

One Shot To End Heart Disease? Gene Editing CRISPR Technology
May 27, 2026
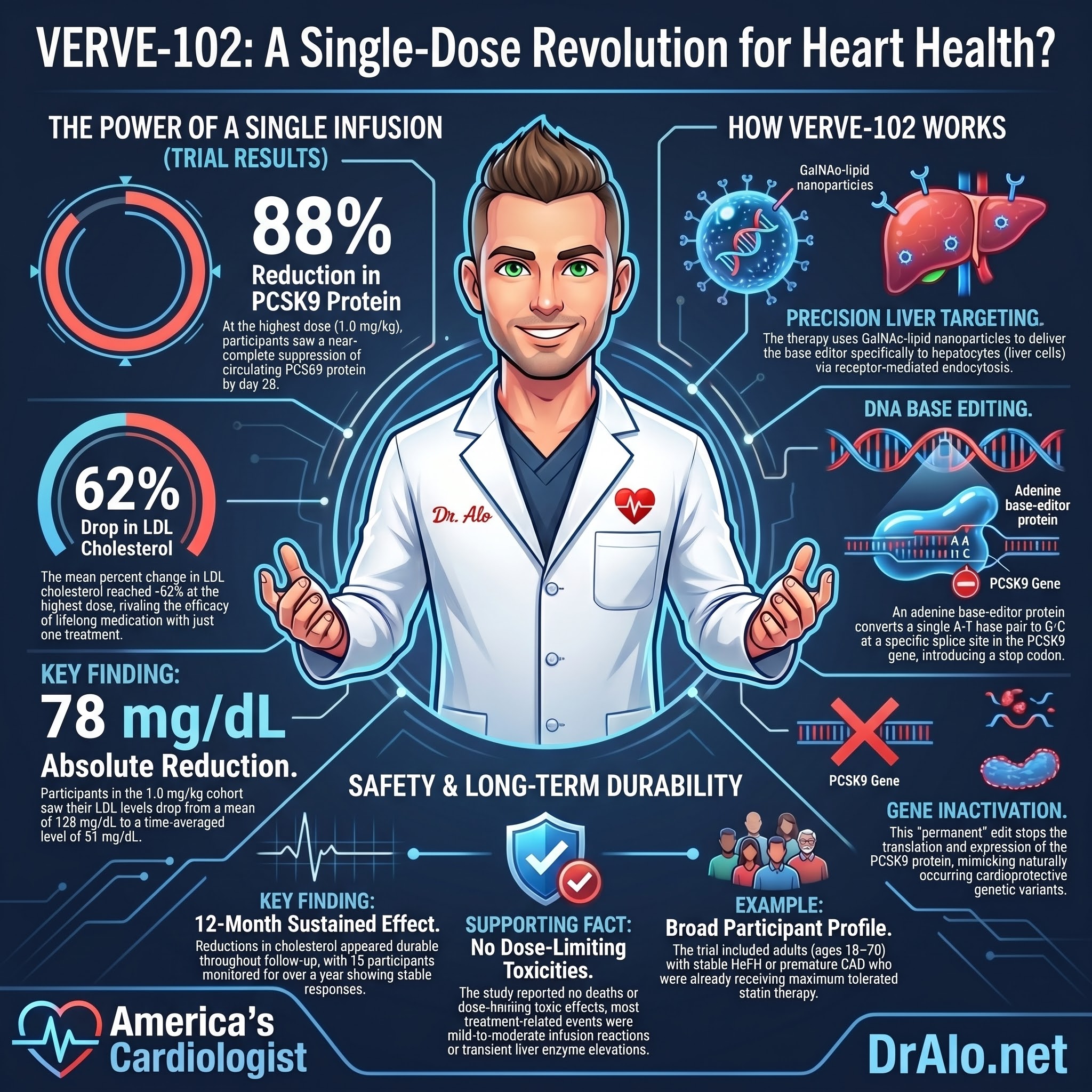
One Shot to Lower Your Cholesterol for Life: The VERVE-102 Gene Editing Trial
What if you could take a single IV infusion and permanently lower your LDL cholesterol by 62% for the rest of your life? No pills every morning. No injections every two weeks. No worrying about adherence, side effects, or insurance prior authorizations. Just one treatment that edits a single gene in your liver and, as far as we can tell, keeps working indefinitely.
