

Comparing the US and European Cholesterol Guidelines: Who Got It Right?
Apr 13, 2026
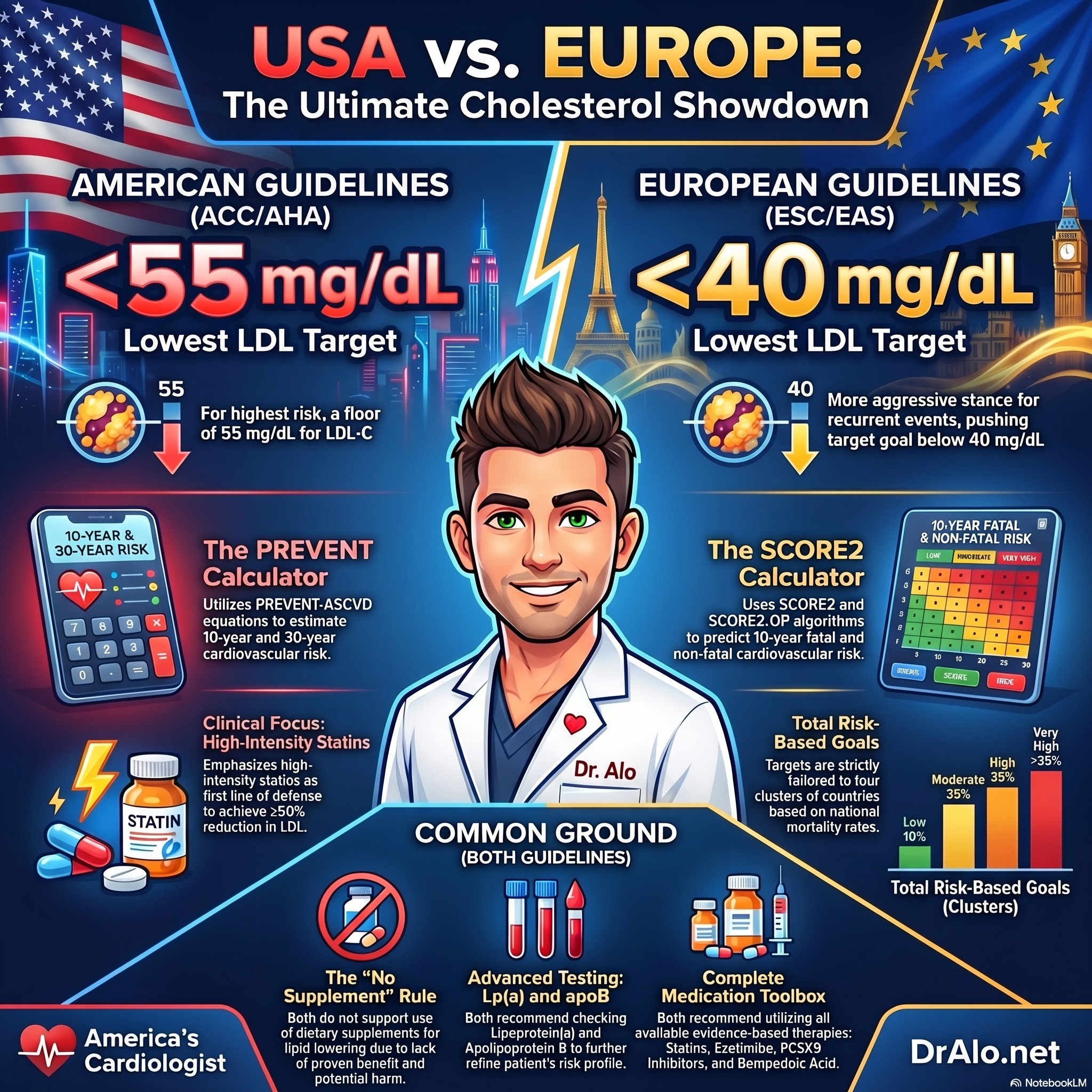
Comparing the ACC/AHA Guidelines To The European EAS Guidelines: Cholesterol Treatment
Just a few months apart, the Europeans and Americans have released Dyslipidemia Treatment Guidelines. They are getting closer to matching what myself and Dr. Thomas Dayspring published in 2023 in the Cholesterol TRUTHS book, but they need a few more tweaks.
So how do they compare?
And where do I disagree with them?
