

Do Statins Only Reduce Risk by 1%? The Absolute vs. Relative Risk Myth
Dec 30, 2025
Statin Absolute vs Relative Risk
One of the arguments you hear online is that the absolute risk reduction in heart attacks or death is very small. They will say that statins only reduce the risk of death by 1.1%. They argue that this small reduction is not worth the possible side effects of the medication. Even if we were to accept this at face value, there are 9 billion humans on earth. You would save 90 million lives per year. That's a lot of lives saved.
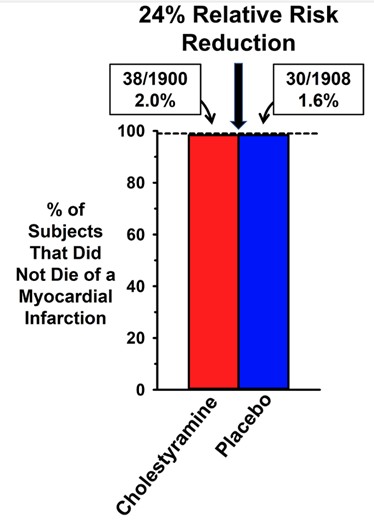
The Medfluencers love this graphic and this chart.
Here you see that placing patients on cholestyramine only reduced the risk of dying of a heart attack by 0.4% in absolute terms. You went from a 2% chance of having a heart attack to a 1.6% chance of having a heart attack, which is a 0.4% absolute reduction. However, this does translate into a 24% relative risk reduction in death from a heart attack.
They use this small absolute risk reduction to deny that there is any benefit or to minimize the 24% relative risk reduction. This is flawed and dishonest thinking. The graphs are not drawn to scale, so you can’t even perceive a real difference.
Even if we stick to their example, if you carried out that intervention (cholestyramine) over billions of people all over the world, you would still save millions of lives. Especially, with medications with little to no side effects.
The biggest problem is they use this example to deny the benefit of other medications like statins, which have shown significantly higher relative and absolute reductions in CV mortality, MACE events, and all-cause mortality. We now know that for every 7 people you place on a statin you save 1 life. But they still insist on using this silly example, with a medication that had very little efficacy to make broad statements.
