and the margin of error. If you run the same blood sample twice through the same machine, you could easily end up with a difference of 3.8 mg/dL and no one would bat an eye.
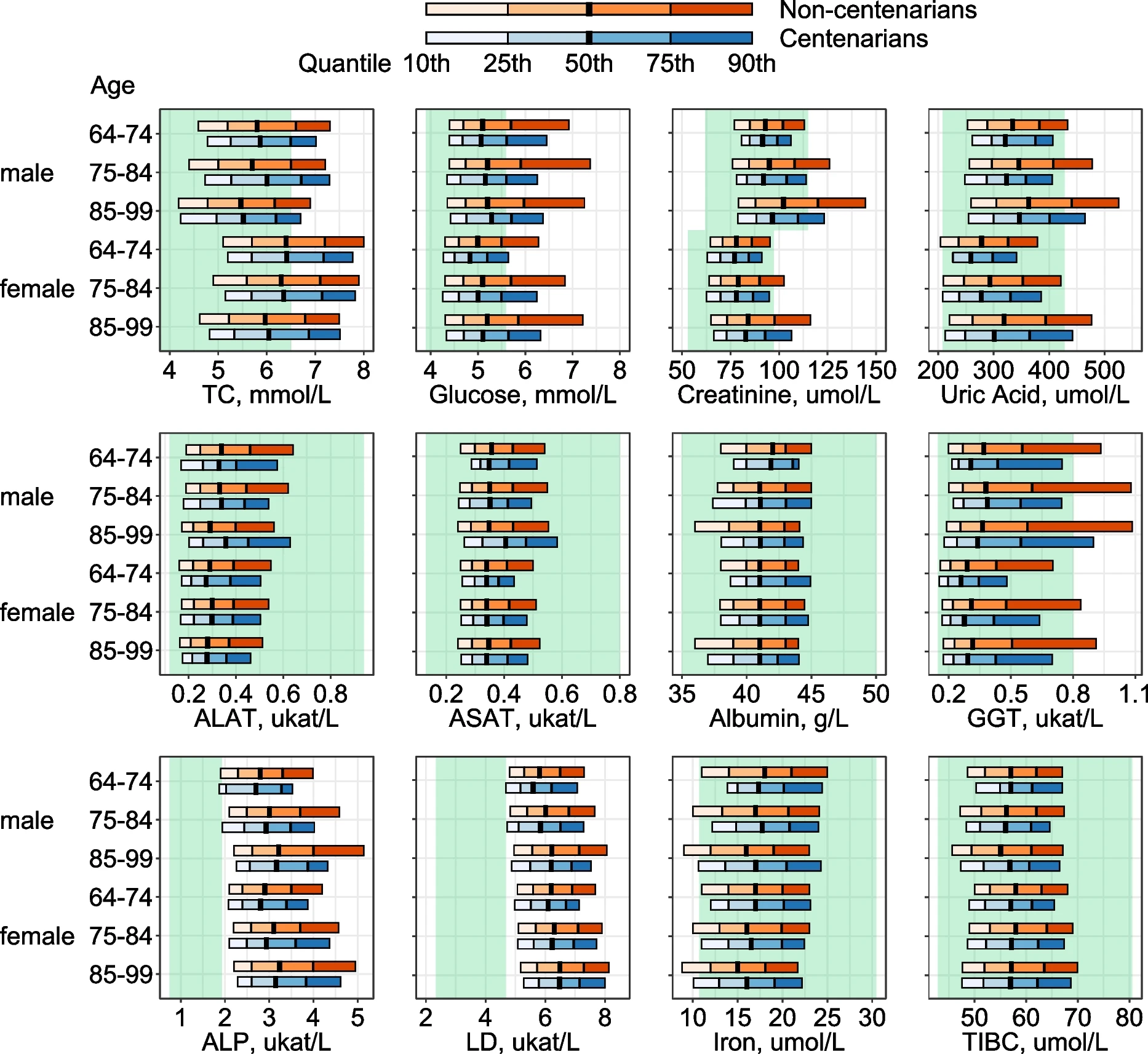
Look at the top left corner. That’s Total Cholesterol (TC). The difference between the centenarians and non-centenarians was minimal. Compare that to uric acid, creatine, or GGT. There are very obvious differences.
If you look at the supplemental data that was provided, you’ll notice that the difference in total cholesterol between the two groups was only 0.1 mmol/L, which is 3.86 mg/dL in American. That means one person could have a cholesterol of 197 mg/dL and the other 200 mg/dL. That’s an insignificant difference, especially given the inaccuracy of labs tests and the margin of error. If you run the same blood sample twice through the same machine, you could easily end up with a difference of 3.8 mg/dL and no one would bat an eye.
The authors themselves, in the conclusion, admitted that chance probably plays a role and that genetics probably plays a role as well. Further, the sample size is quite small at only 1200.
It’s a stretch to conclude from this data that a 0.1 mmol/L increase in total cholesterol explains the entire story of why some people live to 100.
So, while the headlines sounded interesting, the study falls flat. We have mountains of evidence demonstrating that elevated cholesterol shortens your lifespan. But the anti-cholesterol crowd will probably try to run with it.
What Biomarkers Actually Differed Between Centenarians and Non-Centenarians?
Here is what the data actually showed when you look at it honestly.
The centenarians in the AMORIS cohort were dramatically healthier on almost every meaningful clinical marker. Compared to non-centenarians, the people who lived past 100 had five times fewer heart attacks, four times less congestive heart failure, four times less peripheral artery disease, eight times less COPD, and six times less diabetes.