ACC/AHA Versus EAS Cholesterol Treatment Guidelines Infographic Summary:
The Cholesterol Guidelines Just Changed — Here's What You Need to Know
If you've ever had a conversation with your doctor about cholesterol, you've probably heard terms like LDL-C, statins, and cardiovascular risk. The medical societies that set the rules for how doctors manage cholesterol just released major updates, and as your cardiologist, I want to break down what changed, what it means for you, and why it matters.
In March 2026, the American College of Cardiology and American Heart Association released a brand new U.S. dyslipidemia guideline, the first complete overhaul since 2018. At the same time, the European Society of Cardiology and European Atherosclerosis Society published a 2025 update to their 2019 guidelines. These documents shape how cardiologists and primary care physicians around the world decide when and how aggressively to treat high cholesterol.
Bottom line: The guidelines are now more aggressive, more personalized, and more aligned across the Atlantic than ever before.
1. A New Way to Measure Your Risk — The PREVENT Equations
One of the biggest changes in the U.S. guideline is the replacement of the old Pooled Cohort Equations with the newer PREVENT equations (Predicting Risk of cardiovascular disease EVENTs). These new equations were built from more recent and more diverse American populations, so they give a more accurate picture of your individual risk.
What's really new is that PREVENT can now estimate both your 10-year risk AND your 30-year lifetime risk. This is a big deal for younger patients. If you're 42 years old and your 10-year risk looks low, your 30-year risk might tell a very different story, and your doctor now has a guideline-backed reason to act earlier.
The European guidelines use a different tool called SCORE2, which is well-validated across European populations. Both tools now categorize people into similar risk tiers, though the exact thresholds differ slightly due to the populations they were studied in.
The American guideline introduces a handy framework called the "CPR" approach: Calculate your 10-year risk, Personalize it with factors your risk score might miss (like family history or chronic inflammation), and Reclassify if there's still uncertainty, using a coronary artery calcium (CAC) scan.
Personally, I am not a fan of risk calculators. The do not predict risk accurately and still severely under estimate risk. The risk calculators go out of their way to give patients a "low score" thereby keeping them off meds. It appears they try their hardest to keep people off meds. We should be doing the opposite.
In my practice, everyone's LDL should be under 100. If you have one single risk factor, it should be under 70. If you have a cardiovascular event, it should be under 55. If you have repeat vents or lipoprotein a, you need to be under 40.
2. LDL-C Targets Are Back And Now Both Guidelines Agree
This is arguably the most important change in the U.S. guideline. The 2018 American guideline controversially moved away from specific LDL-C numbers and focused only on percentage reductions. That created confusion in practice. The 2026 guideline brings back specific LDL-C targets, and in doing so, finally aligns with how European cardiologists have been practicing for years.
Here's how the goals compare across both guidelines:
|
Risk Category |
ESC/EAS 2025 (European) |
ACC/AHA 2026 (American) |
|
Very High Risk (secondary prevention) |
<55 mg/dL + ≥50% reduction from baseline |
<55 mg/dL + non-HDL-C <85 mg/dL |
|
Very High Risk (recurrent events) |
<40 mg/dL may be considered |
Same very high risk category applies |
|
High Risk |
<70 mg/dL + ≥50% reduction |
<70 mg/dL + non-HDL-C <100 mg/dL |
|
Intermediate Risk (primary prevention) |
<100 mg/dL |
<100 mg/dL + non-HDL-C <130 mg/dL |
|
Borderline/Low Risk (primary prevention) |
Lifestyle first; drug if uncontrolled |
<100 mg/dL if statin started |
The European Guidelines add a lower LDL target of < 40 mg/dL for those with repeat cardiovascular events, are at severe risk, or have lipoprotein a. That's what I have recommended in my book for the last 3 years. It's nice to see the guidelines catching up to the science and clinical practice. The American guidelines have not yet added this very high risk category.
The American guideline also now formally adds non-HDL-C goals alongside LDL-C goals. Non-HDL-C captures all the "bad" cholesterol particles in your blood, not just LDL, making it a more complete measure of risk, especially if your triglycerides are elevated.
As a cardiologist who has always preferred ApoB as the most precise measure of atherogenic particle burden, I'm encouraged to see ApoB now formally recognized in both guidelines as a secondary target, particularly useful when LDL-C and non-HDL-C goals have been met but residual risk remains.