This gains them a large online following among conspiracy theorists and the anti-science, anti-cholesterol crowd. Which supports them financially by supporting their speaking careers, book sales, supplement sales, etc.
It’s dishonest and harms the public. Unfortunately, they prey on less educated, younger populations and are harming future generations.

Absolute Risk Is Artificially Lower
Another problem with using absolute risk reduction is that it is artificially lower.
Let’s imagine a trial where the intervention is to quit smoking at age 45. You take 10,000 smokers and you tell half of them to quit smoking. You follow them for 5 years, until they are 50 years old.
In that five-year span, about 3% of smokers develop lung cancer and only 2% of non-smokers develop lung cancer. That’s a 1% absolute reduction but a 33% relative risk reduction. But that’s only 5 years. The curve would look something like this:
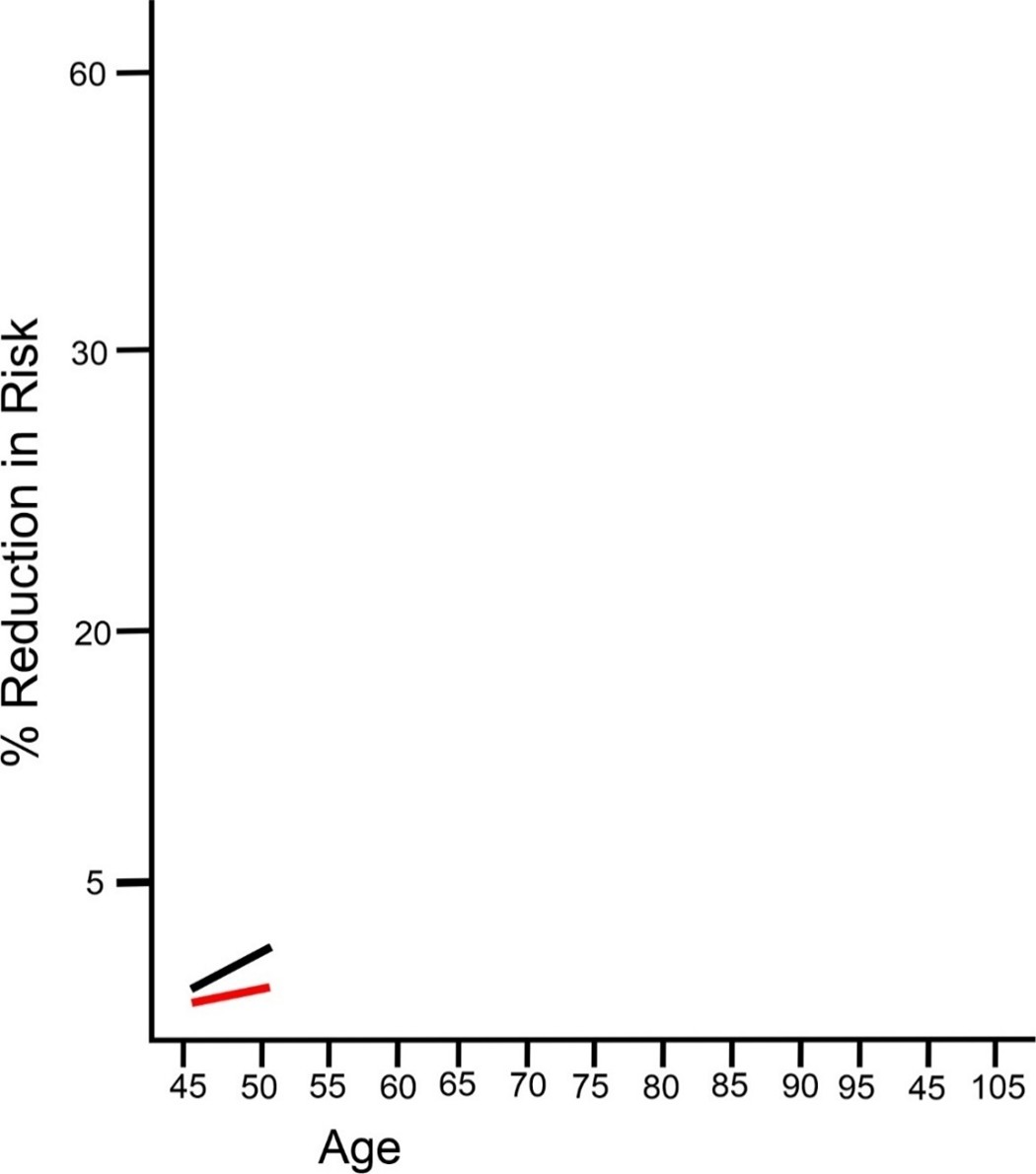
If you quit smoking by age 45, your risk of future lung cancer goes down from 3% to 2%. That’s a 1% absolute risk reduction in those 5 years from age 45 to age 50. But this is a 33% relative risk reduction. As you can see, using the relative risk reduction seems astronomical compared to the absolute risk reduction, which seems miniscule.
Is it plausible then to conclude that people who quit smoking only reduce their risk of lung cancer by 1%?
The problem is that these are short term studies. You cannot look at a five-year study and draw conclusions like that.
Further, it’s unethical to keep people on cigarettes and tell them to keep smoking. Once you see a difference, the trial must be stopped early. You are going to kill a lot of people if you tell them to keep smoking because it’s only a 1% absolute reduction.
If you allow that experiment to continue further, the chart will look very different. We only have this data because people have been smoking for a very long time.
