

Repatha For Primary Prevention? The Data Is In!
May 18, 2026
Can You Use Repatha If You Have Never Had A Heart Attack?
A new study in the New England Journal of Medicine has the answer. And it's not what we expected. For many years we have been using Repatha to lower the chance of repeat heart attacks and strokes in people who have already had them. Now, it looks like we can use it in those who have never had one, to prevent one altogether.
Primary vs Secondary Prevention
For decades, the medical community has drawn a clear line between two types of cardiovascular care: helping people who have already had a heart attack or stroke (secondary prevention) and protecting those who haven't yet experienced one (primary prevention). A new landmark clinical trial called VESALIUS-CV is now blurring that line, showing that an injectable cholesterol-lowering medication called evolocumab, sold under the brand name Repatha, can significantly reduce the risk of a first major cardiovascular event in high-risk patients.
This review breaks down what the trial found, why it matters, and what it could mean for the future of heart disease prevention.
What Is Repatha, and How Does It Work?
To understand why this trial is such a big deal, it helps to know a little about cholesterol and how the body manages it.
Low-density lipoprotein cholesterol, commonly known as LDL-C or "bad cholesterol," plays a central role in the development of atherosclerosis, the buildup of fatty plaques inside artery walls. Over time, these plaques can rupture, triggering blood clots that block blood flow to the heart (causing a heart attack) or the brain (causing a stroke).
The body has a natural system for clearing LDL-C from the bloodstream. Liver cells have receptors on their surface that grab LDL particles and pull them out of circulation. However, the body also produces a protein called PCSK9 (proprotein convertase subtilisin/kexin type 9), which breaks down those receptors. Think of it as a recycling problem: PCSK9 destroys the very tools the liver uses to clean up cholesterol.
Repatha is a monoclonal antibody, a lab-made protein designed to target and neutralize PCSK9. By blocking PCSK9, Repatha allows more LDL receptors to survive on liver cells, which means the liver can pull more LDL-C out of the blood. The result is a dramatic drop in LDL-C levels, often by 50 to 60% on top of what statins (the most commonly used cholesterol drugs) can achieve.
The VESALIUS Repatha Trial
The VESALIUS-CV trial, published in the New England Journal of Medicine in November 2025, is a landmark study that changes how we think about PCSK9 inhibitors. In a double-blind, randomized, placebo-controlled trial of 12,257 patients with atherosclerosis or high-risk diabetes who had never had a heart attack or stroke, evolocumab (140 mg every two weeks) reduced the risk of cardiovascular death, MI, or ischemic stroke by 25% over a median follow-up of 4.6 years. LDL cholesterol dropped from a median of 115 mg/dL at baseline down to 45 mg/dL in the treatment group. That is a 55% reduction on top of already being on a high-intensity lipid-lowering regimen. The absolute risk reduction for the 3-point MACE endpoint was 1.8%, and when revascularization was added as a fourth endpoint, the absolute benefit grew to 2.8%. No new safety signals were identified. This trial is the first to show that a PCSK9 inhibitor can prevent a first cardiovascular event, not just a recurrent one, and that is a major clinical distinction.