That is not a cholesterol story. That is a chronic disease story. The people who reached 100 simply had far less disease burden across every organ system. They were not protected by high cholesterol. They were protected by the absence of the conditions that kill most people.
When you look at which biomarkers showed genuinely meaningful differences between centenarians and non-centenarians, the story becomes clear. Uric acid levels differed substantially. Creatinine, a marker of kidney function, differed substantially. Gamma-glutamyl transferase (GGT), a liver enzyme, differed substantially. These are markers of metabolic disease, organ stress, and inflammation. The centenarians simply had healthier kidneys, lower metabolic toxicity, and less systemic stress.
Total cholesterol? The difference was 3.86 mg/dL. In a world where lab machines have inherent measurement variation, that number is statistical noise.
Does High Cholesterol Help You Live to 100? What the Data Actually Shows
No. The AMORIS study does not show that. Not before the retraction, and certainly not after.
We have decades of rigorous evidence from randomized controlled trials, Mendelian randomization studies, meta-analyses, and natural experiments involving genetic LDL disorders that consistently point to the same conclusion: elevated LDL cholesterol and elevated ApoB accelerate atherosclerosis, increase cardiovascular event rates, and shorten lifespan.
Individuals with familial hypercholesterolemia, who have been born with genetically elevated LDL, die of cardiovascular disease at dramatically higher rates than the general population when untreated. That natural experiment has been running for generations. The signal is unambiguous.
The centenarians in the AMORIS cohort were not long-lived because of their cholesterol. They were long-lived despite whatever cholesterol levels they carried, because they were a biologically selected group that had already been filtered through 60-plus years of life before anyone drew their blood. Their longevity reflects genetics, low disease burden, favorable organ function, and the absence of the metabolic conditions that kill most people in their 50s, 60s, and 70s.
Claiming that this study proves high cholesterol is beneficial is like studying the health of professional athletes in their 60s who have been training since childhood, finding they have large hearts, and concluding that everyone should develop an enlarged heart. The logic does not hold.
Frequently Asked Questions About the Swedish AMORIS Cholesterol Study
Did the Swedish study prove that high cholesterol leads to a longer life?
No. The finding that centenarians had higher cholesterol was retracted by the authors after independent review showed the difference was only 3.86 mg/dL, which is smaller than standard laboratory measurement variation. The study does not support any conclusion that elevated cholesterol is protective or beneficial for longevity.
What is the AMORIS cohort?
The Swedish AMORIS (Apolipoprotein MOrtality RISk) cohort is a long-running longitudinal study of 44,636 Swedish participants. Biomarkers were collected between ages 64 and 99, and researchers identified 1,224 individuals who lived past age 100. It is a rich dataset for studying aging and biomarker trajectories, but it has significant survivorship bias limitations for interpreting cholesterol's role in longevity.
Why did the authors retract the cholesterol finding?
After the paper was published, independent scientists reviewed the supplemental data tables and found that the total cholesterol difference between centenarians and non-centenarians was only 0.1 mmol/L (3.86 mg/dL), a clinically meaningless difference within normal lab measurement error. The authors acknowledged this, agreed with the critique, and issued a formal retraction in GeroScience (November 4, 2023, Vol. 46, No. 2, p. 2793).
What does survivorship bias mean in longevity research?
Survivorship bias occurs when a study only measures people who have already survived a filtering process, while ignoring those who did not survive it. In this case, anyone who died of a cholesterol-related heart attack before age 64 was never included in the AMORIS cohort. The study therefore only captured people who were resilient enough to survive to the point of enrollment, making it impossible to draw conclusions about whether high cholesterol is generally safe or beneficial.
What biomarkers are actually associated with living to 100?
The AMORIS data showed that centenarians had meaningfully lower levels of uric acid, creatinine, and GGT compared to non-centenarians. These markers reflect kidney health, liver function, and metabolic stress. Centenarians also had dramatically lower rates of heart disease, diabetes, COPD, and peripheral artery disease. Longevity appears to be associated with low organ stress and the absence of chronic disease, not with any particular cholesterol level.
The Bottom Line
The Swedish AMORIS cholesterol study was a genuinely interesting piece of research that was briefly misrepresented, went viral in the wrong direction, and was then corrected by the scientific process working exactly as it should. The authors identified their error and retracted it.
What remains is a dataset that confirms something cardiologists already knew: people who live to 100 tend to be biologically exceptional, with healthier organs, lower metabolic burden, and far less chronic disease than the general population. Their cholesterol levels are not what set them apart.
If you encounter someone on social media telling you that this Swedish study proves high cholesterol is fine and statins are unnecessary, ask them a simple question: did you read the retraction? The answer will tell you everything you need to know about how carefully they are interpreting the science.
Cholesterol management, specifically targeting LDL and ApoB, remains one of the most evidence-backed interventions in all of preventive cardiology. That evidence has not changed. One retracted headline does not undo 60 years of randomized trial data.
References
Original Swedish AMORIS Cohort Study:
https://link.springer.com/article/10.1007/s11357-023-00936-w
Formal Retraction Notice (GeroScience, November 4, 2023):
https://link.springer.com/article/10.1007/s11357-023-00996-y
PMC Full Text of Retraction:
https://pmc.ncbi.nlm.nih.gov/articles/PMC10828262/
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine