

Sleep Apnea The Silent Heart Killer!
May 23, 2026
Sleep Apnea and Heart Disease: A Cardiologist's Full Breakdown
Your partner tells you that you snore. You wake up exhausted no matter how many hours you sleep. You have been told you stop breathing in the night. You brush it off as a nuisance.
Here is what I need you to understand: obstructive sleep apnea is not a nuisance. It is a serious cardiovascular disease driver, and it is almost certainly underdiagnosed in your doctor's office right now.
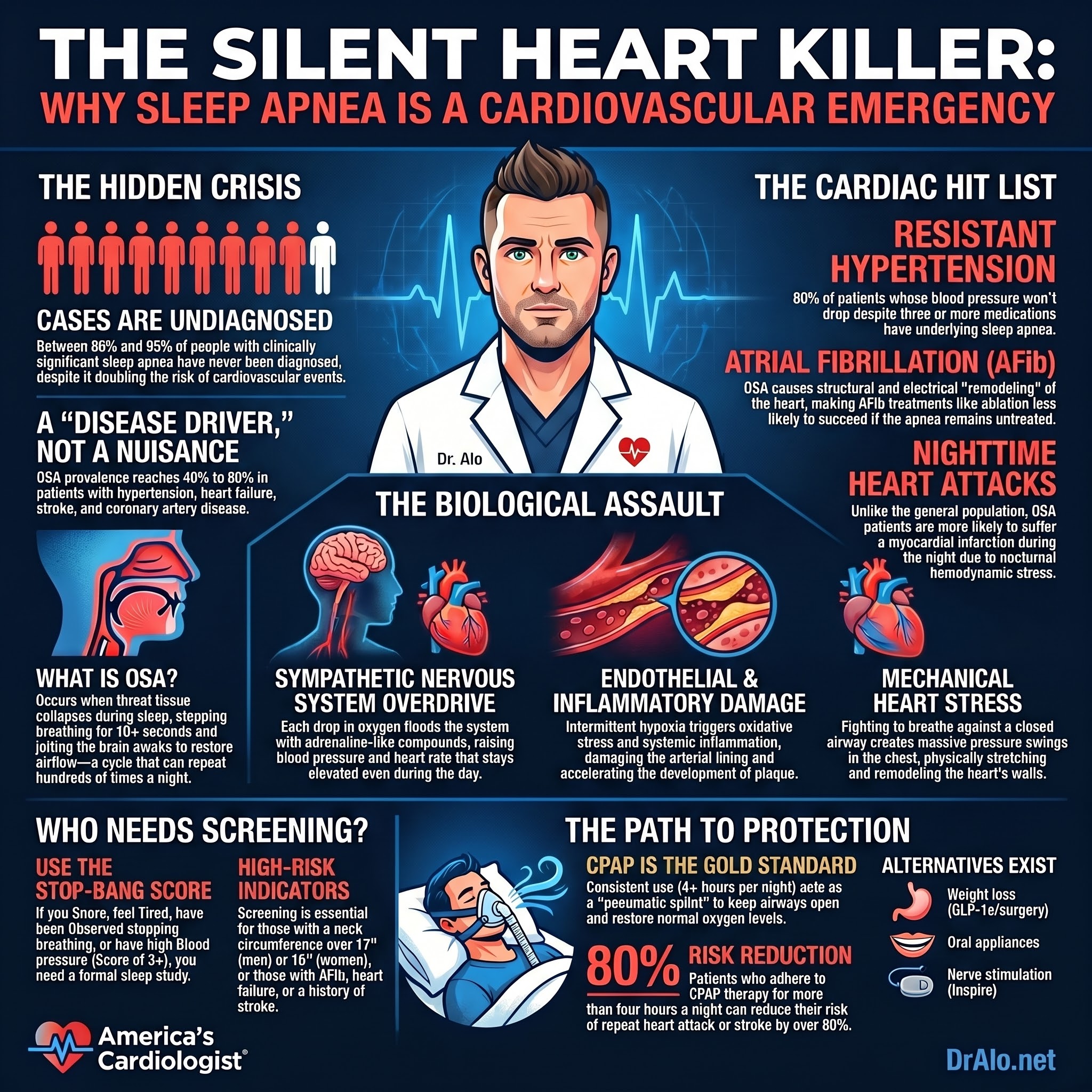
The American Heart Association published a scientific statement in Circulation in 2021 that laid this out clearly. OSA prevalence reaches as high as 40 to 80 percent in patients with hypertension, heart failure, coronary artery disease, pulmonary hypertension, atrial fibrillation, and stroke. And yet, between 86 and 95 percent of people with clinically significant OSA have never been diagnosed.
Let that sink in. Most people walking around with a condition that doubles their risk of cardiovascular events have no idea they have it.
I am going to walk you through what sleep apnea actually is, why it wrecks your cardiovascular system at a biological level, which specific heart conditions it drives, and what the evidence actually says about treatment. No fluff. No oversimplification. Real cardiology.
Infographic Summary:
What Is Obstructive Sleep Apnea, and How Common Is It?
Obstructive sleep apnea (OSA) occurs when the soft tissue in your throat repeatedly collapses during sleep, partially or completely blocking your airway. Each time this happens, breathing stops for at least 10 seconds, sometimes much longer. Your brain detects the oxygen drop and jolts you partially awake to restore airflow. This cycle can repeat dozens or even hundreds of times per night without you ever being fully aware of it.
There is a second type called central sleep apnea, where the brain simply fails to send the right signals to the breathing muscles. It is less common but carries its own set of cardiovascular complications, particularly in patients with existing heart failure.
The numbers on OSA prevalence are staggering. Approximately 34 percent of middle-aged men and 17 percent of middle-aged women meet the diagnostic criteria. Globally, an estimated 936 million adults aged 30 to 69 are affected. In the United States, in clinical cardiovascular practices, OSA is found in 40 to 80 percent of patients with high blood pressure, heart failure, coronary artery disease, atrial fibrillation, and stroke.
Severity is classified by the apnea-hypopnea index (AHI), which counts breathing disruptions per hour of sleep. Mild is 5 to 14 events per hour. Moderate is 15 to 30. Severe is above 30. But here is something cardiologists have learned: event count alone does not capture the full cardiovascular risk picture. The total hypoxic burden, meaning how much time your oxygen saturation spends below normal, is actually a stronger predictor of cardiovascular mortality than the AHI alone.
Who Is at Risk for Sleep Apnea?
Certain factors put you squarely in the crosshairs. Obesity is the single biggest modifiable risk factor. A 10 percent weight gain is associated with a 32 percent increase in AHI. Even modest weight control substantially reduces the incidence of sleep-disordered breathing.
Neck circumference matters more than most people realize. Neck sizes above 17 inches in men and 16 inches in women are particularly associated with OSA, and neck circumference can be an even stronger predictor of OSA severity than BMI alone.
Other established risk factors include male sex, older age, craniofacial anatomy (retrognathia, large tonsils, narrowed upper airway), smoking, family history, and nighttime nasal congestion. Alcohol, benzodiazepines, and opioids do not cause OSA but they absolutely worsen it by further relaxing upper airway muscles.
And I want to make this point clearly: Black patients are disproportionately affected by undiagnosed OSA. Structural inequities in healthcare access and screening have left this population particularly vulnerable. This is a health equity issue as much as it is a cardiology issue.
The Biology: How Sleep Apnea Destroys Your Cardiovascular System
This is where most patient-facing articles fall short. They tell you that sleep apnea is "linked" to heart disease without explaining why. That is not good enough. You deserve to understand the actual biology.
Every time you stop breathing, your blood oxygen drops. When oxygen returns, there is a surge of reactive oxygen species, the same cellular stress seen in ischemia-reperfusion injury, meaning it resembles what happens to heart tissue during a heart attack at a microscopic level, happening repeatedly every night.