Infographic Summary:
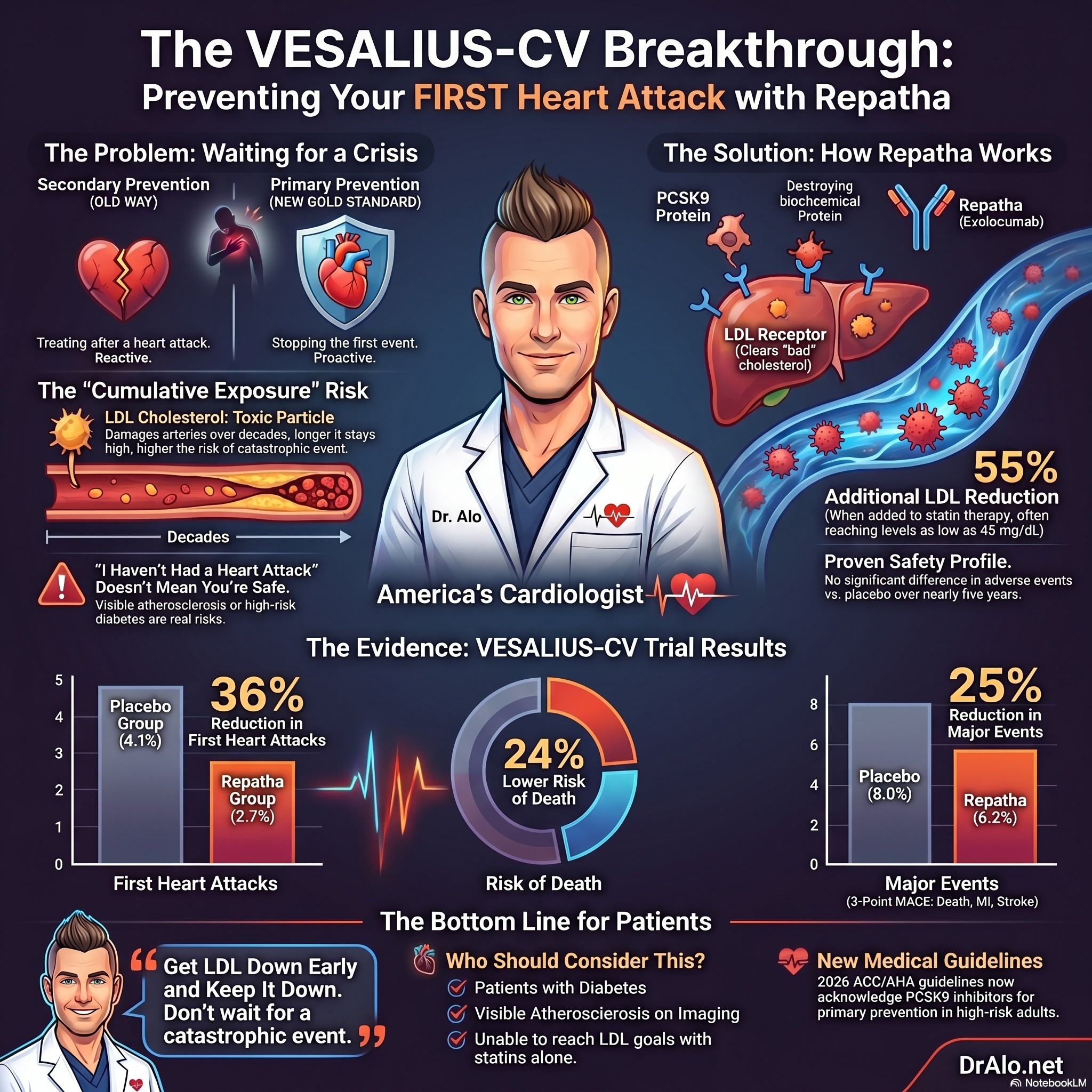
VESALIUS-CV: PCSK9 Inhibitors Now Proven for Primary Prevention
For years I have had a simple message for my patients who have heart disease risk but have never had a heart attack or stroke: get your LDL down early, keep it down, and do not wait for a catastrophic event to take this seriously. The VESALIUS-CV trial, published in the New England Journal of Medicine in November 2025 and presented at the American Heart Association Scientific Sessions, now gives us the hard clinical trial data to back that up with one of the most powerful LDL-lowering drugs we have.
Let me walk you through what happened, what it means, and why I think this changes how we practice preventive cardiology.
What Was VESALIUS-CV?
VESALIUS-CV was a large, international, double-blind, randomized, placebo-controlled trial. That means patients, doctors, and researchers did not know who was getting the real drug and who was getting a placebo. It enrolled 12,257 patients with established atherosclerotic cardiovascular disease or high-risk diabetes who had an LDL cholesterol of at least 90 mg/dL and, critically, had never had a heart attack or stroke.
The drug being tested was evolocumab (brand name Repatha), a PCSK9 inhibitor given as 140 mg injected under the skin every two weeks. Patients were followed for a median of 4.6 years.
The population had a median age of 66. Roughly 43% were women. Most, about 93%, were white, which is a limitation worth noting.
What Did the Trial Find?
The trial had two co-primary endpoints. The first was a 3-point composite of death from coronary heart disease, heart attack, or ischemic stroke. The second added ischemia-driven revascularization to make it a 4-point composite.
