

Nature CT: Zero CAC Score? You May Still Have Dangerous Artery Plaque
May 25, 2026
Zero CAC Score? What a New Study Reveals About Silent Plaque Progression
Young, metabolically healthy, zero calcium score? Never head a heart attack before? No risk factors? You think you must be fine, right? Not so fast!
Most people assume that if they feel fine, their heart is fine. No chest pain, no shortness of breath, no heart attack, no problem. And if their doctor has never put them on a cholesterol medication, they figure they must not need one.
A brand new study published in the Journal of Cardiovascular Computed Tomography challenges that assumption in a serious way. It followed over 200 adults who had none of the typical warning signs we use to justify early intervention. And what it found should change how you think about preventive cardiology.
Let me break it down for you.
What Was This Study, and Why Does It Matter?
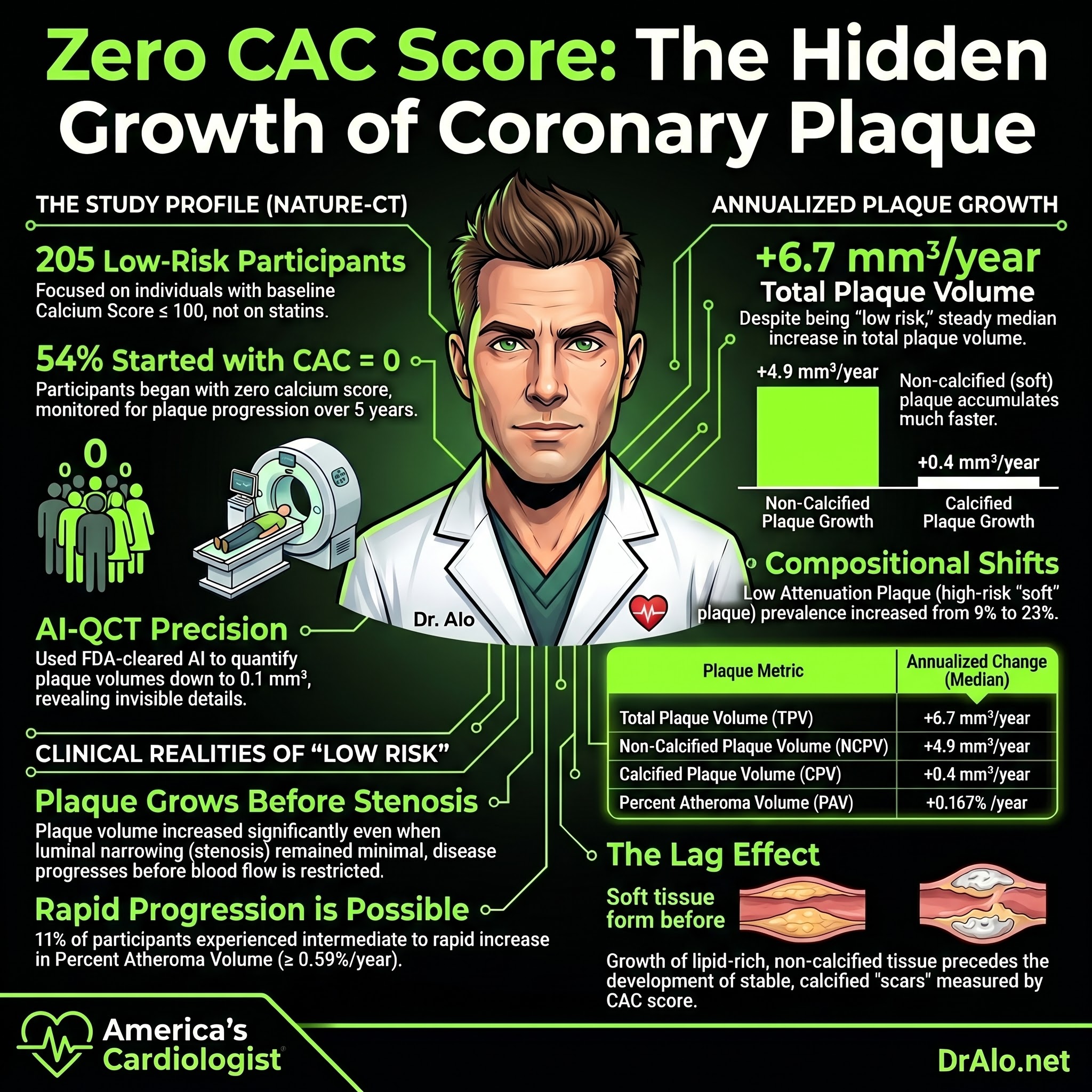
The NATURE-CT study (which stands for NATURal History of Coronary PlaquE on Cardiac Computed Tomography) was a multicenter retrospective study out of two cardiovascular imaging centers in Los Angeles. The researchers identified 205 adults who had undergone at least two coronary CT angiograms (CCTA) at least two years apart.