Here is what that cascade triggers:
Sympathetic nervous system overdrive. Intermittent hypoxia activates your carotid body chemoreceptors, which fire off signals that flood your system with adrenaline-like compounds. This sympathetic surge raises your heart rate and blood pressure acutely during each apnea. The problem is that this sympathetic activation does not fully resolve when you wake up. Patients with OSA have elevated sympathetic tone throughout the day, not just at night.
RAAS activation. The renin-angiotensin-aldosterone system is turned on by intermittent hypoxia. This promotes salt and water retention, vasoconstriction, and sustained elevation of blood pressure. It also contributes to cardiac remodeling over time.
Endothelial dysfunction. The arterial lining loses its ability to produce nitric oxide and regulate vascular tone. This is a foundational step in the development of atherosclerosis. OSA accelerates this process through oxidative stress and systemic inflammation.
Systemic inflammation. Intermittent hypoxia activates the nuclear transcription factor NF-kB, which drives the release of pro-inflammatory cytokines including TNF-alpha and interleukin-6. Chronic low-grade inflammation is a cornerstone of atherosclerotic plaque development, plaque instability, and acute cardiovascular events.
Intrathoracic pressure swings. Every time the airway obstructs and you fight to breathe against it, you generate massive negative pressure swings in your chest. These swings physically stress the walls of your heart, increasing both preload (the volume of blood the heart must fill with) and afterload (the resistance it must pump against). Over time, this mechanical stress contributes to atrial and ventricular remodeling.
The result of all these mechanisms running simultaneously, night after night, year after year, is a cardiovascular system that ages faster than it should.
Sleep Apnea and Hypertension: The Most Common Intersection
The relationship between OSA and high blood pressure is well established and bidirectional. OSA is present in 30 to 50 percent of all hypertensive patients. Among those with resistant hypertension, the patients whose blood pressure does not come under control despite three or more medications, the prevalence of OSA reaches up to 80 percent.
If your blood pressure is difficult to control and no one has screened you for sleep apnea, something is missing from your workup.
The AHA scientific statement from Circulation recommends screening for OSA specifically in patients with resistant or poorly controlled hypertension. This is not a soft suggestion. It is a formal clinical recommendation backed by data.
Does CPAP therapy lower blood pressure? Yes, but modestly. Meta-analyses show reductions of roughly 2 to 3 mmHg in both systolic and diastolic pressure. In patients with resistant hypertension, a 3-month CPAP trial produced similar reductions, with greater benefit tied directly to hours of use per night. The more compliant the patient, the more the blood pressure came down.
CPAP is not a replacement for antihypertensive medications. But it is an important complementary intervention, and ignoring OSA in a hypertensive patient leaves a major driver of elevated blood pressure untreated.
Sleep Apnea and Atrial Fibrillation: A Critical Connection
OSA is an independent risk factor for atrial fibrillation. This is one of the most clinically important relationships in all of cardiovascular medicine, and it is still underappreciated in practice.
Here is the mechanism. During each apnea, there is acute hypoxia, hypercapnia, surging sympathetic tone, and a sudden negative shift in intrathoracic pressure. Repeated exposure to these stressors causes structural and electrical remodeling of the atria. The atrial tissue develops fibrosis. Connexin proteins, which govern electrical conduction between cells, are downregulated. The result is an atrial substrate that is prone to the chaotic electrical activity that defines atrial fibrillation.
OSA also generates triggers for AF that originate outside the pulmonary veins, which is clinically significant because standard AF ablation procedures typically focus on pulmonary vein isolation. In patients with uncontrolled OSA, the ablation success rate is lower for this reason.
The clinical data are compelling. In a cohort of 10,132 patients with atrial fibrillation and OSA, those treated with CPAP were significantly less likely to progress to permanent atrial fibrillation than those without CPAP. Treating the OSA improved outcomes regardless of whether rhythm control was managed with antiarrhythmic drugs, direct cardioversion, or catheter ablation.