The results were clear on both endpoints. Take a look at the chart. Repatha is Evolocumab. You'll notice the placebo group had significantly more events than the treatment group, and the p values were all below 0.001, which means it was statistically significant and not due to chance. MACE stands for Major Adverse cardiovascular Event and usually means; heart attack, stroke, peripheral artery disease, stents, open heart surgery with bypass, and anything else involving the cardiovascular system that is "ischemic" (due to a lack of blood flow in the arteries).
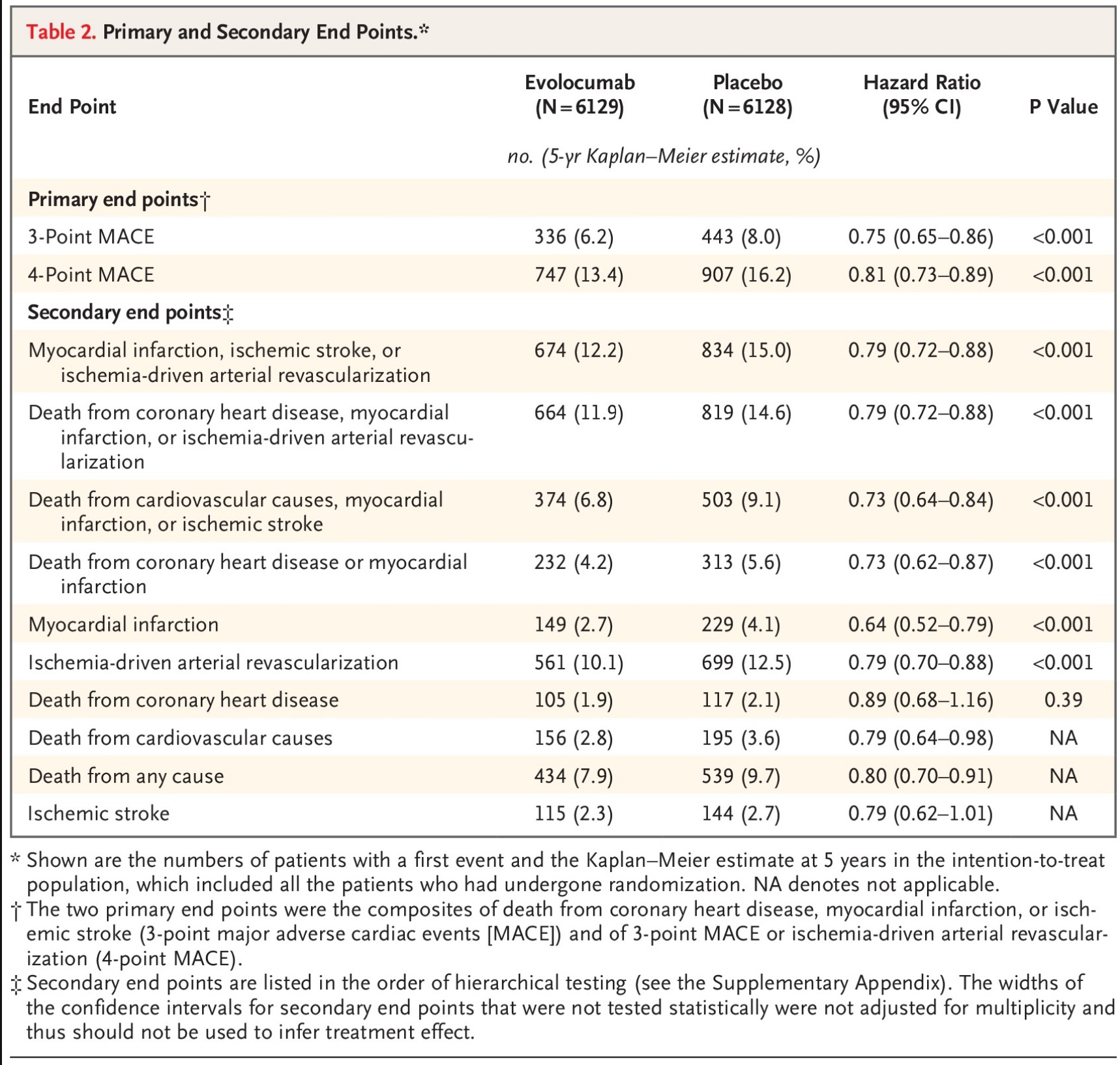
For 3-point MACE, the event rate was 6.2% in the evolocumab group compared to 8.0% in the placebo group. That translates to a 25% relative risk reduction and a 1.8% absolute risk reduction over the follow-up period.