Here is what made this cohort special. These were not sick people. These were not high-risk patients. The inclusion criteria were deliberately restrictive to give us a clean look at what happens to arteries that are largely left alone.
To be included, participants had to have:
A coronary artery calcium (CAC) score of 100 or less at baseline. No prior heart attack, stroke, or other major cardiovascular event. No use of statins, PCSK9 inhibitors, or any other lipid-lowering medication between scans. No diabetes. No familial hypercholesterolemia. No chronic kidney disease.
The average age was about 55 years old. Most were white men. About a quarter had hypertension. About 28 percent had untreated dyslipidemia. The average LDL was 111 mg/dL, which most doctors would look at and say "that's fine, come back in a year."
They were followed for a median of nearly five years between scans.
And the results were sobering.
Infographic Summary:

What Happened to These "Healthy" Arteries Over Five Years?
The researchers used an FDA-cleared artificial intelligence platform called Cleerly to quantify plaque volumes on each scan. This is not the same as a simple CAC score. AI-assisted quantitative CT can detect and measure non-calcified plaque, calcified plaque, and a dangerous subtype called low attenuation plaque, which corresponds to lipid-rich, vulnerable lesions.
Here is what they found after five years of no treatment and no cardiac events.
Total plaque volume nearly doubled, going from a median of 30.3 mm3 at baseline to 59.2 mm3 at follow-up. That is an annualized increase of 6.7 mm3 per year.
Non-calcified plaque volume went from 27.5 mm3 to 53.5 mm3, an annualized increase of 4.9 mm3 per year. This is the plaque type most strongly associated with future heart attacks.
Calcified plaque volume increased as well, though more slowly, from 0.3 mm3 to 3.2 mm3.
Perhaps most concerning: low attenuation plaque, the lipid-rich, inflamed, vulnerable subtype, was present in only 9 percent of participants at baseline. By follow-up, that number had risen to 23 percent.
And remember: 54 percent of these people started with a CAC score of zero. Meaning if you had only used a CAC score to evaluate them, more than half would have been told "you have no calcified plaque, you're fine."
The CAC Zero Problem
I want to stop here because this is critical. A CAC score of zero is genuinely reassuring, and I am not here to dismiss its value. A zero CAC is associated with a very low short-term cardiovascular risk, and it remains a useful tool.
But a CAC score only detects calcified plaque. It tells you nothing about the non-calcified, lipid-rich plaque that is quietly building inside your arterial walls right now. This study found that even people with a CAC of zero had detectable non-calcified plaque at baseline, and that plaque grew substantially over five years without any symptoms and without triggering any events.
This is exactly why ApoB matters more than LDL-C for understanding your true atherogenic burden. Every LDL particle, every VLDL particle, every remnant lipoprotein that crosses into your arterial wall contributes to plaque. ApoB counts them all. And at an average LDL of 111 mg/dL in this study, most of these people would have been told by a standard risk calculator that they did not need a statin. Their arteries disagreed.
Non-Calcified Plaque Is Growing Faster, and That Is the Dangerous Kind
One of the most important findings in this paper is that non-calcified plaque accumulated much faster than calcified plaque. This is not a coincidence. It reflects the biology of atherosclerosis.
