

Mitral Valve Prolapse: Symptoms, Risks, and Treatments
Dec 29, 2025
Mitral Valve Prolapse: Everything You Need to Know (MVP Symptoms, Diagnosis & Treatment 2026)
Mitral valve prolapse affects 2–3% of the general population—that's roughly 170 million people worldwide. If you've been told you have MVP or suspect you might, this guide walks you through what it actually means for your heart health, why most people with MVP do just fine, and when you need to worry.
What Is Mitral Valve Prolapse (MVP)?
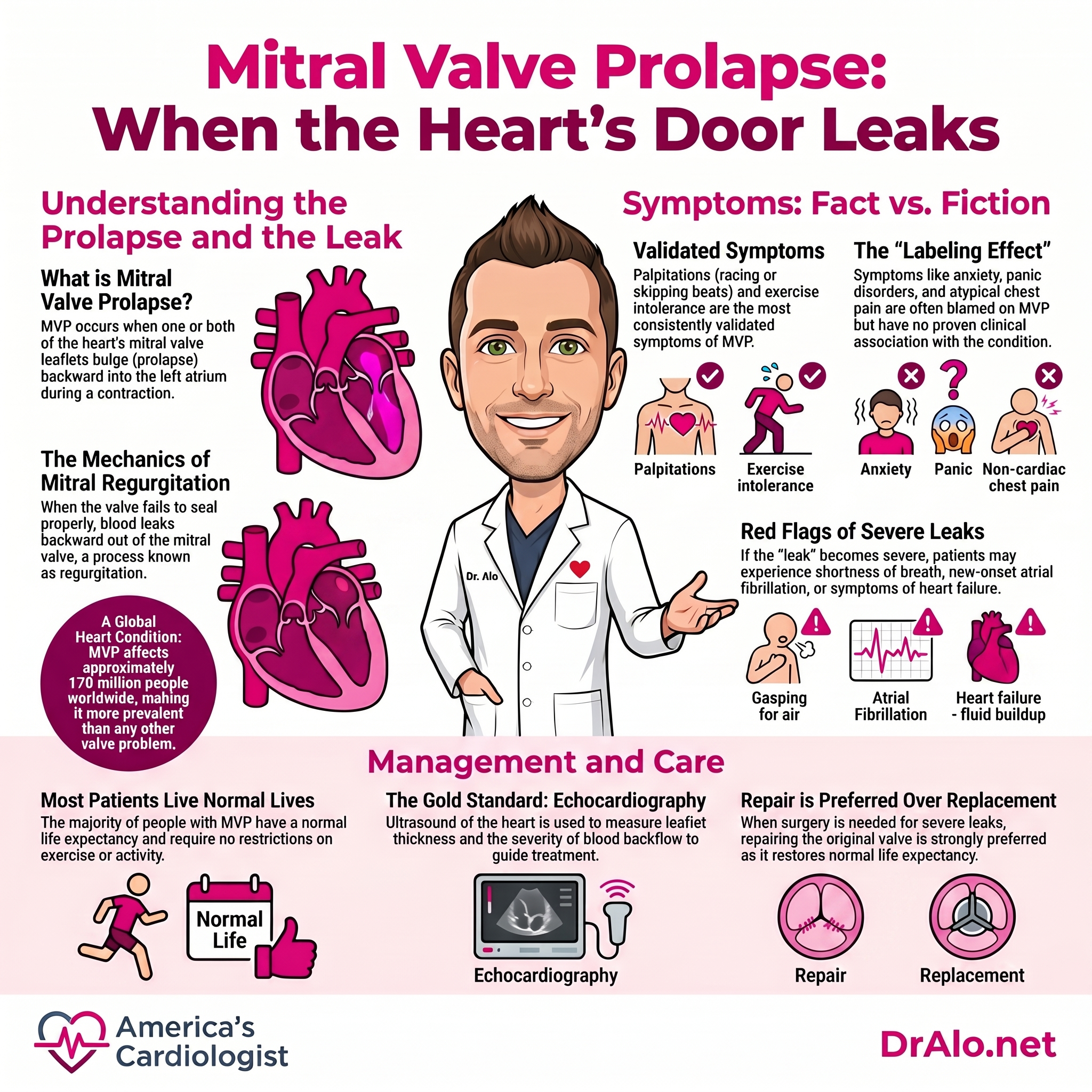
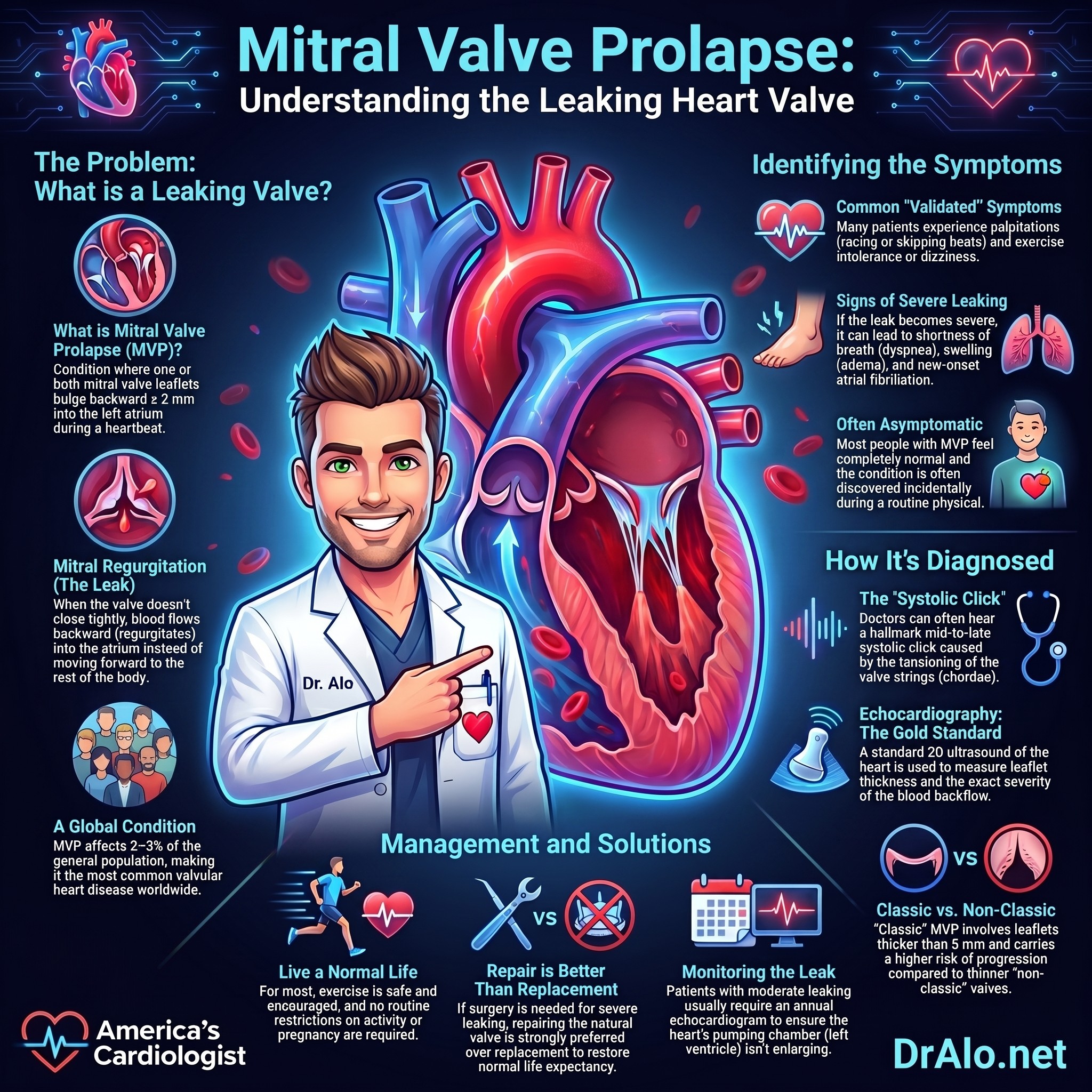
Mitral valve prolapse is a heart valve condition where one or both leaflets of your mitral valve bulge backward (prolapse) into your left atrium during the heartbeat. The diagnostic definition is straightforward: ≥2 mm systolic displacement of one or both leaflets superior to the annular plane, visible on echocardiography.
Here's the key thing to know right away: most people with MVP have an excellent prognosis and normal life expectancy. You won't need restrictions on exercise, and you can live a completely normal life. That said, a small subset does need closer monitoring because of progressive mitral regurgitation or arrhythmia risk.