For 4-point MACE, evolocumab produced a 19% relative risk reduction and a 2.8% absolute risk reduction.
Risk of a first heart attack specifically was cut by 36%.
On the lipid side, evolocumab lowered LDL cholesterol by approximately 55% on top of existing statin therapy. The median LDL in the evolocumab group at 48 weeks was 45 mg/dL, compared to 109 mg/dL in the placebo group. That is a profound difference, and it is a direct reflection of the cumulative LDL exposure hypothesis I talk about constantly: the lower you go, and the longer you stay there, the more you protect the arteries.
Importantly, the benefit was consistent across key subgroups, including the roughly one-third of patients who had high-risk diabetes without qualifying atherosclerotic disease. No new safety signals were identified.
The Results: A Clear Win for Prevention
The primary endpoint of the trial, the main outcome researchers were looking for, was a composite of three major adverse cardiovascular events (3-point MACE): death from coronary heart disease, heart attack, or ischemic stroke. The results were striking:
-
3-point MACE occurred in 6.2% of the Repatha group compared to 8.0% of the placebo group, representing a 25% relative risk reduction (hazard ratio 0.75).
-
When the endpoint was expanded to include coronary revascularization procedures (such as stenting or bypass surgery), the so-called 4-point MACE, the rates were 13.4% vs. 16.2%, a 19% relative risk reduction (hazard ratio 0.81).
-
Heart attacks alone were reduced by 36% (2.7% vs. 4.1%).
-
An exploratory analysis even suggested a 24% reduction in all-cause mortality (7.9% vs. 9.7%), though this was not a prespecified primary endpoint and should be interpreted with some caution.
All of these differences were statistically significant, meaning they were very unlikely to be due to chance.
Repatha Reduced All Cause Mortality
It's interesting to note, that Repatha reduced the risk of dying from any cause as well. Take a look at "All-cause death" below. You'll also notice that every single endpoint favored evolocumab and nearly all of the confidence intervals were on the left side, meaning likelihood this was due to chance is quite low.
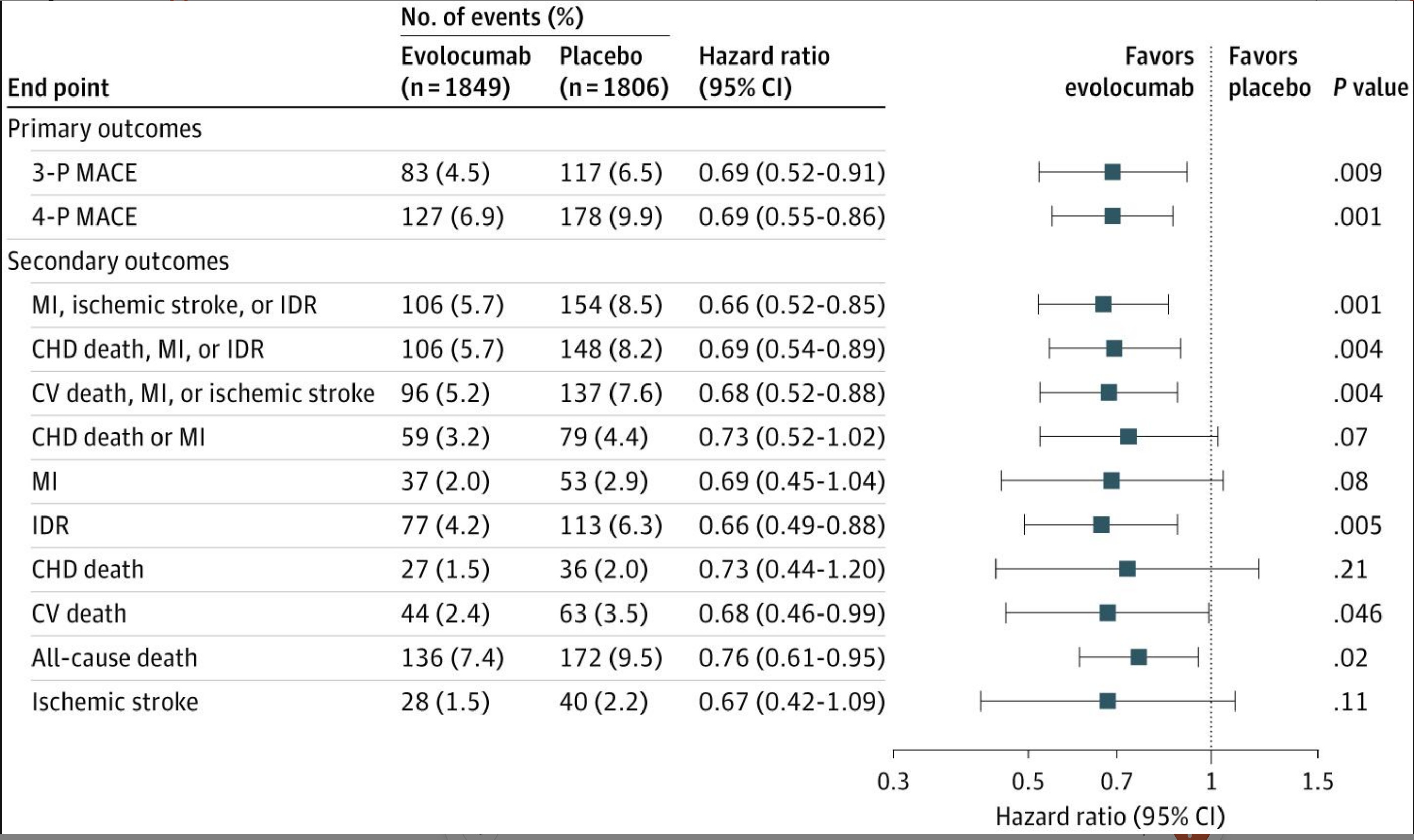
The all cause mortality benefit was quite surprising, because most cardiovascular outcomes trials aren't powered to resolve differences in all cause mortality, because they aren't long enough, or don't have enough participants. But this trial showed a 24% reduction in all cause mortality or the chance of dying from any cause. Which is pretty significant. And the confidence interval on that finding was the tightest of the above findings. Pretty impressive.
What the Guidelines Say Now