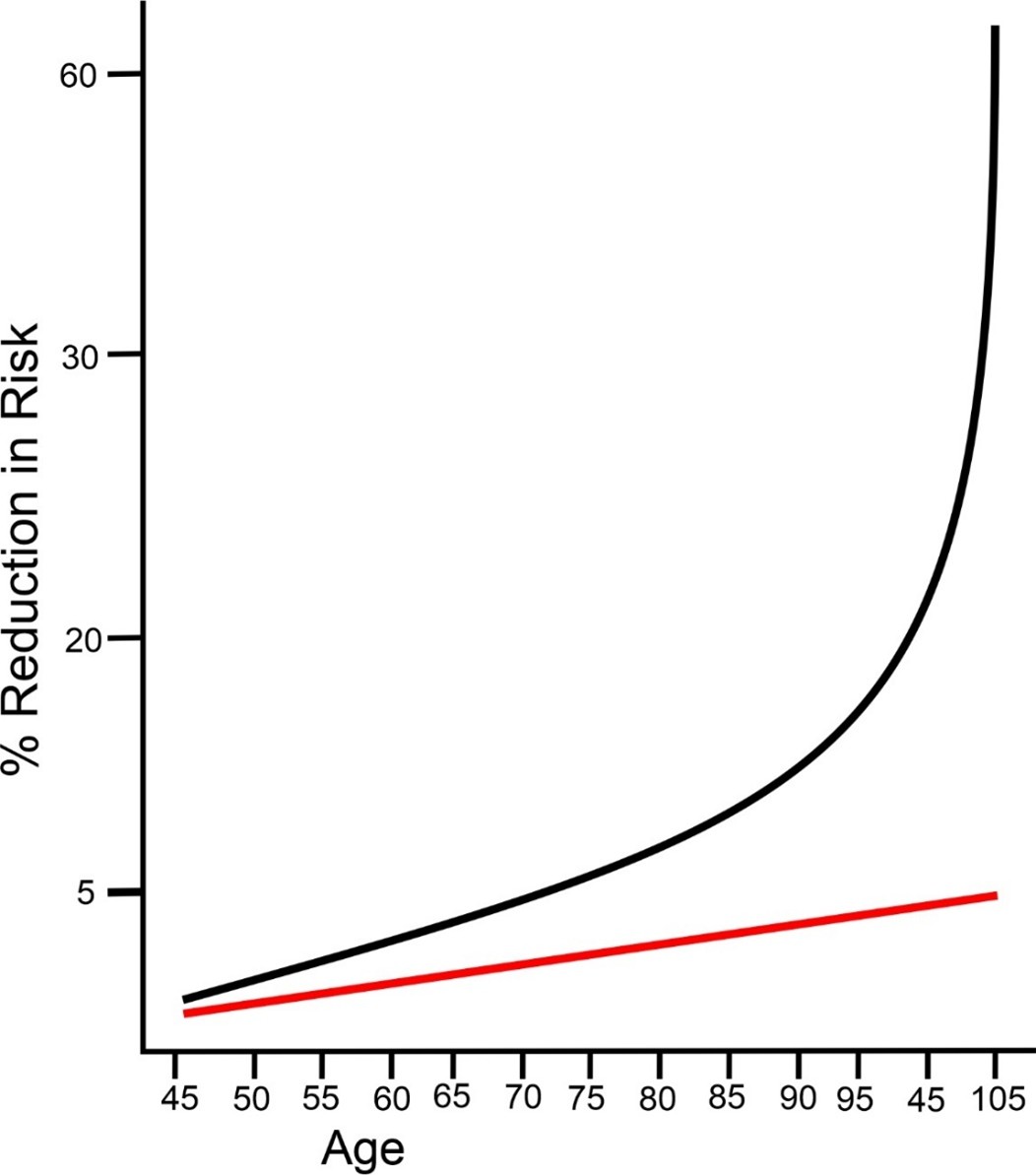
You see that the non-smokers still have a less than 5% chance of getting lung cancer, while those that continued to smoke for longer, had much higher odds of developing lung cancer. Almost to the point of certainty. The area under the curve, or lifetime exposure to cigarette smoke, is what increases your risk. The area under the curve is called “AUC”.