Calcified plaque represents older, more stable, remodeled disease. Non-calcified plaque, especially low attenuation plaque, represents the active, lipid-rich, inflamed lesions that are most likely to rupture and cause a heart attack. The SCOT-HEART trial established clearly that low attenuation plaque burden is strongly associated with future myocardial infarction.
The fact that low attenuation plaque prevalence went from 9 percent to 23 percent in this relatively healthy cohort over five years tells us that the window for prevention is earlier than most people think. By the time plaque is calcified, the disease has already been marinating for years.
A Small Subset Was Progressing Rapidly
The study also identified a subgroup of participants who were progressing at an alarming rate using established thresholds from the PARADIGM registry.
Three percent of participants met criteria for rapid plaque progression, defined as an annual percent atheroma volume increase of 1 percent or more per year. Another 11 percent met an intermediate threshold of 0.59 percent per year.
These individuals had no symptoms. No events. No medications. Nothing in their clinical profile flagged them as urgently at risk. The only way to identify them was through serial imaging.
This raises a serious question about who we are missing in standard clinical practice.
What This Means for You
Let me be direct. I am not saying everyone needs a CCTA. I am not saying everyone needs a statin. What I am saying is that the conventional framework of "wait until you have symptoms or a cardiac event before we take this seriously" is wrong and the data keep confirming it.
Atherosclerosis is a decades-long, silent process. It does not ask for your permission. It does not wait until your cholesterol crosses some arbitrary threshold. It accumulates day by day, driven primarily by the number of atherogenic particles circulating in your blood and the duration of their exposure to your arterial wall.
The people in this study had what most clinicians would describe as a reassuring risk profile. Minimal calcium. No history of heart disease. No medications that would bias the result. And yet, over five years, virtually all of them showed meaningful plaque growth, with the most dangerous plaque subtypes becoming more prevalent.
The lesson here is not to panic. It is to get serious about prevention earlier. Know your ApoB. Know your Lp(a). Consider a CAC score, with the understanding of its limitations for detecting non-calcified disease. Talk to a cardiologist who is focused on prevention, not just treatment of established disease.
Limitations Worth Acknowledging
In the spirit of intellectual honesty that I hold myself to on this platform, here are the real limitations of this study.
It was retrospective, meaning the researchers looked back at existing data rather than prospectively designing a controlled trial. The sample was 72 percent white men, limiting generalizability. The cohort came from clinically indicated scans, not random population sampling, which means selection bias exists. Undocumented use of lipid-lowering therapy could not be fully excluded. And importantly, the study did not adjudicate outcomes, meaning we cannot directly connect the plaque findings to future events in this specific cohort.
None of these limitations change the core message. They just remind us that this is one piece of a larger evidentiary puzzle, not the final word.
Infographic Summary:
Zero CAC Score Bottom Line
Coronary atherosclerosis progresses silently, even in adults who feel healthy, have low calcium scores, normal-ish LDL levels, no prior heart attack, and no medications. Non-calcified plaque, the most dangerous kind, accumulates faster than calcified plaque. And a substantial minority of seemingly low-risk adults are progressing rapidly with no clinical warning signs whatsoever.
This is why I keep emphasizing that the goal of cardiovascular medicine is not to treat your first heart attack. It is to prevent it from ever happening. And that requires taking subclinical atherosclerosis seriously, years before the typical alarm bells go off.
If you want to know more about how I approach risk assessment, plaque imaging, and evidence-based prevention in my patients, join the Heart 2 Heart VIP Community at dralo.net/community. This is where I go deeper on exactly this kind of data every week.
Reference:
Aldana-Bitar J, Krishnan S, Ichikawa K, et al. NATURal history of coronary PlaquE on cardiac computed tomography in individuals without MACE or lipid-lowering therapy: NATURE-CT study. Journal of Cardiovascular Computed Tomography. 2026. https://doi.org/10.1016/j.jcct.2026.05.002
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