That is not science fiction. On May 25, 2026, the New England Journal of Medicine published the Phase 1 results of the Heart-2 trial, the first human study of VERVE-102, an in vivo base-editing therapy targeting the PCSK9 gene. The results are among the most exciting I have seen in cardiovascular medicine in a long time.
Let me walk you through exactly what happened, why the science behind it is so compelling, and what it means for the future of cholesterol treatment.
Infographic Summary:
The PCSK9 Story: Why This Gene Is the Perfect Target
To understand why this trial matters, you need to understand one of the most important discoveries in cardiovascular genetics of the past 20 years.
PCSK9, short for proprotein convertase subtilisin/kexin type 9, is a protein your liver makes that degrades LDL receptors. LDL receptors are the cellular machinery that pulls ApoB-containing particles, including LDL, out of your bloodstream and into the liver for disposal. When PCSK9 destroys those receptors, fewer particles are cleared, and LDL cholesterol rises. When PCSK9 is blocked or inactivated, more LDL receptors survive on the liver surface, and LDL cholesterol falls dramatically.
Here is the critical discovery: in 2005 and 2006, researchers studying the genetics of populations in Texas and Dallas found people who were born with natural loss-of-function mutations in their PCSK9 gene. These individuals had lifelong low LDL cholesterol, with no apparent adverse effects on health. And compared to people with normal PCSK9 function, they had an 88% lower lifetime risk of coronary artery disease.
That number deserves repetition. Eighty-eight percent lower lifetime risk from a single gene variant that keeps LDL low from birth.
Compare that to statins. Lowering LDL by the same amount with a statin over five years reduces the risk of major vascular events by approximately 22%. The difference is not because statins are weak drugs. The difference is time. The people with natural PCSK9 mutations had lower LDL from birth, not just from age 50 when they started a statin. The cardiovascular benefits of lower LDL accumulate over decades. Cumulative ApoB exposure is what drives plaque. Start lowering it earlier and keep it lower longer, and the protection is dramatically amplified.
This is exactly the biological logic that VERVE-102 is designed to exploit. Instead of inhibiting PCSK9 with a drug you have to keep taking, what if you could permanently inactivate the PCSK9 gene with a single treatment and mimic the biology of those naturally protected individuals?
How VERVE-102 Works: Base Editing Explained
VERVE-102 is a base-editing therapy, a type of gene editing that is more precise than the original CRISPR-Cas9 scissors approach. Rather than cutting both strands of DNA, base editing chemically converts one DNA base to another at a specific location, like a pencil and eraser operating at the molecular level.
VERVE-102 consists of two components packaged inside a lipid nanoparticle delivery vehicle:
The first component is a messenger RNA encoding an adenine base-editor protein. This protein combines a modified CRISPR-Cas9 component (engineered so it nicks only one strand of DNA rather than cutting both) with an adenosine deaminase enzyme that converts adenine (A) to inosine, which the cell reads as guanine (G).
The second component is a guide RNA that directs the base editor to a specific splice site at the beginning of intron 1 of the PCSK9 gene.
Once the base editor reaches its target, it makes a single A to G substitution at that splice site. This one-letter change disrupts the normal splicing of the PCSK9 gene transcript, causing intron 1 to be retained in the messenger RNA and introducing a premature stop codon. The PCSK9 protein can no longer be produced from that gene. The liver cells stop making PCSK9. LDL receptors accumulate on the liver surface. LDL particles, which carry ApoB, are cleared from the blood at a much higher rate. LDL cholesterol falls.
The delivery vehicle deserves special attention. VERVE-102 uses a GalNAc-lipid nanoparticle. GalNAc stands for N-acetylgalactosamine, a sugar molecule that binds with high affinity to the asialoglycoprotein receptor on the surface of liver cells. This targeting ligand essentially acts as a homing beacon, directing the nanoparticle specifically to hepatocytes and minimizing delivery to other organs. The lipid nanoparticle clears from circulation rapidly, with a mean half-life of less than 20 hours, leaving behind edited liver cells but no persistent drug exposure.
