

HRT, DVT, VTE, And Heart Disease Risk Of Hormone Replacement Therapy
Jan 11, 2026
Perimenopause, Hormone Therapy, and Heart Health: What Women Need to Know
For many women, perimenopause is the first time heart health becomes a personal concern. Symptoms such as heart palpitations, anxiety, sleep disruption, fatigue, and brain fog often appear in the mid to late 30s and 40s and raise understandable fears about cardiovascular disease. Understanding how perimenopause, hormone therapy, heart disease, and blood clot risk intersect is essential for safe and informed decisions.
How Perimenopause Affects Cardiovascular Risk
Perimenopause is marked by fluctuating estrogen levels and declining progesterone, rather than a steady hormone decline. These hormonal changes affect blood vessels, lipid metabolism, insulin sensitivity, inflammation, and the autonomic nervous system. As women approach menopause, cholesterol levels often rise, blood pressure may increase, and cardiovascular risk accelerates. Heart disease becomes the leading cause of death in women after menopause, making this transition a critical prevention window.
Women also see a decrease in testosterone, see the article on Women and Testosterone.
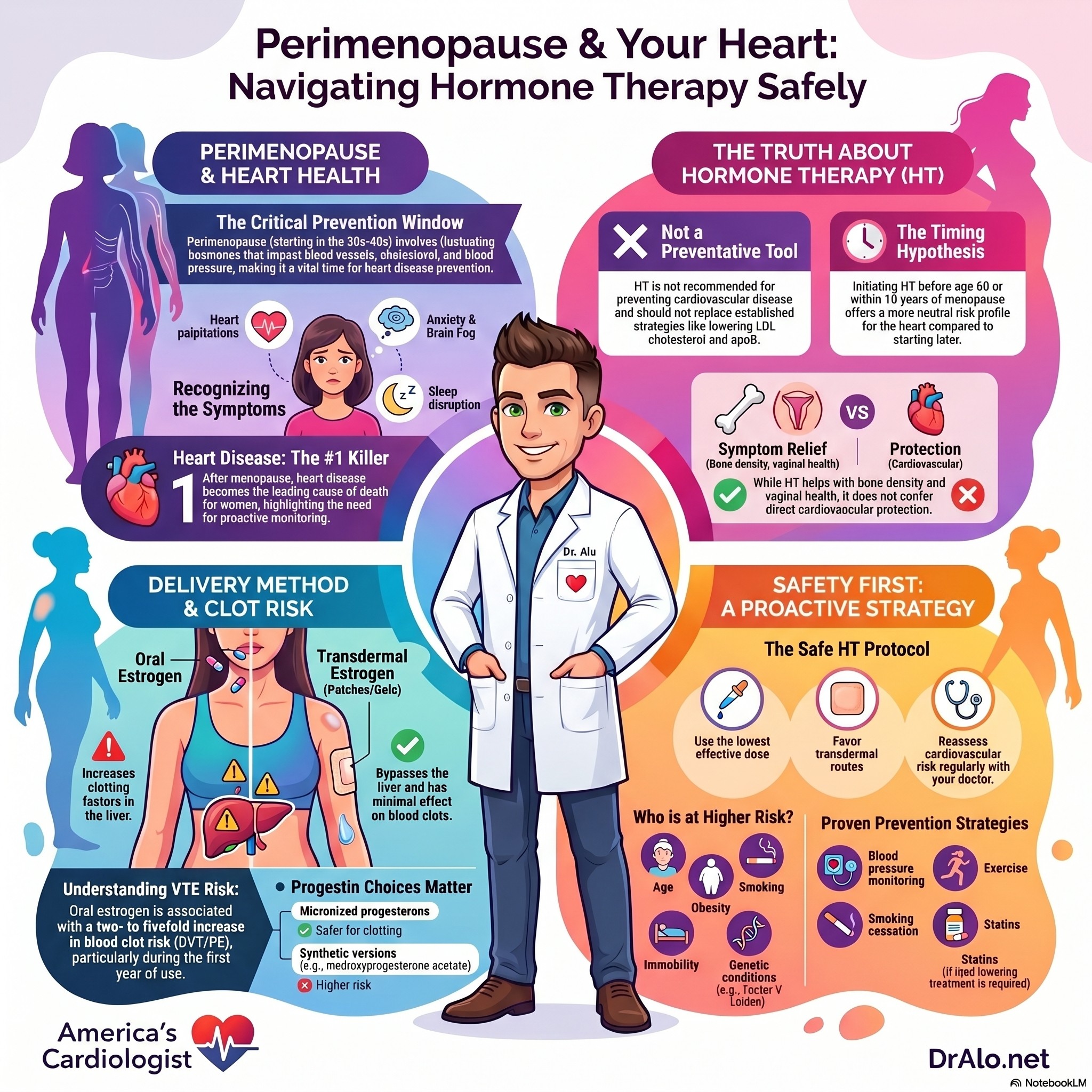
HRT and Heart Disease Infographic Summary:
Does Hormone Therapy Prevent Heart Disease?
While hormone therapy is beneficial, it is not to be used as a preventative medication for heart disease. The data does not support that. Hormone therapy is not recommended for the prevention of cardiovascular disease. Large randomized trials, including the Women’s Health Initiative, did not demonstrate heart disease prevention benefits and showed increased risks in certain populations. Hormone therapy should not be used as a substitute for established cardiovascular prevention strategies, like lowering apoB and LDL cholesterol for prolonged periods of time.
