

Why Niacin Is No Longer Used For Heart Disease
Dec 29, 2025
Why Niacin Is No Longer Used for Heart Disease
Niacin, Cholesterol, and the Hard Lessons of Cardiovascular Outcomes
For decades, niacin (vitamin B3) was widely promoted as a treatment for cholesterol problems and cardiovascular disease. The logic seemed straightforward: niacin improves lipid numbers, lowering LDL cholesterol and triglycerides while significantly raising HDL cholesterol, so it must protect the heart.
Today, we know that logic was flawed.
Despite improving cholesterol measurements, niacin does not reduce heart attacks, strokes, or mortality. Worse, it can cause meaningful harm. As a result, niacin is no longer recommended in modern cardiovascular guidelines.
This article explains why.
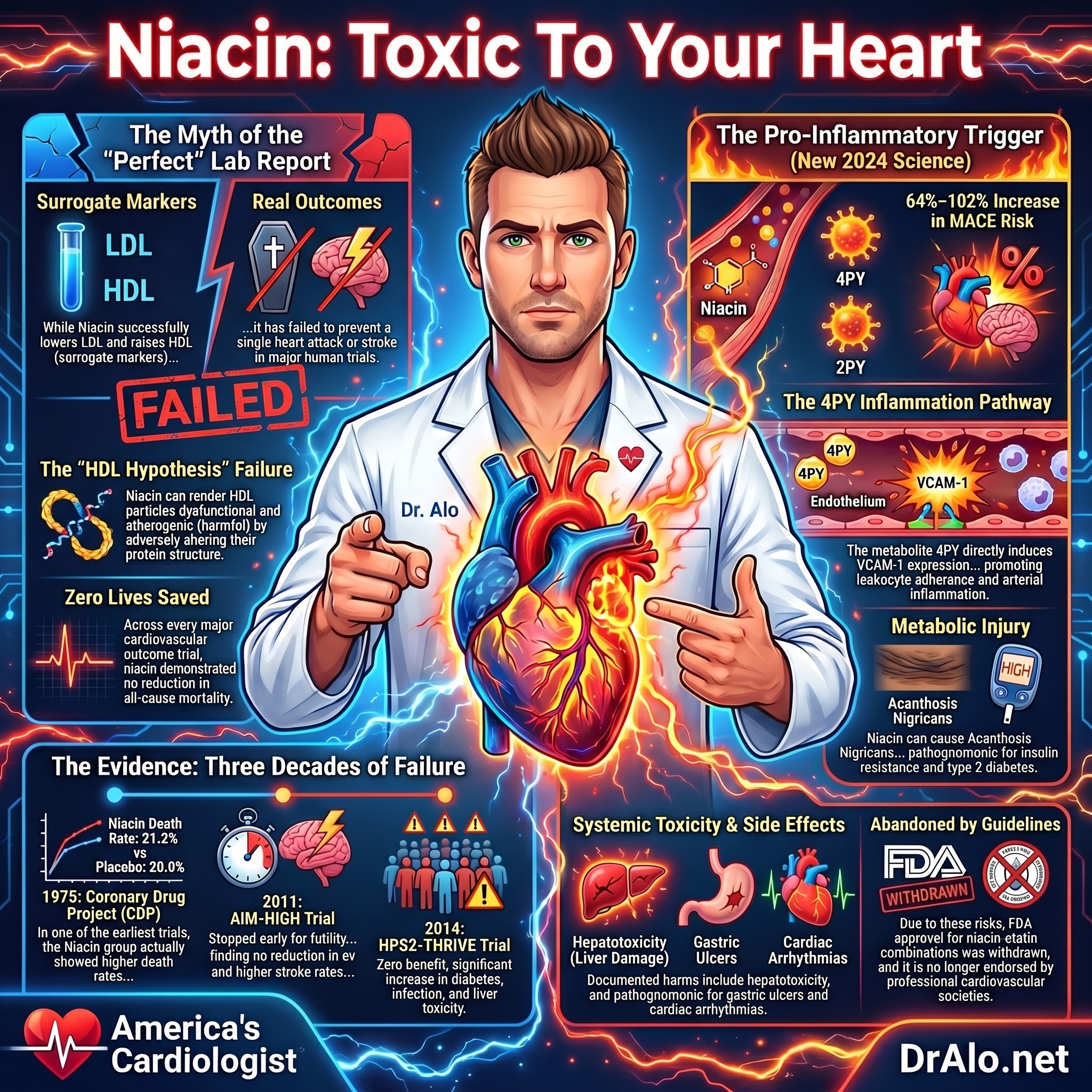
Infographic Summary:
Niacin Rumors vs Science
One of the rumors you hear online is that Niacin will fix your lipid problems. It’s a naturally occurring B vitamin, and the hope is that if you take large pharmacological doses, you’ll reduce your LDL-C, non-HDL-C, LDL-P, and apoB, while simultaneously increasing your HDL-C, and improve your heart health.
