

Do Statins Reduce All Cause Mortality? New Research Says Yes!
May 29, 2026
Do Statins Help You Live Longer? What the Mortality Data Actually Shows
There is a version of the statin debate that lives entirely online, where the drugs are framed as a way to lower a number on a lab report without changing whether you actually live or die. It is a clever argument because it sounds sophisticated. Sure, statins lower cholesterol, the reasoning goes, but do they keep you alive, or do they just trade a heart attack for some other cause of death?
I want to answer that question directly, because the data answer it directly. Statins reduce all-cause mortality. Not just heart attacks. Not just strokes. Total deaths from any cause. That conclusion rests on more than three decades of randomized trials and individual patient meta-analyses, and it is one of the most reproducible findings in all of cardiovascular medicine.
Let me show you the evidence and the nuance that goes with it.
Why All-Cause Mortality Is the Honest Endpoint
In clinical research, all-cause mortality is the hardest endpoint we have. You are either alive or you are not. There is no adjudication committee, no room for misclassification, no way to massage the definition.
That matters because of a specific objection you will hear: that a drug could prevent heart attacks while quietly increasing deaths from something else, leaving you no better off. All-cause mortality closes that loophole. If a therapy lowers total deaths, it cannot be hiding the bodies in another column. Statins clear this bar, and clearing it is far harder than simply reducing cardiovascular events.
Infographic Summary:
The Trial That Started It: 4S
The story begins in 1994 with the Scandinavian Simvastatin Survival Study, known as 4S. It enrolled 4444 patients who already had coronary disease and elevated cholesterol, and randomized them to simvastatin or placebo for a median of 5.4 years.
The result was a 30 percent relative reduction in all-cause mortality, with a relative risk of 0.70 (95 percent CI 0.58 to 0.85). In absolute terms, 8.5 percent of the simvastatin group died compared to 11.5 percent on placebo. That is roughly one life saved for every 33 high-risk patients treated. 4S turned statins from cholesterol curiosities into proven life-extending therapy overnight.
The Confirmation: HPS, WOSCOPS, and LIPID
One trial is a signal. A pattern across trials is the truth.
The Heart Protection Study in 2002 was one of the largest statin trials ever run, enrolling 20,536 patients with vascular disease or diabetes. Simvastatin 40 mg cut all-cause mortality by 13 percent, with a relative risk of 0.87 (95 percent CI 0.81 to 0.94). The benefit held up across subgroups that people love to claim are exceptions: older adults, women, people with diabetes, and importantly, people who started with lower baseline cholesterol.
The West of Scotland Coronary Prevention Study in 1995 mattered because it was primary prevention. These were 6595 men with high cholesterol but no prior heart disease. Pravastatin reduced coronary mortality by 32 percent. This was early proof that you do not have to wait for a heart attack to benefit.
The LIPID trial in 1998 added 9014 patients with coronary disease and showed a 24 percent reduction in coronary mortality with pravastatin, alongside a favorable trend in total mortality.
What the Pooled Data Show
Meta-analyses, especially those using individual patient data, give us the most stable estimates of any treatment effect. Here the consistency is almost monotonous, and in medicine, monotonous is exactly what you want.
The Cholesterol Treatment Trialists Collaboration is the gold standard, built on individual patient data from over 170,000 participants. It has repeatedly shown that statin therapy reduces vascular mortality by roughly 12 percent per 1 mmol/L (about 39 mg/dL) reduction in LDL cholesterol, and that all-cause mortality falls in both primary and secondary prevention.
The United States Preventive Services Task Force commissioned a review in 2022 focused only on primary prevention. Pooling 18 trials and 85,186 participants, statins reduced all-cause mortality with a relative risk of 0.92 (95 percent CI 0.87 to 0.98). The heterogeneity was zero. An I squared of 0 percent means the trials were not arguing with each other, they were agreeing. The number needed to treat was about 286 over one to six years.
Their earlier 2016 review of 15 trials and 71,344 participants found an even larger effect, a relative risk of 0.86 (95 percent CI 0.80 to 0.93) for all-cause mortality, along with a significant reduction in cardiovascular death specifically.