MVP is the most common valvular heart disease in the world, making it more prevalent than aortic stenosis or any other valve problem. It affects men and women equally.
Infographic Summary:
Why MVP Happens: The Pathophysiology Behind the Condition
MVP isn't a defect you're born with in most cases. Instead, it develops because of fibromyxomatous changes—structural remodeling of the mitral valve leaflets themselves.
At the cellular level, several things happen:
Proteoglycan accumulation: The middle spongiosa layer (the "cushion" of the valve leaflet) swells from excessive proteoglycan buildup.
Collagen and elastin breakdown: The structural proteins that keep the valve leaflets strong deteriorate, making them more floppy.
Chordal abnormalities: The tiny strings (chordae tendinae) that anchor the leaflets can become stretched or abnormal.
Researchers have identified two main pathological subtypes:
Barlow disease: Thick, redundant leaflets with excessive connective tissue, often affecting both leaflets (bileaflet prolapse) and causing annular dilatation. More prone to progressive mitral regurgitation.
Fibroelastic deficiency: Thin leaflets with reduced proteoglycan, collagen, and elastin. Generally more benign but can progress with age.
The molecular drivers: At the molecular level, abnormal TGF-β (transforming growth factor-beta) signaling, mTOR pathway activation, and integrin-mediated cell-matrix interactions drive the myxomatous degeneration. This is why future therapies may target these pathways—researchers have shown that mTOR inhibition (rapamycin) can prevent progression in preclinical models.
MVP and Genetic Syndromes: Know Your Risk
While most MVP is primary (familial or sporadic), some people develop MVP as part of systemic connective tissue disorders:
Marfan syndrome (FBN1 mutations): Fibrillin-1 defects cause widespread connective tissue fragility, including the mitral valve.
Loeys-Dietz syndrome (TGF-β receptor mutations): Abnormal TGF-β signaling predisposes to valve and vascular disease.
Vascular Ehlers-Danlos syndrome (COL3A1 mutations): Type III collagen deficiency affects the valve and arteries.
If you have a family history of these conditions, or if you have skeletal features like pectus excavatum, tall stature with arachnodactyly, or skin hyperelasticity, genetic evaluation may be warranted.
MVP Symptoms: What You Actually Feel vs. What Gets Blamed on MVP
This is critical: most MVP patients are completely asymptomatic. The condition is often discovered incidentally during an echo for another reason, or during a routine physical with an auscultatory finding.
Validated MVP Symptoms
Palpitations: The most consistently validated symptom. Patients describe a sensation of heart racing, flopping, or skipping beats—usually benign premature atrial contractions (PACs) or sinus tachycardia triggered by anxiety or caffeine.
Exercise intolerance and orthostatic symptoms: Some patients with significant MVP report fatigue with exertion or dizziness with position changes.
Syncope/presyncope: Documented in case reports, though less common than palpitations. Usually associated with arrhythmias rather than hemodynamic compromise.
Symptoms Often Blamed on MVP (But Not Proven)
Case-control studies, including large Framingham data, have not confirmed a true association between MVP and the following—beyond ascertainment bias (the "labeling effect" where patients attribute pre-existing symptoms to their newly diagnosed condition):
✗ Chest pain (atypical, pleuritic, or reproducible on palpation)
✗ Anxiety or panic disorder
✗ Fatigue (unexplained)
✗ Dyspnea (shortness of breath at rest or minimal exertion)
If you have these symptoms, investigate other causes first (anxiety disorder, deconditioning, thyroid disease, anemia, GERD) rather than attributing them automatically to MVP.
Symptoms from Severe Mitral Regurgitation
If your MVP has progressed to severe mitral regurgitation (MR), you may develop:
• Progressive exertional dyspnea
• Exercise intolerance (reduced EF)
• Heart failure symptoms (orthopnea, edema)
• New-onset atrial fibrillation
These warrant urgent evaluation and likely surgical referral.
How MVP Is Diagnosed: Physical Exam and Imaging
The Classic Physical Exam Finding
The hallmark auscultatory finding is a mid-to-late systolic click, often followed by a high-pitched late systolic murmur. This click is caused by the sudden tensioning of the elongated chordae as the leaflet prolapses.