The 2026 ACC/AHA Dyslipidemia Guideline, published around the same time as the VESALIUS-CV results, assigns a Class 2b recommendation for adding a PCSK9 monoclonal antibody in primary prevention adults who are at 10% or greater 10-year risk of cardiovascular disease and who have not achieved an LDL-C below 70 mg/dL despite maximally tolerated statin therapy with or without ezetimibe. A Class 2b recommendation means the treatment "may be reasonable," not the strongest endorsement, but an acknowledgment that there is supporting evidence. Notably, the guideline was largely written before the full VESALIUS-CV results were available, so future updates may strengthen this recommendation.
Why This Matters: Rethinking the Primary vs. Secondary Prevention Divide
Traditionally, the medical community has set different LDL-C targets depending on whether a patient has already had a cardiovascular event. Secondary prevention patients are typically pushed toward LDL-C levels below 70 mg/dL (or even below 55 mg/dL in some European guidelines), while primary prevention patients have had more relaxed targets.
VESALIUS-CV challenges this framework. The trial suggests that high-risk primary prevention patients, particularly those with diabetes, may benefit from the same aggressive LDL-C lowering (down to 40 to 55 mg/dL) that was previously reserved for patients who had already suffered a heart attack or stroke. The data imply that the biology of atherosclerosis does not care whether a patient has had a prior event; what matters is the cumulative exposure of arteries to LDL-C over time.
Safety: No Major Red Flags
One of the common concerns with aggressively lowering cholesterol is whether it might cause harm. After all, cholesterol is a building block for cell membranes and hormones. Reassuringly, VESALIUS-CV found no significant difference in adverse events between the Repatha and placebo groups over nearly five years of follow-up. This is consistent with earlier safety data from a Cochrane systematic review, a rigorous, independent analysis, that found a favorable safety profile for PCSK9 monoclonal antibodies.
What I Want You to Take Away
First, LDL is not just a number on a lab report. It is cumulative biological exposure to a toxic particle that damages arterial walls over decades. Every year your LDL stays elevated is a year of atherogenic injury. The earlier you intervene and the lower you get, the better.
Second, "I haven't had a heart attack" does not mean "I'm fine." If you have atherosclerosis visible on imaging, or if you have high-risk diabetes with elevated LDL despite being on a statin, you are at real risk of a first major event. That first event can kill you. The whole point of preventive cardiology is to make sure it never happens.