A 2025 study published in the Journal of the American Heart Association confirmed that untreated OSA significantly worsens both arrhythmia recurrence and quality-of-life outcomes after catheter ablation. The message for clinicians and patients alike: if you have atrial fibrillation and you have not been screened for sleep apnea, that is an incomplete evaluation.
Sleep Apnea and Heart Failure
Sleep-disordered breathing is found in 40 to 60 percent of patients with symptomatic heart failure. That is not a rounding error. That is the majority of heart failure patients.
In patients with heart failure with reduced ejection fraction, central sleep apnea tends to dominate over obstructive sleep apnea. The two have different mechanisms and require different treatment approaches, which is why formal sleep testing is essential rather than simply assuming one type over the other.
OSA worsens heart failure through several pathways: neurohormonal activation (increasing sympathetic tone and RAAS activity), increased myocardial oxygen demand from the intrathoracic pressure swings, and exacerbation of systemic hypertension.
The ACC/AHA heart failure guidelines have identified CPAP as a reasonable treatment strategy in patients with heart failure and OSA to improve sleep quality and daytime function. Small-scale studies have reported improvements in left ventricular function and reductions in heart failure hospitalizations with CPAP use.
One important caveat: adaptive servo-ventilation (ASV), a more advanced form of positive pressure therapy, was found to increase mortality in patients with heart failure with reduced ejection fraction and central sleep apnea in the SERVE-HF trial. This distinction matters. Patients with heart failure should not simply be placed on any positive airway pressure device. They need a careful sleep study interpretation to identify the predominant phenotype before treatment is initiated.
Sleep Apnea and Coronary Artery Disease
OSA independently increases coronary risk through the same oxidative stress and inflammation pathways discussed earlier. The repetitive cycles of hypoxia and reoxygenation accelerate atherosclerosis, promote coronary plaque instability, and increase the vulnerability of plaques to rupture.
OSA has been associated with a two-fold increase in the risk of major cardiovascular events or death in patients with coronary artery disease. Patients with OSA are more likely to suffer myocardial infarction during the nighttime hours rather than the morning hours that are typical in people without OSA. This nocturnal shift in MI timing is a direct consequence of the hemodynamic and autonomic stressors that OSA generates during sleep.
The RICCADSA trial provides some of the most striking CPAP data available. In post-acute coronary syndrome patients with OSA, those who used CPAP for more than four hours per night reduced their composite risk of repeat revascularization, myocardial infarction, stroke, and cardiovascular death by more than 80 percent compared to non-adherent patients. That is an extraordinary risk reduction, and it was driven entirely by treatment adherence.
Compliance matters here more than in almost any other medication or therapy in cardiovascular medicine. Using CPAP for fewer than four hours per night produces substantially less cardiovascular benefit.
Sleep Apnea, Stroke, and Sudden Cardiac Death
A meta-analysis found that 71 percent of post-stroke patients have OSA, with this figure holding across acute, subacute, and chronic time points after the stroke. OSA is not just a complication of stroke. It is an independent risk factor for having a stroke in the first place, and for stroke recurrence, cognitive decline, and death afterward.
The mechanisms overlap with those driving coronary disease: hypercoagulability, oxidative stress, systemic inflammation, autonomic dysfunction, and impaired cerebral hemodynamics. The association between OSA and stroke is not explained by hypertension or other traditional risk factors alone.
Beyond stroke, OSA is linked to a spectrum of arrhythmias including bradycardia, long pauses, sick sinus syndrome, and ventricular tachycardia. In a 15-year longitudinal study of 10,701 adults, OSA predicted incident sudden cardiac death. The highest-risk patients were those over age 60, with mean nocturnal oxygen saturation below 78 percent, and an AHI above 20. One striking finding from this research: in patients with implanted pacemakers for sick sinus syndrome, 58 percent had previously undiagnosed sleep apnea.
The AHA scientific statement formally recommends evaluation for sleep apnea in patients with tachy-brady syndrome, ventricular tachycardia, and survivors of sudden cardiac death.
Does CPAP Actually Protect Your Heart? What the Evidence Really Shows
This is where I need to be precise, because both the oversellers and the undersellers get this wrong.