A key diagnostic skill: the click and murmur move with preload changes:
Valsalva maneuver or standing (decreased preload): The click moves earlier in systole, and the murmur lengthens.
Squatting or leg raise (increased preload): The click moves later in systole, and the murmur shortens.
This dynamic finding helps distinguish MVP from other cardiac murmurs that don't change with position.
If chordal rupture or a flail leaflet develops, the late systolic murmur becomes holosystolic (pans across all of systole), indicating severe MR.
Echocardiography: The Gold Standard
Two-dimensional transthoracic echocardiography (TTE) is the diagnostic standard. Key points:
Diagnostic criterion: ≥2 mm systolic displacement of one or both leaflets superior to the mitral annular hinge points in the long-axis view.
Why the long-axis view matters: The mitral annulus is saddle-shaped, not planar. Prolapse seen only in the four-chamber view without long-axis confirmation is NOT diagnostic and leads to false-positive MVP diagnoses. This is a common source of overdiagnosis.
MVP classification:
• Classic MVP: Leaflet thickness ≥5 mm (associated with fibromyxomatous disease, higher risk of progression)
• Non-classic MVP: Leaflet thickness <5 mm="" usually="" benign="" lower="" progression="" risk="" p="">
What else the echo assesses:
• Mitral regurgitation severity (none, trivial, mild, moderate, severe)
• Leaflet morphology and segmental involvement
• Left atrial and left ventricular dimensions
• Mitral annular disjunction (MAD)—abnormal separation of the annulus from the ventricular wall, linked to arrhythmia risk
• Left ventricular ejection fraction (LVEF)
Transesophageal Echocardiography (TEE)
TEE offers superior image quality and is superior for identifying specific prolapsing segments, particularly lateral scallop prolapse. It's used when TTE is inconclusive or when surgical planning is needed to assess repairability.
Cardiac MRI
Increasingly used for tissue characterization and arrhythmia risk stratification. CMR can detect:
• Myocardial fibrosis via late gadolinium enhancement (LGE), typically in the basal inferolateral wall and papillary muscles
• Myocardial inflammation
• Precise quantification of regurgitant volumes
Presence of myocardial fibrosis is increasingly recognized as a risk factor for arrhythmias in MVP—even in patients with mild MR—and helps stratify which patients need closer surveillance.
Complications: Who Needs to Worry and Why
Although the overall complication rate is approximately 2% per year, certain subsets are at higher risk. Understanding these helps guide surveillance and treatment decisions.
Progressive Mitral Regurgitation
Prevalence: Severe MR affects ~10% of MVP cohorts initially, but rises to ~25% with advancing age (lifetime risk).
Risk factors: Barlow disease (thick leaflets, bileaflet prolapse), chordal rupture, annular dilatation.
Clinical course: Asymptomatic MR can progress silently until left ventricular dilatation develops. Serial echo surveillance is essential for asymptomatic patients with moderate MR.
Infective Endocarditis
MVP with mitral regurgitation increases endocarditis risk compared to the general population. Patients with MVP and MR should receive endocarditis prophylaxis for high-risk dental or invasive procedures (per current guidelines).
Atrial Fibrillation
MVP is associated with increased AF risk, particularly in patients with:
• Significant mitral regurgitation (which dilates the left atrium)
• Left atrial enlargement on echo
• Advancing age
New-onset AF in an MVP patient warrants investigation for secondary causes and may trigger surgical referral if MR is moderate-to-severe.
Cerebrovascular Ischemic Events
There is an epidemiologic association between MVP and stroke, though the mechanism remains debated (paradoxical embolism via patent foramen ovale, arrhythmia-induced thromboembolism, or both). Anticoagulation decisions are individualized based on stroke risk factors.
Sudden Cardiac Death (The Arrhythmic MVP Phenotype)
This is the most feared complication, affecting a small but important subset: young women with specific features:
• Bileaflet prolapse (both leaflets involved)
• Mitral annular disjunction (MAD) on echo or CMR
• Myocardial fibrosis on CMR (LGE in inferolateral wall or papillary muscles)
• Palpitations with sustained or frequent premature contractions on monitoring
• Family history of sudden cardiac death in MVP
These patients are at increased SCD risk independent of mitral regurgitation severity—you can have "arrhythmic MVP" with trivial MR and still be at risk. Diagnosis of arrhythmic MVP warrants ICD evaluation and consideration of cardiac MRI screening.