The Heart-2 Trial: Who Was Studied and What They Found
The Heart-2 study enrolled adults aged 18 to 70 with heterozygous familial hypercholesterolemia (FH) or premature coronary artery disease, defined as disease onset before age 55 in men or 65 in women. Participants were already on maximum tolerated oral therapy (statin with or without ezetimibe) and still had fasting LDL cholesterol of at least 70 mg/dL. Participants already on injectable PCSK9 inhibitors were excluded.
This is an important patient population. These are the high-risk patients who are most diligently treated and still not at goal. Their ApoB and LDL remain elevated despite best available oral therapy, and guidelines recommend lifelong aggressive treatment. The question VERVE-102 is answering is whether a single gene editing infusion can deliver the LDL reduction that current drugs require ongoing maintenance to achieve.
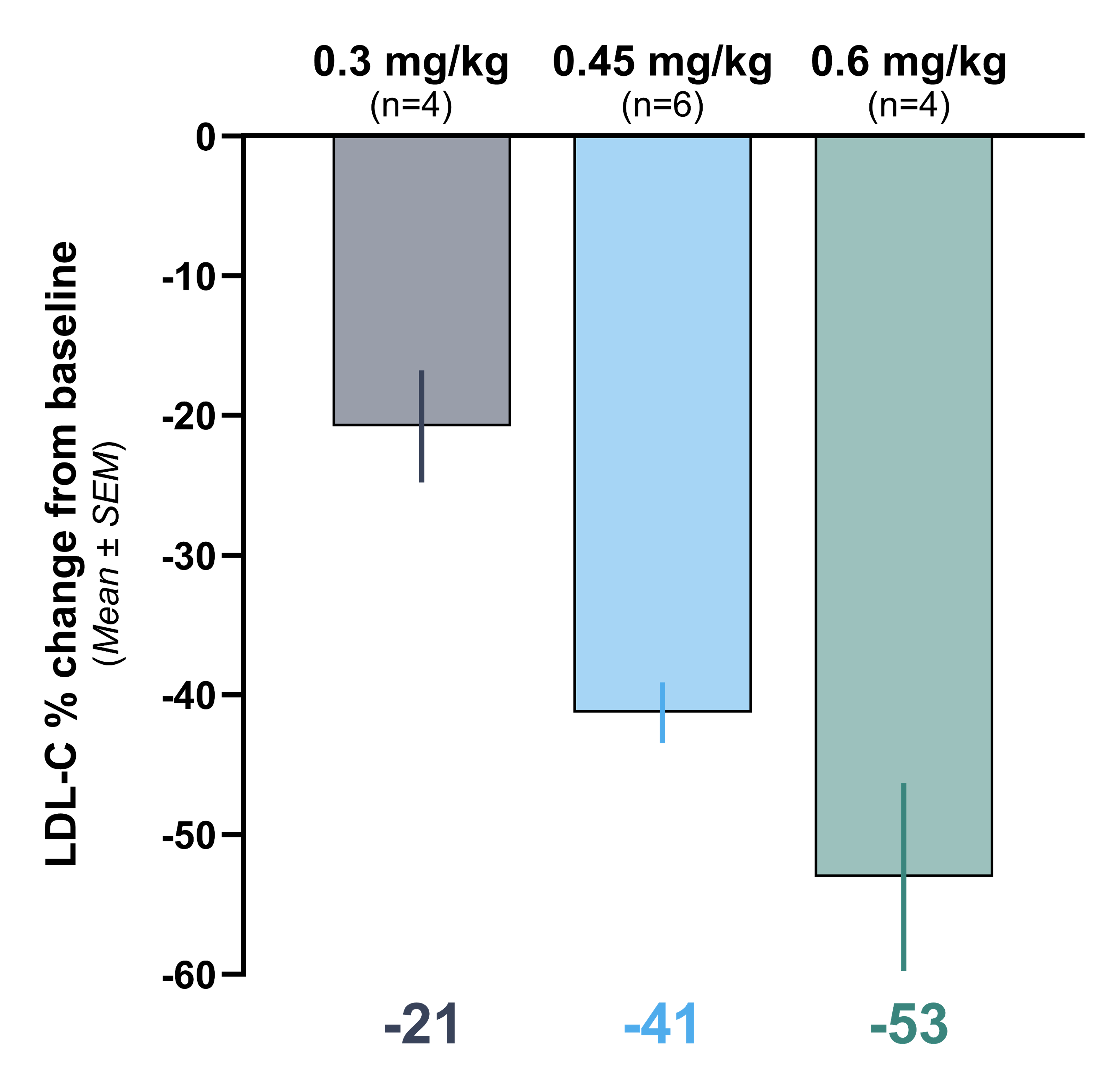
Thirty-five participants received a single IV infusion of VERVE-102 at one of six weight-based doses ranging from 0.3 to 1.0 mg of total RNA per kilogram of body weight. Median follow-up was approximately 9 months, with 15 participants having at least 12 months of follow-up.