CPAP is the gold standard treatment for OSA. It works by maintaining continuous positive pressure in the airway, acting as a pneumatic splint that prevents the airway from collapsing. When used consistently, it eliminates apneic events and restores normal sleep architecture and oxygenation.
The evidence on cardiovascular outcomes is nuanced. Large randomized controlled trials including the SAVE trial have not shown significant reduction in major cardiovascular events with CPAP in non-sleepy patients with moderate to severe OSA. This has led some to conclude that CPAP does not protect the heart. That conclusion is too fast.
The issue is adherence. In clinical trials, CPAP adherence is typically 40 to 80 percent when defined as use for at least four hours per night. When researchers look specifically at patients who actually use CPAP consistently, the cardiovascular benefits become substantial and consistent.
In the RICCADSA post-hoc analysis, adherent patients reduced their composite cardiovascular event risk by over 80 percent. A 2024 study in Archives of Bronchopneumology found that CPAP continuators had a 39 percent lower risk of cardiovascular death compared to those who stopped therapy, after adjustment for age, sex, and key comorbidities. A 2025 Lancet Respiratory Medicine meta-analysis synthesizing data from randomized trials and observational studies further supported that consistent positive airway pressure use reduces mortality, particularly in patients with severe disease.
In the Sleep Heart Health Study, a PAP prescription was associated with 42 percent lower mortality in patients with severe OSA, but the benefit was not statistically apparent until six to seven years of follow-up. This is consistent with how we think about other long-term cardiovascular interventions. Statins, antihypertensives, and antiplatelet agents also require sustained use over years before their full mortality benefit is captured in clinical trials.
The bottom line: CPAP works when you use it. The tragedy is that non-adherence is the rule rather than the exception, and we need much better tools to support patients in sustaining therapy.
Treatment Options Beyond CPAP
CPAP is the most effective therapy for moderate to severe OSA, but it is far from the only option.
Oral appliances, specifically mandibular advancement devices, are a validated alternative for mild to moderate OSA or for patients who cannot tolerate CPAP. They produce blood pressure reductions comparable to CPAP in meta-analyses and are often better tolerated, which means higher real-world adherence.
Weight loss is powerful. A 10 percent reduction in body weight produces a 26 percent decrease in AHI on average. In patients with significant obesity, GLP-1 receptor agonists and bariatric surgery have shown substantial improvements in sleep apnea severity, which is another reason the cardiovascular benefits of these interventions extend well beyond glycemic control and weight reduction alone.
Positional therapy is appropriate for patients whose apnea occurs predominantly in the supine position. Upper airway surgery and hypoglossal nerve neurostimulation (Inspire therapy) are options for carefully selected patients who have moderate to severe OSA and cannot tolerate CPAP. Neurostimulation in particular has shown significant AHI reductions and improved patient-reported outcomes.
The key principle: all patients with OSA should be offered treatment. The right treatment depends on OSA severity, anatomy, comorbidities, and patient preference. Doing nothing is not a neutral choice.
Who Should Be Screened? The Clinical Recommendations
The AHA 2021 scientific statement from Circulation provides specific recommendations on which cardiovascular patients warrant formal sleep apnea evaluation. These are the categories where the evidence supports proactive screening:
Resistant or poorly controlled hypertension. Pulmonary hypertension. Recurrent atrial fibrillation after either cardioversion or catheter ablation. New York Heart Association class II to IV heart failure with symptoms suggestive of sleep-disordered breathing or excessive daytime sleepiness. Tachy-brady syndrome or sick sinus syndrome. Ventricular tachycardia. Survivors of sudden cardiac death. Patients with nocturnally occurring angina, myocardial infarction, or appropriate shocks from an implanted cardioverter-defibrillator.