Other Risk Factors for Complications
Patients at higher risk for overall cardiovascular events include those with:
• Moderate-to-severe MR
• Leaflet thickness >5 mm
• Flail leaflet (chordal rupture)
• LV dysfunction (LVEF ≤60%)
• LA enlargement
• Atrial fibrillation
• Pulmonary hypertension
• Male sex (counterintuitively, SCD is more common in young women, but overall mortality is higher in men)
• Age >50 years
Recent large cohort data (2026) in patients <65 years="" identified="" additional="" independent="" predictors="" of="" mortality:="" p="">
• Anterior MVP (higher risk than posterior)
• Mitral annular calcification (advancing atherosclerotic disease)
• Elevated pulmonary artery systolic pressure
Infographic Summary:
MVP Management: When to Watch, When to Treat, When to Refer for Surgery
Conservative Management (The Majority)
Asymptomatic patients with no or mild MR:
✓ No activity restriction; routine exercise is encouraged and beneficial
✓ No routine surveillance echos needed if examination findings are stable and MR is consistently mild
✓ Normal pregnancy and vaginal delivery are safe
Symptomatic patients (palpitations, orthostatic symptoms):
• Beta-blockers: First-line for palpitations, mild tachyarrhythmias, or increased adrenergic symptoms. Atenolol or metoprolol are reasonable choices.
• Caffeine, alcohol, and cigarette cessation: May be sufficient for symptom control in many patients. Caffeine is a potent trigger for PACs in MVP.
• Orthostatic symptoms: Managed with liberal fluid and salt intake, compression stockings, and rarely mineralocorticoid therapy (fludrocortisone) for refractory cases.
• Reassurance: Many MVP-related palpitations are benign PACs and do not indicate risk of serious arrhythmia or SCD. Holter or event monitoring can reassure if symptoms are frequent or patient anxiety is high.
Monitoring Intervals for Asymptomatic Patients with MVP
Mild MR, non-classic MVP: Repeat echo in 3–5 years (can lengthen intervals if stable).
Moderate MR or classic MVP: Annual echo surveillance.
Severe MR with preserved LV function: Serial echo every 6–12 months to detect LV dilatation or EF decline.
Surgical Intervention: When MVP Requires Surgery
Per the 2020 ACC/AHA Guidelines on Valvular Heart Disease, indications for mitral valve surgery in MVP include:
Class I (Definite benefit):
• Symptomatic patients with severe primary MR (any LVEF)
• Asymptomatic patients with severe MR + LV dysfunction (LVEF ≤60% or LVESD ≥40 mm)
Class IIa (Reasonable to consider):
• Asymptomatic patients with severe MR, preserved LV function, and >95% likelihood of durable repair with <1% operative mortality (centers with high MVP repair expertise)
• Severely symptomatic patients (NYHA III–IV) with high or prohibitive surgical risk (consider transcatheter edge-to-edge repair [TEER] if anatomy favorable)
Class IIb (May be considered):
• Asymptomatic patients with progressive LV enlargement or declining EF on ≥3 serial studies
Critical point: Mitral valve repair is strongly preferred over replacement when the cause is degenerative disease and a successful, durable repair is achievable. Repair:
• Restores normal life expectancy
• Markedly reduces heart failure risk when performed early
• Avoids the morbidity of long-term anticoagulation (mechanical prosthesis) or structural deterioration (bioprosthesis)
Success rates for MVP repair exceed 90% at experienced centers and are improving with robotic-assisted and minimally invasive approaches.
Transcatheter Edge-to-Edge Repair (TEER)
For severely symptomatic patients with high or prohibitive surgical risk, TEER (MitraClip, Pascal, or Evoque systems) is reasonable if:
• Anatomy is favorable for clip placement
• Life expectancy is ≥1 year
• Patient has failed or is not a candidate for medical therapy
TEER is less durable than surgical repair but offers a lower-risk alternative for elderly or frail patients.
Emerging Medical Therapies: The Future of MVP Treatment
Currently, there is no FDA-approved medical therapy to prevent MVP progression. However, exciting preclinical and translational research is underway:
mTOR inhibition (rapamycin): Preclinical studies in hypomorphic fibrillin-1 mice show that mTOR inhibitors can prevent TGF-β overactivity and myxomatous degeneration. Conserved transcriptomic signatures have been confirmed in human MVP specimens, raising hope for clinical translation within 5–10 years.