Byrne and colleagues, writing in JAMA Internal Medicine in 2022 from a more skeptical posture, still found a 9 percent relative reduction in all-cause mortality across 21 trials (95 percent CI 5 to 14 percent). Their real contribution was insisting that we communicate absolute risk to patients, which I agree with completely.
And when you step outside the trials into the real world, the picture holds. Nowak and colleagues pooled 54 propensity score matched observational studies in 2022 and found a hazard ratio of 0.72 (95 percent CI 0.66 to 0.76) for all-cause mortality, with a similar benefit in people with and without established disease.
Statin All Cause Mortality Forest Plot
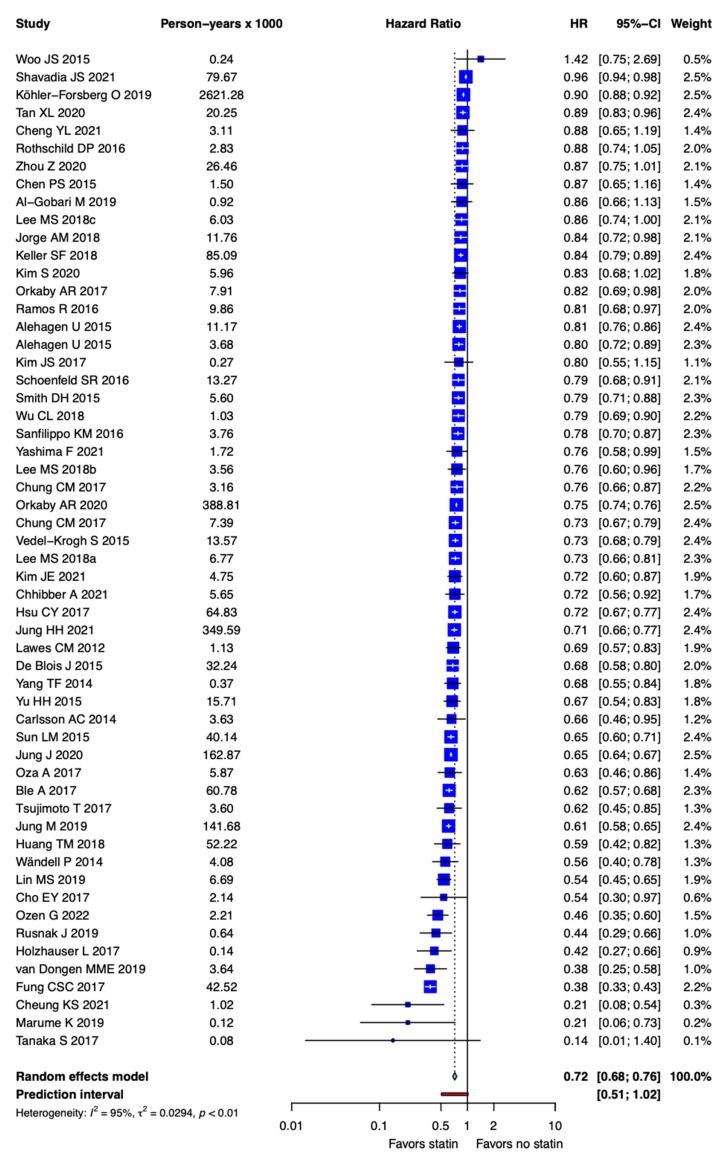
Nearly every study ever done on statins shows a reduction in all cause mortality.
What About Patients Over 75?
This is the question I get constantly, because the original trials underenrolled the elderly. An observational study of United States veterans aged 75 and older, none with prior atherosclerotic disease, found statin use associated with a hazard ratio of 0.75 (95 percent CI 0.74 to 0.76) for all-cause mortality over a mean follow-up of 6.8 years.
It is observational, so I hold it more loosely than a randomized trial. But the size, the tight confidence interval, and the consistency across sensitivity analyses are reassuring. Age alone is not a reason to stop a statin.
Primary Versus Secondary Prevention: Read the Absolute Numbers
Here is the nuance that honest clinicians do not skip. The relative risk reduction from statins is broadly similar whether you have had an event or not, somewhere in the range of 8 to 30 percent for mortality. What changes is the absolute benefit, because absolute benefit scales with your baseline risk.