3. Coronary Artery Calcium Scoring Gets a Major Upgrade
A coronary artery calcium (CAC) scan is a low-dose CT scan that detects calcium buildup in your heart arteries, an early sign of atherosclerosis, before symptoms ever appear. Both guidelines endorse this test, but the 2026 American guideline goes much further than ever before.
Personally, if you have any amount of calcium, I am very aggressive. I want LDL below 55 mg/dL. I treat this like having prior ASCVD. It's decades too late, and we might as well be super aggressive now. If CAC in over 1000, I generally shoot for LDL < 40 mg/dL.
However, here is what the guidelines say:
For the first time, specific LDL-C treatment goals are now tied directly to your CAC score:
- CAC score ≥1,000 units: Treat as aggressively as someone who has already had a heart attack, LDL-C goal below 55 mg/dL
- CAC score 300–999: LDL-C goal below 70 mg/dL
- CAC score 100–299 or ≥75th percentile for your age and sex: LDL-C goal below 70 mg/dL
- CAC score 1–99: Moderate statin therapy, LDL-C goal below 100 mg/dL.
- CAC score of 0: It is reasonable to defer medication and recheck in 3–7 years, while focusing on lifestyle.
I vehemently disagree. If the LDL is high, we do not need to wait until we have end stage disease. Calcium is an end stage finding. It's decades too late.
The guidelines also now recommends acting on incidentally discovered CAC, calcium found during a chest CT or other scan done for a completely different reason. If your CT scan for something else picks up calcium in your coronary arteries, your doctor should now factor that into decisions about starting or intensifying cholesterol therapy. I would aim for an LDL < 55 for any incidental calcium.
Personally, I am not a fan of waiting until there is imaging proven ASCVD to treat aggressively. I would rather prevent heart disease before it forms. A CAC indicates late stage or end stage ACSVD when it is no longer reversible. It's the equivalent of allowing smokers to continue smoking until a CT chest shows cancer in their lungs. It's decades too late. We should have told them to stop smoking in their teens.
With that being said, the CAC score is still a useful tool in preventive cardiology, and it just got a formal, evidence-based treatment framework to go with it. Many of my patient come in with these tests that they ordered themselves.
4. Lipoprotein(a): Finally Getting the Attention It Deserves
Lipoprotein(a), or Lp(a), is a genetically determined cholesterol particle that about 20% of the population carries at elevated levels. It dramatically increases your risk of heart attack and aortic valve disease, and until recently, most routine lipid panels didn't even test for it.
The 2026 U.S. guideline makes testing Lp(a) at least once in every adult's lifetime a Class I (highest-level) recommendation. The European 2025 update similarly elevated the status of Lp(a), though it does not yet call for universal screening with quite the same strength.
The American guideline identifies two risk thresholds worth knowing:
- Lp(a) ≥125 nmol/L (50 mg/dL): Associated with about 1.4-fold increased ASCVD risk
- Lp(a) ≥250 nmol/L (100 mg/dL): Associated with 2-fold or greater increased risk
If your Lp(a) is elevated, both guidelines agree: the appropriate response is to more aggressively lower LDL-C and control all other modifiable risk factors. For patients with clinical heart disease and elevated Lp(a) who haven't reached their LDL-C goal on statins, adding a PCSK9 inhibitor (a powerful injectable cholesterol-lowering medication) is now formally recommended — in part because PCSK9 inhibitors can lower Lp(a) by 20–30% in addition to dramatically lowering LDL-C.
I personally recommend LDL < 40 mg/dL for all people with the Lp(a) mutation. Lp(a) is present in about 25% of all people.
Dedicated Lp(a)-lowering therapies are currently in late-stage clinical trials. If your Lp(a) is elevated, ask your doctor about it, and stay tuned, because this space is about to change significantly.
5. New Medications Enter the Picture
Both guidelines now formally incorporate several newer cholesterol-lowering agents beyond the classic statin-ezetimibe-PCSK9 inhibitor ladder:
Bempedoic acid (Nexletol)
An oral medication that works upstream of statins to lower LDL-C by about 23% on its own, and up to 38% when combined with ezetimibe. Crucially, it does not affect muscle tissue the same way statins do, making it a valuable option for people who cannot tolerate statins. The CLEAR Outcomes trial confirmed it reduces heart attacks and cardiovascular events. Both guidelines now give it strong recommendations.