Third, PCSK9 inhibitors work. They are safe. They have now been proven in multiple large randomized trials. If your LDL is not at goal on a statin alone, or on a statin plus ezetimibe, adding a PCSK9 inhibitor is a legitimate and evidence-supported next step. One fair criticism of VESALIUS-CV is that only about 20% of patients were on ezetimibe. Ezetimibe is cheap, generic, and should be exhausted before escalating to a PCSK9 inhibitor for most patients. But when you need the big gun, you now have data showing it saves lives even before the first catastrophic event.
Why This Matters
Before this trial, we had strong evidence for PCSK9 inhibitors from the FOURIER and ODYSSEY OUTCOMES trials. But those trials enrolled patients who had already had a heart attack or stroke. They were secondary prevention trials. The skeptics could argue, and many did, that PCSK9 inhibitors were only proven to help people who were already in the highest-risk category after a major event.
VESALIUS-CV eliminates that argument. This is the first randomized controlled trial to show that a PCSK9 inhibitor, or any non-statin lipid-lowering therapy for that matter, prevents a first cardiovascular event in patients already on high-intensity lipid-lowering therapy. It moves the evidence base into primary prevention territory.
As one of the editorial commentators put it in NEJM, the numerically lower death rate in the evolocumab group, while not statistically significant due to the hierarchical testing structure, almost certainly represents a real biological signal. Longer follow-up would likely reveal a mortality benefit too.
The Bigger Picture: Remaining Questions
While VESALIUS-CV is a major step forward, several questions remain:
-
Cost and access: Repatha is an expensive medication, and its cost-effectiveness in primary prevention, where the absolute event rates are lower than in secondary prevention, will need careful evaluation. The recent approval of biosimilar versions of Repatha may help bring costs down.
-
Who benefits most? The trial enrolled patients with atherosclerosis or diabetes. Whether the benefits extend to other high-risk primary prevention populations (for example, patients with very high LDL-C due to genetic conditions like familial hypercholesterolemia who have not yet developed atherosclerosis) remains to be fully explored.
-
Long-term outcomes: While 4.6 years of follow-up is substantial, even longer-term data will be valuable to confirm the durability of the benefits and the continued safety of very low LDL-C levels.
-
Guideline evolution: As medical societies digest the VESALIUS-CV data, recommendations for PCSK9 inhibitor use in primary prevention are likely to evolve, potentially moving from "may be reasonable" to a stronger endorsement.
A Note on Limitations
No trial is perfect. The VESALIUS-CV population was predominantly white, so we need caution before extrapolating broadly across all racial and ethnic groups. About 8% of patients were not on any lipid-lowering therapy at baseline, which is a quirk for a trial targeting patients already on high-intensity therapy. And the absolute risk reduction, while clinically meaningful, reflects a population at intermediate rather than the highest levels of cardiovascular risk.
None of that changes the overall conclusion. The signal is real, it is consistent, and it is statistically robust.
Repatha Bottom Line
The VESALIUS-CV trial represents a turning point in cardiovascular prevention. For the first time, a dedicated outcomes trial has shown that a PCSK9 inhibitor can prevent first heart attacks and strokes in high-risk patients who have never experienced one. The benefits were consistent across subgroups, including patients with no known atherosclerosis, and the safety profile was reassuring over nearly five years.
For millions of people living with diabetes or early-stage atherosclerosis who are at elevated cardiovascular risk, these findings open the door to a more proactive approach to prevention, one that does not wait for a catastrophic event before deploying the most powerful cholesterol-lowering tools available. As guidelines catch up with the evidence, Repatha's role in primary prevention is poised to grow significantly.
VESALIUS-CV is one of the most important cardiovascular prevention trials in years. It extends the proven benefit of PCSK9 inhibition to patients who have never had a heart attack or stroke. It reinforces everything we know about cumulative LDL exposure and the value of aggressive, early lipid lowering. And it should prompt every clinician to ask whether their high-risk patients are truly at LDL goal.
If you have risk factors, if you have been told you have atherosclerosis, or if you have been struggling to get your LDL under control, this is exactly the kind of evidence-based conversation I have every day in clinical practice.
References:
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