Screening tools include the STOP-BANG questionnaire (Snoring, Tiredness, Observed Apnea, high Blood Pressure, BMI over 35, Age over 50, Neck circumference over 40 cm, male Gender), which has sensitivity between 77 and 89 percent for detecting OSA. A STOP-BANG score of 3 or higher warrants formal sleep testing. Home sleep apnea tests are increasingly accessible and appropriate for many patients. Full in-laboratory polysomnography remains the gold standard, particularly for complex cases involving heart failure or suspected central sleep apnea.
The Bottom Line: Sleep Apnea Is a Cardiovascular Disease
If you snore loudly, wake up unrested, feel sleepy throughout the day, or have been told you stop breathing at night, please bring this up with your physician. Do not wait for your cardiologist to ask you about it because, statistically, they probably will not.
If you have resistant hypertension, atrial fibrillation, heart failure, coronary artery disease, or a history of stroke and you have never had a formal sleep evaluation, that is a gap in your care that needs to be addressed.
And if you already have a CPAP machine that is sitting in your closet unused, I need you to understand something clearly. The data showing cardiovascular protection with CPAP comes specifically from patients who actually use it. Four hours per night is the minimum meaningful threshold. Seven or more hours is where the benefit is maximized.
Sleep apnea is not a lifestyle inconvenience. It is a biological assault on your cardiovascular system that happens hundreds of times per night, every night, until it is treated. The biology is real. The risk is real. And the treatment works.
Get the sleep study. Use the therapy. Your heart depends on it.
References
Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144:e56-e67. https://doi.org/10.1161/CIR.0000000000000988
Javaheri S, Javaheri S, Gozal D, et al. Interactions of obstructive sleep apnea with the pathophysiology of cardiovascular disease, Part 1: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2024;84(13):1224-1240. https://www.sciencedirect.com/science/article/pii/S0735109724079646
Pintilie AL, Marcu DTM, Zabara-Antal A, et al. Sleep apnea: the slept-upon cardiovascular risk factor. Biomedicines. 2025;13(10):2529. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12562078/
Gami AS, Olson EJ, Shen WK, et al. Obstructive sleep apnea and the risk of sudden cardiac death: a longitudinal study of 10,701 adults. Journal of the American College of Cardiology. 2013;62:610-616. https://doi.org/10.1016/j.jacc.2013.04.080
McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. New England Journal of Medicine. 2016;375:919-931. https://doi.org/10.1056/NEJMoa1606599
Peker Y, Glantz H, Eulenburg C, et al. Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease patients with nonsleepy obstructive sleep apnea: the RICCADSA randomized controlled trial. American Journal of Respiratory and Critical Care Medicine. 2016;194:613-620. https://doi.org/10.1164/rccm.201601-0088OC
de Batlle J, Gracia-Lavedan E, Escarrabill J, et al. Effect of CPAP treatment on cardiovascular outcomes. Archivos de Bronconeumologia. 2024;60(10):627-633. https://doi.org/10.1016/j.arbres.2024.05.029
Hu J, Zuo S, Qian J, et al. The effect of continuous positive airway pressure therapy on atrial fibrillation in patients with obstructive sleep apnea. Frontiers in Medicine. 2025;12. https://doi.org/10.3389/fmed.2025.1509776
Holmqvist F, Guan N, Zhu Z, et al. Impact of obstructive sleep apnea and CPAP therapy on outcomes in patients with atrial fibrillation: results from ORBIT-AF. American Heart Journal. 2015;169:647-654. https://doi.org/10.1016/j.ahj.2014.12.024
Azarbarzin A, Sands SA, Stone KL, et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study. European Heart Journal. 2019;40:1149-1157. https://doi.org/10.1093/eurheartj/ehy624
Oyarce MP, Iturriaga R. Contribution of oxidative stress and inflammation to the neurogenic hypertension induced by intermittent hypoxia. Frontiers in Physiology. 2018;9:893. https://doi.org/10.3389/fphys.2018.00893
American Heart Association. Sleep apnea worsens heart disease, yet often untreated. AHA Scientific Sessions 2021 press release. https://newsroom.heart.org/news/sleep-apnea-worsens-heart-disease-yet-often-untreated
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