In secondary prevention, where baseline mortality is high, the absolute reduction is large, often 1 to 3 percent over 5 years. In primary prevention, the same relative reduction sits on top of a lower baseline risk, so the absolute number looks smaller, around 0.35 to 0.8 percent.
That smaller number is not a reason to dismiss treatment. It is a reason to personalize it. A 55 year old man with a 15 percent ten year risk gets meaningful benefit. A 40 year old woman with a 3 percent risk has a different calculation. This is what shared decision making actually means, and it requires showing patients both the relative and the absolute numbers instead of hiding behind whichever one makes the point you want.
The Particle Story Behind the Survival Curve
Step back and ask why any of this works, and you arrive at the same place I always land. Cardiovascular disease is driven by the lifetime burden of atherogenic, ApoB containing particles depositing cholesterol into the artery wall. LDL cholesterol is the number we measure, but ApoB counts the actual particles doing the damage.
Statins reduce that particle burden, and the survival benefit follows the magnitude of LDL lowering rather than any mystical property of the drug class. That is exactly what you would predict if particles cause the disease, and it is why the mortality benefit shows up across different statins, different countries, and three decades of investigators. The drug is not the point. Lowering the particle load is the point, and statins do it cheaply, safely, and effectively.
Addressing the Usual Objections
On the claim that the benefit is too small to matter: in primary prevention the absolute mortality reduction is modest, but statins also prevent nonfatal heart attacks, strokes, and procedures that mortality counts alone do not capture. Apply even a small absolute benefit across tens of millions of people and you are talking about a very large number of lives.
On the claim that statins do more harm than good: serious harm is rare. Rhabdomyolysis runs around 1 in 10,000 patient years. The much discussed new onset diabetes signal is real but small, roughly 1 extra case per 255 people treated for 4 years, and it is concentrated in those already heading toward diabetes. Much of the muscle symptom burden attributed to statins does not survive blinded nocebo controlled testing.
On the claim that industry funded everything: the publicly funded USPSTF reviews and the academically led CTT analyses, using raw individual patient data, reproduce the same answer. Bias does not replicate that cleanly across that many independent hands.
Infographic Summary:
Why Statins Stand Alone: The Non-Statin Comparison
Here is a point the statin critics never seem to make, even though it cuts against their own argument. If lowering cholesterol were just a number game with no real payoff, you would expect every cholesterol drug to look the same. They do not. Statins are the only lipid-lowering class with a clearly established all-cause mortality benefit across multiple large trials and meta-analyses. The other agents tell an instructive story about why.
The strongest non-statin signal comes from the PCSK9 inhibitors, and specifically alirocumab. In ODYSSEY OUTCOMES, which enrolled 18,924 patients after an acute coronary syndrome and followed them for a median of 2.8 years, alirocumab reduced all-cause death by 15 percent, with a hazard ratio of 0.85 (95 percent CI 0.73 to 0.98). That was a nominal p-value of 0.03, but because of the trial's hierarchical testing rules it did not formally clear the bar for statistical significance. A Bayesian re-analysis put the probability of a true mortality benefit at 98.4 percent, and in the subgroup followed for 3 years or more the reduction grew to a hazard ratio of 0.78 (95 percent CI 0.65 to 0.94). Alirocumab even showed a trend toward fewer noncardiovascular deaths, hazard ratio 0.77 (95 percent CI 0.59 to 1.01).
Evolocumab, the other major PCSK9 inhibitor, did not reduce all-cause or cardiovascular mortality in FOURIER. The most likely reason is mundane: a median follow-up of only 2.2 years is simply too short to let a mortality curve separate. A Cochrane review and a later pooled analysis both confirmed the split, with alirocumab showing a mortality reduction and evolocumab not reaching significance.
That timing point is the key to reading all of this correctly. Mortality is the hardest endpoint to move, and moving it usually requires high baseline risk and years of separation between the curves. The PCSK9 and ezetimibe add-on trials were short by design, so their event reductions are real even where the mortality signal has not yet matured.
