

When To Start Treating Cholesterol? The Sooner The More Benefit You Get!
May 28, 2026
The Cholesterol Paradox: Why Lower-Risk Patients Get the Biggest Benefit From Treatment
For years the standard advice has gone something like this: wait until your risk is high enough, then we will treat your cholesterol. The logic feels intuitive. Sicker patients have more to gain, so we save the medication for them.
A new systematic review and meta-analysis published in the American Journal of Preventive Cardiology in 2026 turns that intuition on its head, and it lines up beautifully with everything we know about how atherosclerosis actually develops over a lifetime.
The headline finding is striking. When you measure the relative benefit of lowering LDL cholesterol, the people who gain the most per unit of lowering are not the highest-risk patients. They are the lower-risk ones. The patients we have historically been the slowest to treat.
Let me walk you through what this study found and why it matters for the way we think about prevention.
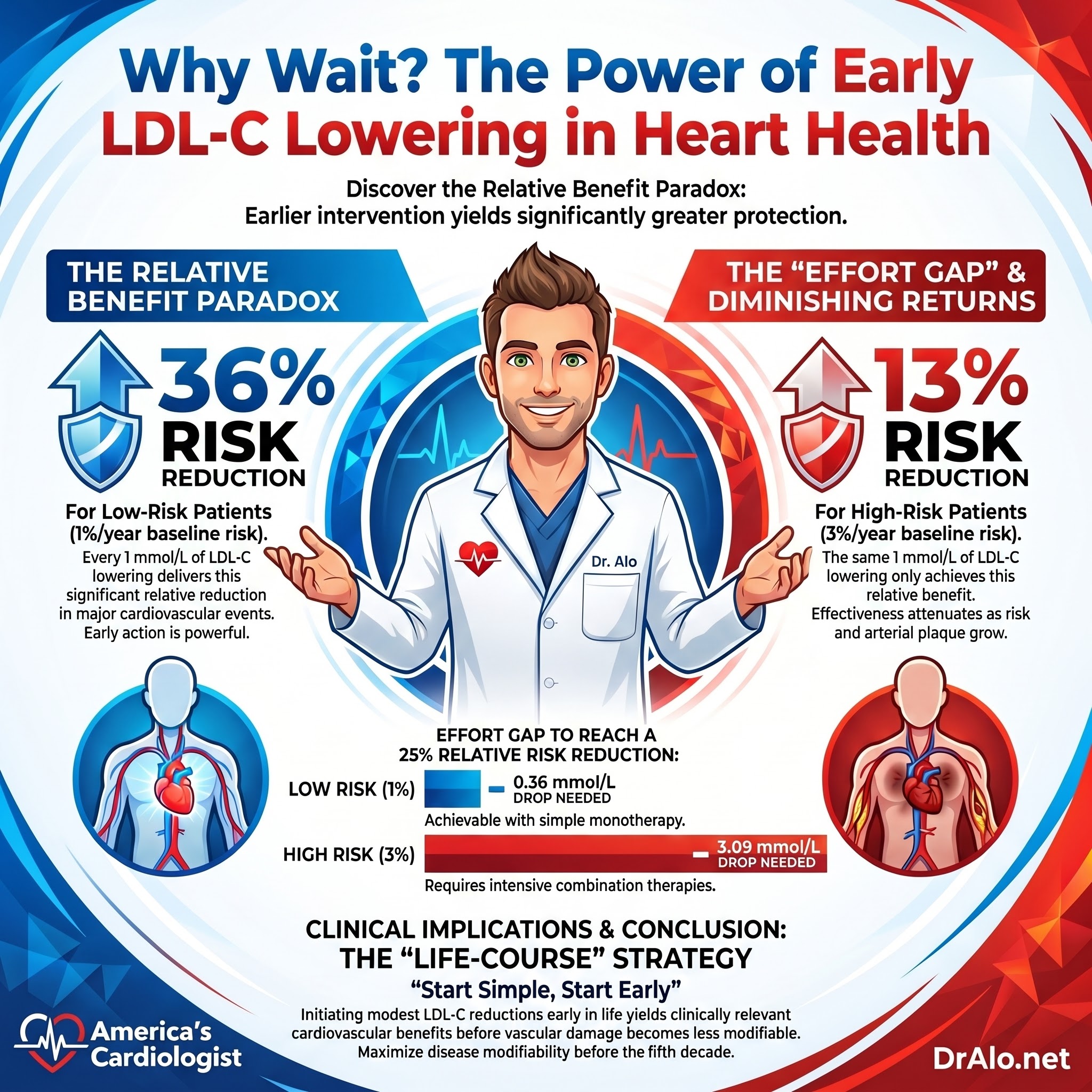
Infographic Summary:
What the Study Actually Looked At
The research team, led by Irene Karungi and senior author Kausik Ray (who wrote a forward for my cholesterol and lipidology textbook and past president of the European Atherosclerotic Society) at Imperial College London, pooled data from 17 completed randomized controlled trials. That is 105,879 participants and 6076 hard cardiovascular events, with a median follow-up of 4.4 years and a mean age of 63 years.