The Timing Hypothesis and Hormone Therapy
Research supports the timing hypothesis, also known as the window of opportunity. Women who initiate hormone therapy before age 60 or within 10 years of menopause tend to have lower absolute cardiovascular risk compared with women who start therapy later. However, early initiation does not confer cardiovascular protection. Instead, it suggests a more neutral risk profile when hormone therapy is used appropriately for symptom relief. If you have symptoms in your 30s and 40s, it may be better to start therapy sooner, rather than waiting until menopause completion. Many of the effects of menopause are less likely to improve when starting later, like decreased bone mineral density and vaginal atrophy.
Why Route of Hormone Therapy Matters
The route of estrogen administration plays a major role in cardiovascular and clotting risk. Oral estrogen undergoes first-pass metabolism in the liver, increasing clotting factors and inflammatory markers. Transdermal estrogen bypasses the liver and has minimal effects on coagulation pathways. As a result, transdermal estrogen is generally preferred for women with cardiovascular risk factors when hormone therapy is indicated. People who are more prone to clotting or have an inherited clotting disorder are more prone to this.
Deep Vein Thrombosis and Blood Clot Risk With Hormone Therapy
Systemic hormone therapy can increase the risk of venous thromboembolism, including deep vein thrombosis and pulmonary embolism (clots in your legs or lungs). Oral estrogen is associated with an approximately two- to fivefold increased risk, particularly during the first year of therapy. Combined estrogen-progestin therapy carries higher risk than estrogen alone. In contrast, large observational studies show no significant increase in clot risk with transdermal estrogen. The risk is higher in those with a known genetic clotting disorder. Many women may not known they have a clotting condition until they have their first clot.
The magnitude of VTE risk with HRT has been consistently demonstrated across multiple large-scale studies. In the Women's Health Initiative trials, combined estrogen-progestin therapy increased deep vein thrombosis risk by 87% (HR 1.87) and pulmonary embolism risk by 98% (HR 1.98) over 5.6 years. Estrogen-alone therapy showed a more modest but still significant 48% increase in DVT risk (HR 1.48), though pulmonary embolism risk was not significantly elevated.

How Progestin Type Influences Clot Risk
The type of progestin used in combination therapy influences thrombotic risk. Micronized progesterone appears to have a more favorable clotting profile, while some synthetic progestins, such as medroxyprogesterone acetate, are associated with higher venous thromboembolism risk. Progestin choice should be individualized based on patient risk factors.
Who Is at Higher Risk for Blood Clots
Certain factors significantly increase clot risk when hormone therapy is used. These include increasing age, obesity, smoking, immobility, recent surgery or fracture, personal or family history of blood clots, and inherited clotting disorders such as Factor V Leiden and others. In these cases, careful risk assessment and consideration of non-hormonal therapies are essential.
Using Hormone Therapy Safely During Perimenopause
Hormone therapy may be appropriate for symptom relief in selected perimenopausal and recently menopausal women. Safe use involves selecting the lowest effective dose, favoring transdermal estrogen, choosing appropriate progestins when needed, and reassessing cardiovascular and clotting risk regularly. Hormone therapy should not be used to treat high cholesterol or prevent heart disease.
Perimenopause as a Window for Heart Disease Prevention
While hormone therapy does not prevent heart disease, perimenopause is an ideal time to focus on cardiovascular prevention. Key strategies include regular blood pressure monitoring, cholesterol screening, physical activity, weight management, smoking cessation, sleep optimization, and stress management. Statins, not hormone therapy, are recommended when lipid-lowering treatment is indicated.
HRT And Heart Disease Bottom Line
Perimenopause is a time of both symptom confusion and rising cardiovascular risk. Hormone therapy decisions should be individualized, guided by timing, route, formulation, and patient risk factors. Understanding the balance between symptom relief, cardiovascular health, and blood clot risk allows women and clinicians to make informed, evidence-based choices.
References
- El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention. Circulation. 2020.
- Pinkerton JV. Hormone Therapy for Postmenopausal Women. New England Journal of Medicine. 2020.
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal Hormone Therapy and Risk of Cardiovascular Disease by Age and Years Since Menopause. JAMA. 2007.
- Newman CB, Blaha MJ, Boord JB, et al. Lipid Management in Patients With Endocrine Disorders. Journal of Clinical Endocrinology & Metabolism. 2020.
- Cho L, Davis M, Elgendy I, et al. Primary Prevention of Cardiovascular Disease in Women. Journal of the American College of Cardiology. 2020.
- Westfall E, Viere AB, Genewick JE. Preventing CVD in Women. American Family Physician. 2023.
- Shufelt CL, Manson JE. Menopausal Hormone Therapy and Cardiovascular Disease. Journal of Clinical Endocrinology & Metabolism. 2021.
- D'Costa Z, Spertus E, Hingorany S, et al. Cardiovascular Risk Associated With Menopause and Hormone Therapy. Current Atherosclerosis Reports. 2025.
- American College of Obstetricians and Gynecologists. Postmenopausal Estrogen Therapy: Route of Administration and Risk of Venous Thromboembolism. 2019.
- Canonico M, Plu-Bureau G, Lowe GDO, Scarabin PY. Hormone Replacement Therapy and Risk of Venous Thromboembolism. BMJ. 2008.
- Vinogradova Y, Coupland C, Hippisley-Cox J. Use of Hormone Replacement Therapy and Risk of Venous Thromboembolism. BMJ. 2019.
- Sweetland S, Beral V, Balkwill A, et al. Venous Thromboembolism Risk and Hormone Therapy. Journal of Thrombosis and Haemostasis. 2012.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