Wrong!
Niacin has failed multiple major human outcomes trials. Yes, it does raise HDL-C and lower LDL-C. But those changes did not prevent one heart attack nor stroke. Nor did they change mortality. Not one life was saved.
Niacin Failed Cardiovascular Trials:
Niacin failed to meet the primary endpoint in the three large randomized, double blinded clinical trials it was tested in:
(1) In the 1975 the Coronary Drug Project (CDP) the Niacin group had higher death rates than the placebo group after 5 years (21.2% versus 20.9%).
(2) In 2011 Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes (AIM-HIGH). More people on Niacin had strokes although the rate was low.
(3) In 2014 The Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE).
There have been numerous small angiographic trials with Niacin, but it’s the outcome trials that matter. Niacin is no longer recommended in any ASCVD guidelines. Not one trial showed improved outcomes.
Niacin Toxic and Causes Harm
In fact, the opposite was true. Niacin can cause acanthosis nigricans, a darkening of skin folds, which is a sign of insulin resistance and ultimately diabetes.
This is dark discoloration of the folds of the skin in the neck and armpit. It’s pathognomonic for insulin resistance and diabetes. Which means, if you have acanthosis nigricans, you have diabetes.
But there’s more.
Niacin is also associated with rash, severe flushing and itching, gastric ulcers, liver toxicity, and cardiac arrhythmias.
Niacin has been shown to adversely alter the proteome of HDL particles, rendering them dysfunctional. Which can make HDL particles more atherogenic due to the changes in proteins and expression of proteins that worsen CVD.
Read more on how Niacin worsened HDL-C atherogenicity:
https://www.ahajournals.org/doi/10.1161/ATVBAHA.121.316278
In an attempt to minimize the flushing and itching that’s so common with immediate release niacin, Kos pharmaceuticals developed an intermediate release form sold as Niaspan. It was later acquired by Abbott, but the drug fizzled out after failure to meet outcomes in AIM-HIGH and HPS-Thrive 2. The drug was never a commercial success. We used to prescribe this, but as Niacin failed human outcomes trials, we eventually stopped.
Although Niaspan is still on the market, because of its trial failures and removal from guidelines, no 3rd party payer will cover it. It has been withdrawn by the regulatory authorities in Europe.
A study published in February 2024 in Nature showed that the terminal metabolites of niacin, 2PY and 4PY, promote inflammation and contribute to cardiovascular disease risk. The metabolites 2PY and 4PY were shown to increase MACE by 64-102% over a three-year span. It appears they act through the soluble vascular adhesion molecules (sVCAM).
Study:
https://www.nature.com/articles/s41591-023-02793-8
A great review of the data on Niacin was published in Circulation:
Niacin: Time to Believe Outcomes Over Surrogate Outcomes
If Not Now, When?
https://www.ahajournals.org/doi/full/10.1161/CIRCOUTCOMES.116.003094
Niacin Produces Inflammatory Metabolites
The relationship between niacin metabolites and inflammation is nuanced, specific terminal metabolites of excess niacin (particularly 4PY) are pro-inflammatory and associated with increased cardiovascular risk, while niacin itself and some of its other metabolites are predominantly anti-inflammatory.
The Key Pro-Inflammatory Metabolite: 4PY
A landmark 2024 study in Nature Medicine by Ferrell et al. identified that the terminal niacin metabolites N1-methyl-4-pyridone-3-carboxamide (4PY) and N1-methyl-2-pyridone-5-carboxamide (2PY), breakdown products of excess niacin, were associated with increased major adverse cardiovascular events (MACE) across three independent cohorts:
-
4PY: adjusted HR 1.89 (95% CI 1.26–2.84) in the US validation cohort and 1.99 (1.26–3.14) in the European cohort
-
2PY: adjusted HR 1.64 (1.10–2.42) and 2.02 (1.29–3.18), respectively
The proposed mechanism involves vascular inflammation through VCAM-1 upregulation. In murine models, physiological levels of 4PY (but not 2PY) directly induced VCAM-1 expression on vascular endothelium and promoted leukocyte adherence — a critical early step in atherogenesis. Both metabolites were significantly correlated with soluble VCAM-1 levels in human cohorts, and a genetic variant (rs10496731) associated with 2PY/4PY levels was also linked to sVCAM-1 in a meta-analysis of ~106,000 individuals.
Study:
https://pubmed.ncbi.nlm.nih.gov/38374343
The Niacin Myth: “Fix Your Lipids, Fix Your Heart”
One of the most persistent claims online is that niacin can fix cholesterol and improve heart health.