In case you were wondering, that is a real study. Read the smoking cessation study here:
https://academic.oup.com/jnci/article/96/2/99/2520973
Absolute vs Relative Risk In Lipid Lowering
The same applies to cholesterol lowering therapy. When you do a study, like JUPITER for example, that was supposed to evaluate Crestor over 5 years, but you notice a huge drop in death rates after just 13 months. It is no longer ethical to continue the trial.
I highly recommend watching Dr. Gil Carvalho’s video on YouTube explaining the difference between absolute risk reduction versus relative risk reduction. He is an MD and PhD and is a great educator. His channel contains many other evidence based topics around cardiometabolic health.
Video:
https://www.youtube.com/watch?v=vRRD8nXEyGM
A few studies have been published trying to explain this exact principle in various scientific journals. One such study was published in the Journal of the American College of Cardiology.
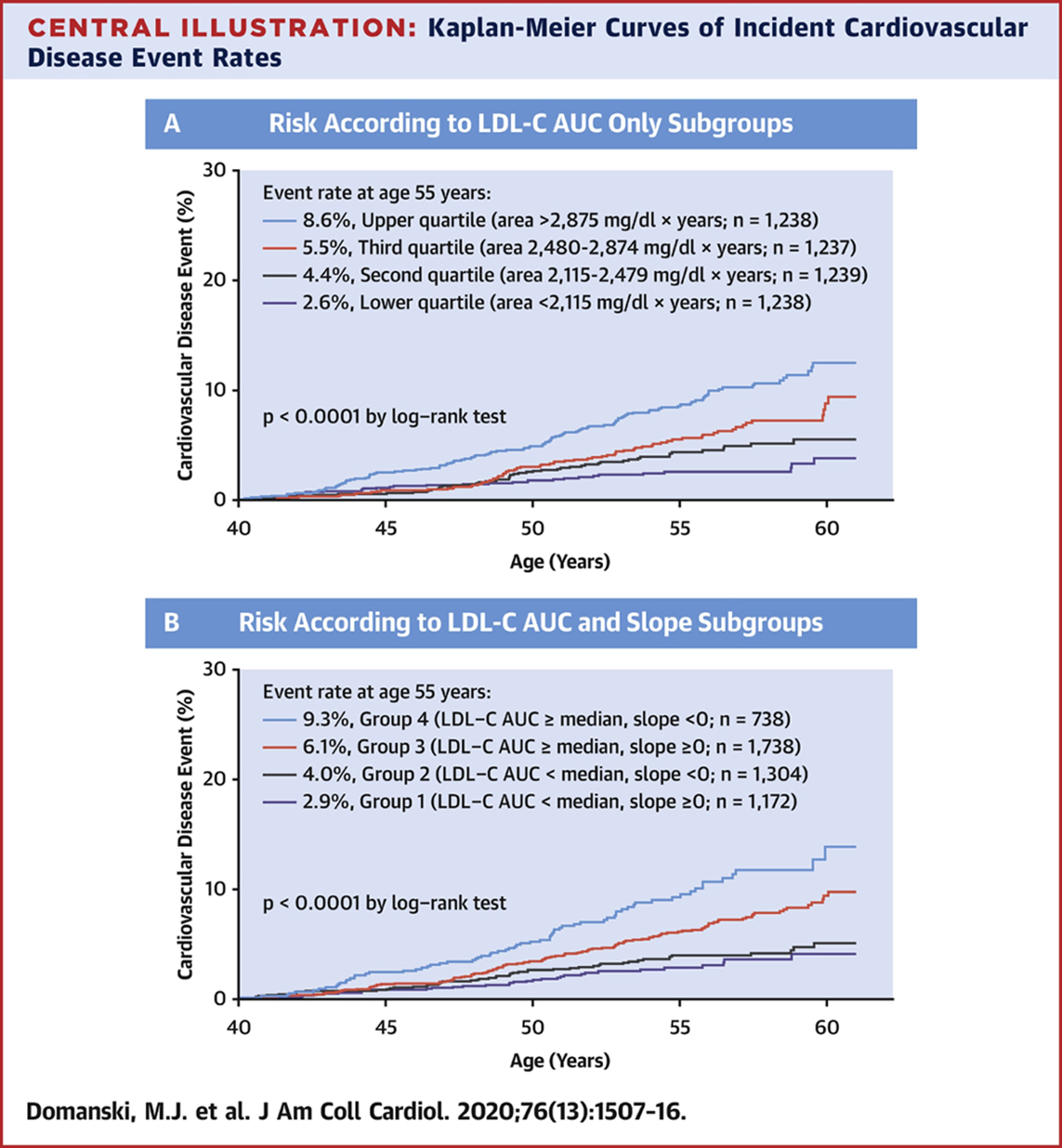
The longer you are exposed to elevated concentrations of apoB, LDL-P, or their surrogates like LDL-C and non-HDL-C, the more likely you are to have a cardiovascular event sooner.