The results were dose-dependent and striking.
At the lowest dose (0.3 mg/kg), the mean PCSK9 reduction was 51% and the mean LDL-C reduction was 9%. Results at the lowest dose were variable and modest, likely reflecting insufficient editing at that dose level.
At the highest dose (1.0 mg/kg), the mean PCSK9 reduction was 88%, ranging from 78 to 94% across participants. The mean LDL-C reduction was 62%, ranging from 45 to 79%. The mean absolute LDL-C reduction was 78 mg/dL, bringing average LDL from 128 mg/dL at baseline to a time-averaged level of 51 mg/dL.
To put that in clinical context: that is a response comparable to adding a PCSK9 inhibitor on top of maximized oral therapy, but from a single infusion rather than from injections every two to four weeks indefinitely.
The Durability Signal: Does It Last?
Durability is the central question for any gene editing therapy. If the edit wears off, you are not editing the genome, you are just temporarily suppressing a gene with extra steps.
The Heart-2 trial provides early evidence that VERVE-102's effects are durable. Among participants with follow-up extending to 12 months and beyond, PCSK9 and LDL cholesterol levels at day 28 were consistent with the time-averaged values over the full follow-up period. There was no evidence of waning effect in the data presented.
Why would the edit be durable? Because mature hepatocytes, the liver cells being edited, have an average lifespan of 200 to 300 days. The fact that LDL remained suppressed through the turnover of hepatocyte populations suggests the edited gene is being faithfully copied to daughter cells as the liver regenerates. This is consistent with data from another in vivo gene-editing medicine showing stable inactivation of a hepatic gene through three years of follow-up with no waning of effect.
The authors are appropriately cautious. This is an interim analysis of a Phase 1 study. Follow-up at the highest doses extends only to 12 to 18 months. Longer-term data are needed, and all participants will undergo 15 years of regulatory-mandated follow-up.
But the early signal is what it is. One infusion, at least 12 months of stable LDL reduction, with no apparent waning.
Safety: What Happened and What to Make of It
No dose-limiting toxicities occurred. No deaths occurred. All 35 participants completed the full planned infusion.
Infusion-related reactions occurred in 7 of 35 participants (20%), all grade 1 or 2 in severity. Five resolved without any treatment. Two were treated with acetaminophen or antihistamines. One led to a brief 40-minute pause in the infusion. All resolved completely. Premedication with dexamethasone and antihistamines was administered to all participants on the day of infusion, and dexamethasone was given the day before.
Transient, asymptomatic elevations in alanine aminotransferase (ALT), a liver enzyme, were observed in three participants, reaching a peak of 2.0, 2.2, and 2.4 times the upper limit of normal. All three peaked on day 3 or 4 and returned below two times the upper limit of normal by day 8. These were mild, asymptomatic, and self-resolving.
One serious adverse event occurred: aspiration pneumonitis in a participant who had pre-existing gastroesophageal reflux disease and a hiatal hernia, approximately two weeks after infusion. The site investigator assessed this as unrelated to VERVE-102. The participant was hospitalized briefly and discharged the next day.
Critically, the safety profile of VERVE-102 compared favorably to the previous-generation therapy, VERVE-101, which used a different lipid nanoparticle formulation and was associated with more significant adverse events including decreased platelet counts. The addition of the GalNAc targeting ligand and modifications to the lipid components appear to have substantially improved the safety profile, though the authors note these conclusions are preliminary.