Inclisiran (Leqvio)
A twice-yearly injectable medication that lowers LDL-C by about 50% by silencing the gene that produces PCSK9 in the liver. The 2026 U.S. guideline formally recommends it as an alternative to the monoclonal antibody PCSK9 inhibitors for patients who prefer less frequent dosing or who cannot access those medications. The European guidelines are holding off on a formal recommendation until ongoing cardiovascular outcomes trials report back in 2026–2027.
Olezarsen: New for Triglycerides Only For FC (Familial Chylomicronemia)
The 2026 U.S. guideline is the first to give olezarsen (an ApoC-III inhibitor) a Class I recommendation for patients with familial chylomicronemia syndrome, a rare condition with dangerously elevated triglycerides. This reflects the landmark ESSENCE-TIMI 73b trial data showing dramatic reductions in triglycerides and pancreatitis risk.
6. HIV, Cancer, and Chronic Kidney Disease: Underserved Patients Finally Get Clear Guidance
Both guidelines have now elevated statin therapy to a Class I recommendation for people living with HIV aged 40–75 who are on stable antiretroviral therapy, based on the REPRIEVE trial showing a 35% reduction in major cardiovascular events with pitavastatin.
The 2026 U.S. guideline goes further by creating dedicated guidance for:
- Cancer survivors with at least 2 years of life expectancy: Should be treated the same as people without cancer history if they otherwise qualify for cholesterol therapy
- Chronic kidney disease stage 3 or higher with known heart disease: LDL-C goal below 55 mg/dL with high-intensity statin plus ezetimibe and/or PCSK9 inhibitor
7. Dietary Supplements: Both Guidelines Now Say "No"
One area where the guidelines have become crystal clear, and where I've been vocal for years, is dietary supplements. The SPORT trial was a landmark study that directly compared low-dose rosuvastatin (a statin) against fish oil, cinnamon, garlic, turmeric, plant sterols, and red yeast rice in people at elevated cardiovascular risk. The result: rosuvastatin dramatically lowered LDL-C; none of the supplements produced any significant LDL-C reduction compared to placebo.
Both the 2025 European and 2026 American guidelines now carry explicit Class III (not recommended) ratings for dietary supplements as LDL-C or triglyceride-lowering therapy. This includes red yeast rice, fish oil at standard doses, berberine, and others. If you are spending money on cholesterol-lowering supplements instead of, or as a substitute for, proven medications, you are not protecting your heart, and your doctor's guidelines now explicitly say so.
Supplements are not a substitute for statins. This is no longer just my opinion, it is the consensus of every major cardiovascular guideline in the world.
8. Treating Earlier, Especially for Young Adults
One theme running through the entire 2026 U.S. guideline is the importance of preventing the cumulative damage that comes from decades of exposure to elevated cholesterol. Atherosclerosis begins in childhood, builds slowly and silently for decades, and then strikes.
The guideline now includes new recommendations for young adults aged 30–59 with low 10-year risk but an LDL-C of 160–189 mg/dL, or a 30-year risk of 10% or higher. For these patients, starting a moderate-intensity statin to reduce their cumulative lifetime exposure to atherogenic lipoproteins is now considered reasonable, even if their near-term risk looks low on paper.
This is a paradigm shift toward lifetime cardiovascular health rather than just treating what's in front of us today.
Cholesterol Guidelines Bottom Line
Here is what I want you to take away from all of this:
- Get your Lp(a) measured at least once. Ask your doctor for it if it hasn't been checked.
- If you've had a heart attack, stroke, or stent, your LDL-C goal is below 55 mg/dL. If you're not there, escalate your treatment.
- A CAC score of zero is powerful reassurance. A high CAC score is an urgent call to act, even without symptoms.
- Supplements will not protect your heart. Proven medications will.
- If you're younger and your family history worries you, ask about your 30-year risk, not just your 10-year risk.
These guidelines represent years of evidence from hundreds of clinical trials and hundreds of thousands of patients. My job, and the job of every preventive cardiologist, is to translate that evidence into action for you. If you have questions about where you stand, reach out. This is exactly the conversation we should be having.
References
- Blumenthal RS et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia. Circulation. 2026;153. doi: 10.1161/CIR.0000000000001423
- Mach F, Koskinas KC, Roeters van Lennep JE, et al. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur Heart J. 2025;46:4359-4378. doi: 10.1093/eurheartj/ehaf190
- Mach F et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur Heart J. 2020;41:111-188. doi: 10.1093/eurheartj/ehz455
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