Ezetimibe is the clean example. A Cochrane review of 26 trials and 23,499 patients found little or no effect on all-cause mortality, with a relative risk of 0.98 (95 percent CI 0.91 to 1.05), and no effect on cardiovascular mortality. It does reduce nonfatal heart attacks and strokes, which is exactly what you would expect from modest additional LDL lowering over a short horizon.
Fibrates are where the picture turns. Cochrane reviews in both primary and secondary prevention show no all-cause mortality benefit, with relative risks sitting right at 1.0. The pre-statin-era VA-HIT trial did show a 41 percent mortality reduction with gemfibrozil, but that has never been replicated in the statin era, and a systematic review by Studer and colleagues actually linked fibrates to an increase in noncardiovascular death.
Niacin is worse. A Cochrane review of 23 trials and 39,195 patients found no mortality benefit, relative risk 1.05, and when the analysis was limited to the two largest, highest-quality trials, AIM-HIGH and HPS2-THRIVE, the signal pointed toward harm, relative risk 1.10 (95 percent CI 1.00 to 1.20), along with a trend toward more noncardiovascular death. This is one reason niacin has largely fallen out of favor.
Icosapent ethyl sits in its own category, because it is not really an LDL drug. In REDUCE-IT, 4 grams a day cut cardiovascular death by 20 percent, hazard ratio 0.80 (95 percent CI 0.66 to 0.98), though overall all-cause mortality was not significantly reduced. In the United States subgroup of 3146 patients, all-cause mortality did fall significantly, hazard ratio 0.70 (95 percent CI 0.55 to 0.90), and in patients with a prior heart attack it trended in the same direction.
Put it together and the lesson reinforces everything above. No non-statin lipid-lowering agent has yet demonstrated a reduction in noncardiovascular mortality, and statins remain the only class with a clear, repeatedly confirmed all-cause mortality benefit. That is not a reason to abandon the add-on therapies, which lower ApoB and prevent events, especially in higher-risk patients who need more lowering than a statin alone can deliver. It is a reason to start with the agent that has the deepest survival evidence, and to give the others the long, high-risk follow-up they need before we judge their effect on mortality.
The Bottom Line
The question of whether statins reduce all-cause mortality is settled. They do, robustly, in the highest quality evidence we have, and they remain the only lipid-lowering class that has clearly cleared that bar. The benefit is largest in secondary prevention, real but smaller in absolute terms in primary prevention, and consistent across age, sex, and baseline cholesterol.
The honest work now is not relitigating whether statins save lives. It is identifying who benefits most, lowering the ApoB particle burden early enough to matter, and communicating both the relative and absolute numbers clearly enough that patients can make a real decision. That is a conversation worth having, and it should be grounded in the data rather than the noise.
References
Chou R, Cantor A, Dana T, et al. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2022;328(8):754 to 771. https://doi.org/10.1001/jama.2022.12138
Chou R, Dana T, Blazina I, Daeges M, Jeanne TL. Statins for Prevention of Cardiovascular Disease in Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2016;316(19):2008 to 2024. https://doi.org/10.1001/jama.2015.15629
Byrne P, Demasi M, Jones M, et al. Evaluating the Association Between Low-Density Lipoprotein Cholesterol Reduction and Relative and Absolute Effects of Statin Treatment: A Systematic Review and Meta-analysis. JAMA Internal Medicine. 2022;182(5):474 to 481. https://doi.org/10.1001/jamainternmed.2022.0134
Collins R, Reith C, Emberson J, et al. Interpretation of the Evidence for the Efficacy and Safety of Statin Therapy. Lancet. 2016;388(10059):2532 to 2561. https://doi.org/10.1016/S0140-6736(16)31357-5
Nowak MM, Niemczyk M, Florczyk M, Kurzyna M, Paczek L. Effect of Statins on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies. Journal of Clinical Medicine. 2022;11(19):5643. https://doi.org/10.3390/jcm11195643
Orkaby AR, Driver JA, Ho YL, et al. Association of Statin Use With All-Cause and Cardiovascular Mortality in US Veterans 75 Years and Older. JAMA. 2020;324(1):68 to 78. https://doi.org/10.1001/jama.2020.7848
Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease (4S). Lancet. 1994;344(8934):1383 to 1389.
Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360(9326):7 to 22.
Steg PG, Szarek M, Bhatt DL, et al. Effect of Alirocumab on Mortality After Acute Coronary Syndromes. Circulation. 2019;140(2):103 to 112. https://pubmed.ncbi.nlm.nih.gov/31117810
Labos C, Brophy JM, Sniderman A, Thanassoulis G. Mortality Benefit of Alirocumab: A Bayesian Perspective. Journal of the American Heart Association. 2019;8(20):e013170. https://pubmed.ncbi.nlm.nih.gov/31599200
AlTurki A, Marafi M, Dawas A, et al. Meta-Analysis of Randomized Controlled Trials Assessing the Impact of Proprotein Convertase Subtilisin/Kexin Type 9 Antibodies on Mortality and Cardiovascular Outcomes. The American Journal of Cardiology. 2019;124(12):1869 to 1875. https://pubmed.ncbi.nlm.nih.gov/31679643
Schmidt AF, Carter JL, Pearce LS, et al. PCSK9 Monoclonal Antibodies for the Primary and Secondary Prevention of Cardiovascular Disease. The Cochrane Database of Systematic Reviews. 2020;10:CD011748. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD011748.pub3/full
Imran TF, Khan AA, Has P, et al. Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors and Small Interfering RNA Therapy for Cardiovascular Risk Reduction: A Systematic Review and Meta-Analysis. PLoS One. 2023;18(12):e0295359. https://pubmed.ncbi.nlm.nih.gov/38055686
Zhan S, Tang M, Liu F, et al. Ezetimibe for the Prevention of Cardiovascular Disease and All-Cause Mortality Events. The Cochrane Database of Systematic Reviews. 2018;11:CD012502. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD012502.pub2/full
Khan SU, Yedlapati SH, Lone AN, et al. PCSK9 Inhibitors and Ezetimibe With or Without Statin Therapy for Cardiovascular Risk Reduction: A Systematic Review and Network Meta-Analysis. BMJ. 2022;377:e069116. https://pubmed.ncbi.nlm.nih.gov/35508321
Jakob T, Nordmann AJ, Schandelmaier S, Ferreira-Gonzalez I, Briel M. Fibrates for Primary Prevention of Cardiovascular Disease Events. The Cochrane Database of Systematic Reviews. 2016;11:CD009753. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009753.pub2/full
Wang D, Liu B, Tao W, Hao Z, Liu M. Fibrates for Secondary Prevention of Cardiovascular Disease and Stroke. The Cochrane Database of Systematic Reviews. 2015;(10):CD009580. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009580.pub2/full
Virani SS, Morris PB, Agarwala A, et al. 2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients With Persistent Hypertriglyceridemia. Journal of the American College of Cardiology. 2021;78(9):960 to 993. https://linkinghub.elsevier.com/retrieve/pii/S0735-1097(21)05323-7
Studer M, Briel M, Leimenstoll B, Glass TR, Bucher HC. Effect of Different Antilipidemic Agents and Diets on Mortality: A Systematic Review. Archives of Internal Medicine. 2005;165(7):725 to 730. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/archinte.165.7.725
Schandelmaier S, Briel M, Saccilotto R, et al. Niacin for Primary and Secondary Prevention of Cardiovascular Events. The Cochrane Database of Systematic Reviews. 2017;6:CD009744. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009744.pub2/full
Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. The New England Journal of Medicine. 2019;380(1):11 to 22. https://www.nejm.org/doi/full/10.1056/NEJMoa1812792
Bhatt DL, Miller M, Brinton EA, et al. REDUCE-IT USA: Results From the 3146 Patients Randomized in the United States. Circulation. 2020;141(5):367 to 375. https://pubmed.ncbi.nlm.nih.gov/31707829
Gaba P, Bhatt DL, Steg PG, et al. Prevention of Cardiovascular Events and Mortality With Icosapent Ethyl in Patients With Prior Myocardial Infarction. Journal of the American College of Cardiology. 2022;79(17):1660 to 1671. https://pubmed.ncbi.nlm.nih.gov/35483753
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