The other major safety consideration for any gene editing therapy is off-target editing, meaning unintended edits at locations in the genome other than the PCSK9 splice site. In pre-clinical experiments with primary human hepatocytes in vitro, editing with VERVE-102 was specific for the intended target site. In mice given a mouse-equivalent version of VERVE-102, there was no transmission of the PCSK9 edit to offspring, consistent with an absence of germline editing. However, long-term off-target safety data in humans will require years of follow-up, and the full 15-year regulatory surveillance period is ongoing.
The Adherence Problem: Why This Matters Beyond the Numbers
I want to take a step back from the clinical data and talk about something that does not get enough attention in cardiology: the real-world treatment gap.
We have excellent drugs for LDL lowering. Statins, ezetimibe, PCSK9 inhibitors, inclisiran. When patients take these drugs consistently, outcomes are dramatically better. The evidence is overwhelming.
The problem is adherence. Across all classes of lipid-lowering therapy, including PCSK9 inhibitors, discontinuation rates range from 30 to 50% within 12 months of starting treatment. Side effects, cost, coverage denials, pill burden, and treatment fatigue all contribute. In the real world, many patients with familial hypercholesterolemia and established cardiovascular disease are not on guideline-directed therapy, and many who start it eventually stop.
This is where VERVE-102 represents something genuinely different. A treatment you cannot forget to take. A treatment that does not require a prior authorization every year. A treatment whose benefit is not diminished by insurance changes, formulary switches, or a period of financial hardship. One infusion with effects that, if the durability data hold, may last decades.
The authors make this point directly in the paper: the 78 mg/dL absolute LDL reduction observed at the highest dose, if maintained over 20 years, is predicted to reduce the risk of atherosclerotic cardiovascular disease by more than 50% for most patients with hypercholesterolemia. That projection comes from the same Mendelian randomization data that tells us lifelong lower LDL has effects far larger than the same reduction achieved over a shorter period.
What Still Needs to Be Answered
Let me be clear about what this trial does not prove.
Heart-2 is a Phase 1 safety study. It was not designed or powered to demonstrate a reduction in cardiovascular events. The 35 participants were carefully selected, premedicated, and observed in an inpatient setting for at least two days. This is not how a real-world treatment rollout works.
The follow-up at the highest doses is short. The 1.0 mg/kg cohort had the fewest participants with long-term data precisely because they were enrolled last. We need to see what PCSK9 and LDL levels look like at three years, five years, and beyond. The edited hepatocytes appear to be passing the edit to their progeny through cell turnover, but we do not yet have human data confirming this over many years.
We do not know the long-term off-target editing risk. The potential for gene editing to introduce unintended changes near oncogenes or tumor suppressor genes, theoretically increasing cancer risk, is a legitimate concern that requires a decade or more of follow-up to meaningfully evaluate. No such signal has emerged in the related ATTR-CM gene editing trials or in the broader gene editing literature, but the surveillance must continue.
The participant population in Heart-2 was 86% White, reflecting the geographic footprint of the trial sites in Australia, Canada, New Zealand, and the United Kingdom. Broader population diversity will be essential in subsequent trials, both because FH variants differ across ancestral populations and because the asialoglycoprotein receptor expression that VERVE-102 relies on for hepatocyte targeting needs to be validated across diverse populations.
Finally, the question of cost, access, and payer coverage has not been addressed and will ultimately determine how many patients can actually benefit from this technology.
The Bottom Line
VERVE-102 is among the most consequential cholesterol data published in years. A single infusion permanently editing the PCSK9 gene in the liver, achieving 88% PCSK9 suppression and 62% LDL reduction, with a favorable early safety profile and durability extending to at least 12 to 18 months, is a genuinely new therapeutic paradigm.
The story of PCSK9 has always been about what happens when LDL stays low for an entire lifetime. The people born with natural PCSK9 loss-of-function variants do not just have lower LDL. They have 88% less coronary artery disease. VERVE-102 is an attempt to give that protection to patients who were not born with it.
We are still in Phase 1. Long-term outcomes trials will be needed before this reaches clinical practice. But the science is sound, the early data are compelling, and the therapeutic logic is backed by twenty years of genetic evidence.
This is the direction cardiovascular medicine is heading. And as your cardiologist, I want you to know it is coming.
References
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