Niacin is a naturally occurring B vitamin, and at pharmacologic doses it can:
- Lower LDL-C
- Lower non-HDL-C
- Lower LDL particle number (LDL-P)
- Lower apolipoprotein B (apoB)
- Raise HDL-C
The assumption is that these changes must reduce cardiovascular risk.
They don’t.
Niacin Improves Lab Numbers — Not Patient Outcomes
Yes, niacin reliably raises HDL cholesterol and lowers LDL cholesterol.
But across multiple large human outcomes trials:
- Not a single heart attack was prevented
- Not a single stroke was prevented
- No reduction in cardiovascular or all-cause mortality
- No lives were saved
In cardiology, outcomes, not theories or surrogate markers, determine whether a treatment works.
Niacin Failed Every Major Cardiovascular Outcomes Trial
Niacin has been rigorously tested. The results were consistent—and disappointing.
Coronary Drug Project (1975)
One of the earliest large randomized trials:
- After 5 years, mortality was higher in the niacin group
- Death rates: 21.2% with niacin vs 20.9% with placebo
Even in the pre-statin era, niacin failed to demonstrate benefit.
AIM-HIGH Trial (2011)
Studied niacin added to statin therapy in patients with:
- Low HDL-C
- High triglycerides
- Established atherosclerotic cardiovascular disease (ASCVD)
Results:
- No reduction in cardiovascular events
- Higher stroke rates in the niacin group (absolute numbers were low but concerning)
- Trial stopped early for futility
HPS2-THRIVE Trial (2014)
The definitive trial.
Over 25,000 high-risk patients were randomized to niacin plus statin therapy versus statin alone.
Results:
- No reduction in heart attacks
- No reduction in strokes
- No reduction in mortality
- Significant increases in serious adverse events, including diabetes, infection, bleeding, and liver toxicity
At that point, the evidence was unequivocal.
Surrogate Markers Don’t Save Lives
Niacin’s rise and fall underscores a critical lesson in medicine:
Improving lab values does not guarantee improved health.
Small angiographic or surrogate-endpoint studies once suggested benefit. But when hard outcomes were tested, niacin failed.
That is why:
- Niacin is not recommended in any contemporary ASCVD guideline
- FDA approval for niacin–statin combinations was withdrawn
- No professional cardiovascular society endorses its routine use
Niacin Can Cause Metabolic and Systemic Harm
Niacin is not a benign vitamin at pharmacologic doses.
One particularly telling adverse effect is acanthosis nigricans:
- Darkening and thickening of skin folds (neck, axillae)
- A finding pathognomonic for insulin resistance
- Strongly associated with type 2 diabetes
If acanthosis nigricans is present, metabolic injury has already occurred.
Additional documented adverse effects include:
- Severe flushing and itching
- Rash
- Gastric ulcers
- Hepatotoxicity
- Cardiac arrhythmias
- Worsening glycemic control and new-onset diabetes
In large trials, patients taking niacin were far more likely to discontinue therapy due to side effects.
Niacin Can Make HDL Dysfunctional
Niacin also exposed a fundamental flaw in the long-held “HDL hypothesis.”
While niacin raises HDL-C levels, it has been shown to adversely alter the proteome of HDL particles, rendering them dysfunctional.
This means:
- HDL cholesterol levels may increase
- HDL function may worsen
- Dysfunctional HDL may become more atherogenic, not protective
This helps explain why raising HDL-C with niacin did not improve cardiovascular outcomes.
📖 Reference:
https://www.ahajournals.org/doi/10.1161/ATVBAHA.121.316278
What Happened to Niaspan?
To reduce flushing seen with immediate-release niacin, extended-release niacin (Niaspan) was developed and later acquired by Abbott.
For a time, it was widely prescribed.
Then:
- AIM-HIGH failed
- HPS2-THRIVE failed
- Niacin was removed from guidelines
- Insurance coverage disappeared
Although Niaspan technically remains available, no third-party payer covers it, and it has no meaningful role in modern cardiovascular care.
Believe Outcomes Over Surrogate Endpoints
A landmark editorial in Circulation summarized niacin’s failure succinctly:
“Niacin: Time to Believe Outcomes Over Surrogate Outcomes — If Not Now, When?”
📖 Full article:
https://www.ahajournals.org/doi/full/10.1161/CIRCOUTCOMES.116.003094
This principle now defines evidence-based cardiology.
Final Clinical Bottom Line
Niacin:
- Improves cholesterol numbers
- Does not prevent heart attacks or strokes
- Does not reduce mortality
- Increases metabolic and systemic risk
- Increases inflammation
- Has failed every modern cardiovascular outcomes trial
That is why niacin is no longer recommended for the prevention or treatment of cardiovascular disease.
Modern cardiology is outcomes-driven, and niacin simply does not meet that standard.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