These were not secondary prevention trials. Every trial enrolled people with no or low prevalence of established atherosclerotic cardiovascular disease, meaning primary prevention. Twelve trials tested statins and five tested non-statins, including ezetimibe, bempedoic acid, and a PCSK9 inhibitor. The LDL reductions across trials ranged from 0.38 to 1.95 mmol/L, which is about 15 to 75 mg/dL.
The clever part was the analysis. They asked a simple question: does the relative risk reduction per 1 mmol/L (38.6 mg/dL) of LDL lowering change depending on how high-risk the population is? They used each trial's placebo event rate as a stand-in for baseline risk, then ran a meta-regression.
Finding One: Lower Risk, Bigger Relative Benefit
Here is the number that should make you sit up. For every 1 mmol/L (roughly 39 mg/dL) reduction in LDL, the relative risk reduction was about 36 percent in populations with a low event rate of 1 percent per year. In populations with an event rate of 3 percent per year, that same 1 mmol/L reduction delivered only about 13 percent.
That is nearly a threefold difference in relative benefit, and it favors the lower-risk group. The statistical signal was rock solid, with a p-value below 0.0001.
In plain terms: the earlier and the lower-risk you are when you start lowering your atherogenic particle burden, the more mileage you get out of each unit of lowering.
Finding Two: The Higher Your Risk, the Harder You Have to Push
The flip side is just as important. The study estimated how much LDL lowering you would need to hit a 25 percent relative risk reduction, the benchmark figure from the classic Cholesterol Treatment Trialists analysis.
At a low event rate of 1 percent per year, you only needed to drop LDL by about 0.36 mmol/L (around 14 mg/dL) to reach that 25 percent benefit. At an event rate of 2 percent per year, you needed 1.72 mmol/L (about 67 mg/dL). At 3 percent per year, you needed a massive 3.09 mmol/L (about 119 mg/dL).
Read that again. The higher-risk patients needed roughly six to eight times more LDL lowering to achieve the same relative benefit. Those are reductions that are genuinely hard to hit in real-world practice and usually require combination therapy, a statin plus ezetimibe or a PCSK9 inhibitor stacked on top.
Finding Three: The Number Needed to Treat Barely Moves
There is one more piece that reframes the cost-effectiveness conversation. Because relative benefit shrinks as risk climbs, the number needed to treat over 5 years for each 1 mmol/L of LDL lowering stayed remarkably flat across the risk spectrum. It ranged from about 58 to 70, and the difference was not statistically significant (p equals 0.361).
This matters. The traditional argument for waiting is that high-risk patients give you a smaller number needed to treat, so your dollars go further. This analysis suggests that assumption does not hold the way we thought, because the larger relative benefit in lower-risk people offsets their lower absolute risk. Withholding treatment from lower-risk patients on purely economic grounds may not be justified.