Full Study:
https://www.jacc.org/doi/10.1016/j.jacc.2020.07.059
Absolute Risk Increase As Time On Therapy Increases
Another study published in Circulation in 2022 agrees and concludes that:
“The benefits of LDL-C lowering do not seem to be fixed but increase steadily with longer durations of treatment. The results from short-term randomized trials are compatible with the very strong associations between LDL-C and cardiovascular events seen in Mendelian randomization studies.”
They found that for each 1 mmol/L (38.6 mg/dL) reduction in LDL-C there was a relative risk reduction in major vascular events of 12% for year one, 20% for year three, 23% for year five, and 29% for year seven.
And the effects continue to compound. The area under the curve grows larger and larger.
Full study:
https://www.ahajournals.org/doi/full/10.1161/CIRCOUTCOMES.121.008552
Another very well done article published by Brian Ference demonstrated that the absolute risk reduction is much greater than expected and increases with time. Again, the area under the curve will shrink in your favor, the sooner you lower your LDL-C or apoB.
I am going to leave you with a lot of the graphics from this paper, they are pretty self-explanatory. I will just point out a few nuggets.
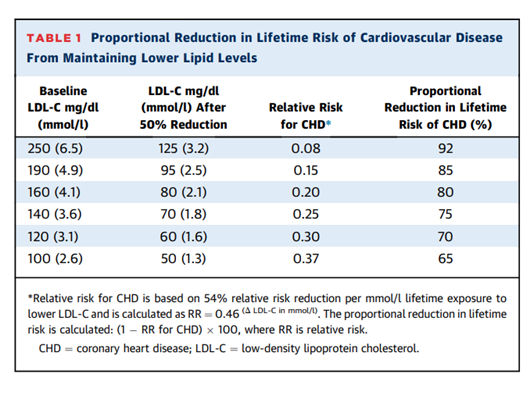
You see from this table that the higher your baseline LDL-C, the more profound reduction in ASCVD with a 50% reduction in LDL-C. Look at the top row that started out with an LDL-C of 250 mg/dL. With a 50% reduction to 125 mg/dL, they reduced their lifetime risk of CVD by 92%. Whereas if you started with an LDL-C of 100 mg/dL, cutting that in half to 50 mg/dL, provided you with a 65% lifetime risk reduction. Those with the highest baseline LDL-C will benefit the most from a 50% reduction over their lifetime.