Serotonin pathway modulation: Being investigated for secondary MR prevention, particularly in Marfan syndrome (where serotonin signaling is abnormal).
TGF-β pathway inhibition: Targeted approaches to block abnormal TGF-β signaling, particularly relevant for syndromic MVP (Marfan, Loeys-Dietz).
These therapies remain investigational and are not yet available outside of clinical trials.
Follow-Up and Monitoring Strategy
Asymptomatic, mild or no MR: Clinical assessment at 3–5 year intervals; echo only if findings change on exam or symptoms develop.
Moderate MR, preserved LV function: Annual echo; refer for surgery evaluation if LV dilation (LVESD >40 mm) or EF decline develops.
Severe MR with preserved LV function: Refer for surgical evaluation; consider early surgery if >95% likelihood of durable repair at your institution.
Any MVP with recurrent palpitations or syncope: Ambulatory ECG monitoring (24-hour Holter, event monitor, or extended monitoring) to characterize arrhythmias and guide treatment.
Suspected arrhythmic MVP: Cardiac MRI for tissue characterization (look for LGE); consider EP study and ICD evaluation if high-risk features present.
The Bottom Line: MVP Is Usually Benign, but Individual Assessment Matters
If you have mitral valve prolapse:
✅ Most likely: You'll never develop symptoms or complications. Your life expectancy is normal.
✅ Exercise is safe and encouraged for cardiovascular health.
✅ Pregnancy is safe in MVP without severe MR.
⚠️ Get echocardiography to characterize your MVP—assess MR severity, leaflet thickness, LV function, and LA size.
⚠️ Avoid over-attribution of symptoms to MVP (chest pain, fatigue, anxiety are not proven MVP manifestations).
⚠️ If you have risk factors for complications (thick leaflets, moderate MR, LA enlargement, palpitations), arrange serial echo surveillance per guideline intervals.
⚠️ If you have arrhythmic MVP features (bileaflet prolapse, MAD, family history of SCD, frequent palpitations), ask your cardiologist about cardiac MRI and arrhythmia risk stratification.
The key is personalized risk assessment based on your specific echocardiographic and clinical findings—not a one-size-fits-all approach.
FAQ: Common MVP Questions
Q: Does MVP run in families?
A: Yes. Primary familial MVP occurs in some families with autosomal dominant inheritance patterns. If you have MVP, your first-degree relatives (parents, siblings, children) may benefit from screening with a stethoscope exam and possibly an echo. Syndromic MVP (Marfan, Loeys-Dietz, vascular EDS) definitely runs in families and warrants genetic evaluation.
Q: Can MVP cause sudden death?
A: Sudden cardiac death is rare in MVP overall (estimated <1% lifetime risk), but a subset with "arrhythmic MVP"—characterized by bileaflet prolapse, mitral annular disjunction, myocardial fibrosis, and young age—is at elevated risk. If you have these features, discuss ICD evaluation with your cardiologist.
Q: Should I take antibiotics before dental work?
A: Current guidelines recommend endocarditis prophylaxis only for MVP patients with mitral regurgitation (even mild) undergoing high-risk dental or invasive procedures. If your MVP is isolated without MR, prophylaxis is not needed. Always clarify with your cardiologist.
Q: Can MVP get worse?
A: MVP can progress, particularly in Barlow disease (thick leaflets). Progressive mitral regurgitation develops in 10–25% of MVP cohorts with aging. This is why serial echo surveillance is recommended for patients with moderate MR or classic (thick-leaflet) MVP.
Q: Is MVP dangerous during pregnancy?
A: MVP without severe MR is generally safe during pregnancy. Pregnancy causes increased blood volume and cardiac output, which may transiently worsen palpitations but does not increase obstetric or cardiac risk. Women with severe MR should discuss pregnancy planning with their cardiologist.
Q: Can I exercise with MVP?
A: Yes. Exercise is encouraged and beneficial for all MVP patients without severe MR. You can participate in competitive sports if you are asymptomatic with preserved LV function. No activity restriction is needed for the vast majority.
References
Hayek E, Gring CN, Griffin BP. Mitral Valve Prolapse. Lancet. 2005.
Related Cardiovascular Posts
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