Why This Happens: It Comes Down to the Plaque
None of this is magic. The most likely explanation is biological, and it is about the stage of the disease.
Early atherosclerosis is soft, dynamic, and modifiable. Statins started against early lesions can prevent and stabilize them effectively. By the time someone is high-risk, they usually carry a larger and more mature plaque burden. Even high-intensity statins, which pull LDL down to roughly 1.6 to 2.0 mmol/L (about 62 to 77 mg/dL), arrest progression but rarely regress those advanced plaques. To meaningfully regress mature disease, you often need on-treatment LDL levels closer to 0.6 to 0.9 mmol/L (about 23 to 35 mg/dL), the territory of adjunctive PCSK9-targeting therapy.
So the same drop in LDL does more when the artery wall has less accumulated damage to undo. You are working with the disease, not against decades of buildup.
The ApoB Connection
I want to be precise here, because this is where the science gets sharpened. The trials measured LDL cholesterol, but LDL-C is really a proxy for the thing that actually drives the disease: the number of atherogenic particles delivering cholesterol into the artery wall. ApoB counts every one of those particles, which is why I lean on it as the preferred risk metric.
The mechanism in this study is a particle-burden story. Cardiovascular benefit tracks with the magnitude of LDL lowering regardless of which drug pathway you use, exactly as Mendelian randomization predicts. Genetic studies show that lifelong lower LDL yields a 50 to 60 percent reduction in risk per 1 mmol/L, far larger than the benefit from a pill started late in life. The longer you keep the particle count low, the more the benefit compounds. Lowering your ApoB-bearing particle load earlier means fewer particles infiltrating the wall over the decades that matter most.
What This Means for You
The 2026 ACC/AHA Multisociety dyslipidemia guidelines are already moving toward a life-course approach. They now recommend strong consideration of statin therapy in people age 30 and older who have persistent LDL-C above 160 mg/dL (4.2 mmol/L), a strong family history of premature heart disease, or an elevated 30-year risk.
This study dovetails with that direction. If we start simple, low-cost, generic statin therapy in primary prevention earlier, we should expect a relative risk reduction closer to one-third rather than the 25 percent average, because we are treating the modifiable, lower-risk phase of the disease.
The practical takeaway is the same one I have been making for years. Do not wait for a calculator to tell you that you are finally sick enough to treat. If your ApoB and LDL are elevated, your family history is concerning, or your long-term risk is high even when your short-term number looks tame, that is precisely when treatment pays off the most.
Risk Treatment Bottom Line
Lowering LDL earlier, in lower-risk people, delivers a larger relative benefit per unit of lowering than waiting until risk is high. Higher-risk patients are not getting a better deal by waiting. They are getting a harder problem that demands far more aggressive lowering to reach the same relative benefit. The biology of plaque, the genetics of lifelong exposure, and now this trial-level evidence all point in one direction: start sooner, keep the particle count low, and let time do the rest.
References
Karungi I, Stevens CAT, Brandts J, Ray KK. Cardiovascular event rate modifies response to pharmacologic LDL-C lowering in primary prevention: implications of a systematic review and meta-analysis for clinical practice. American Journal of Preventive Cardiology. 2026. https://doi.org/10.1016/j.ajpc.2026.101655
Cholesterol Treatment Trialists' Collaboration. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. The Lancet. 2012;380(9841):581 to 590. https://doi.org/10.1016/S0140-6736(12)60367-5
Ference BA, Braunwald E, Catapano AL. The LDL cumulative exposure hypothesis: evidence and practical applications. Nature Reviews Cardiology. 2024;21(10):701 to 716. https://doi.org/10.1038/s41569-024-01017-x
Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. European Heart Journal. 2017;38(32):2459 to 2472. https://doi.org/10.1093/eurheartj/ehx144
Writing Committee Members, Blumenthal RS, Morris PB, et al. 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidemia. Circulation. 2026;153(17):e1154 to e1276.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