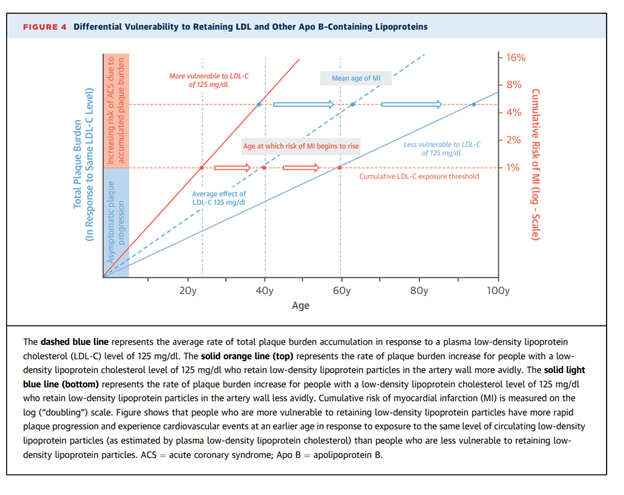
The above chart shows the difference between people who retain LDL particles better than others for the same level of LDL-C. The dashed blue line is the rate of plaque accumulation for a normal person with an LDL-C of 125 mg/dL. The orange line is the people who retain more LDL particles, yet still have an LDL-C of 125 mg/dL. The light blue solid line below is of those that don’t retain LDL particles as well, but still have an LDL-C of 125 mg/dL.
As you can see, the genetics of retaining versus not retaining can make a huge difference in age at first cardiovascular event (heart attack). This will obviously affect your healthspan and lifespan tremendously. Those who consume more saturated fat will retain more LDL particles.
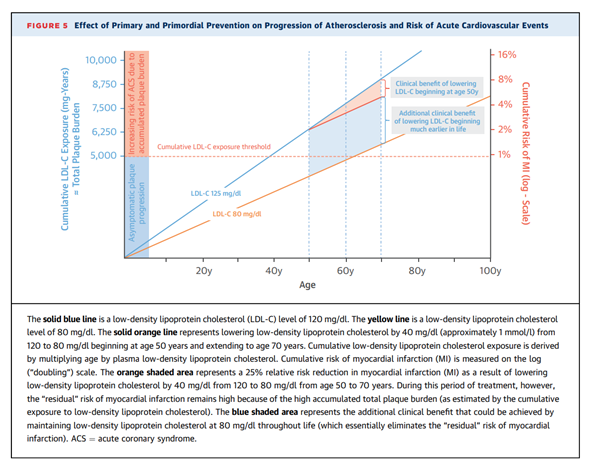
Here you can see two different individuals being exposed to different levels of LDL-C. The blue line is someone who is exposed to an LDL-C of 125 mg/dL for many years. The orange line is someone being exposed to 80 mg/dL for many years. At age 50, they started lipid lowering therapy in the person with the higher LDL-C. They dropped their LDL-C by about 40 mg/dL. This conferred a 25% relative risk reduction. If they had started earlier in life, they would have had much more pronounced risk reduction.
Cumulative LDL Cholesterol Exposure Increase Risk
As you can see the cumulative LDL-C exposure threshold is 5000 mg/years. If your LDL-C is 125 mg/dL and you are 40 years old. Multiply 40 x 125, and you get 5000 mg/years. You have plaque and ASCVD. Over 5000 mg/years and you have ASCVD. That’s the current threshold. And we know that if your LDL-C is above 60 mg/dL, then you are laying down plaque.
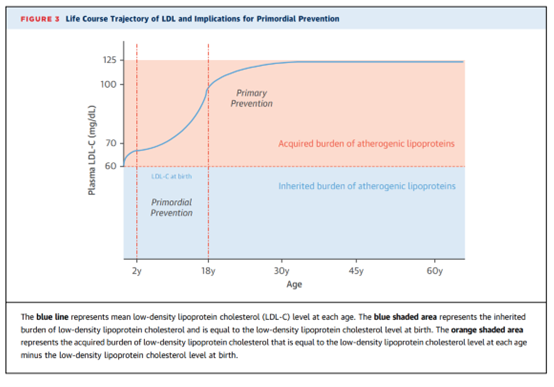
Again, here we are stressing primordial prevention. Once your LDL-C is above 60 mg/dL, on a long enough time horizon, your odds of having ASCVD increase.
Read the full article, it’s free access:
https://www.jacc.org/doi/pdf/10.1016/j.jacc.2018.06.046
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















