

Statins Reduce Testosterone? What The Science Really Says!
May 14, 2026
Do Statins Lower Testosterone?
I get this question constantly. A patient comes in for their lipid management follow-up, and almost before they sit down, they want to know: is my statin destroying my testosterone? They have read something online, or a friend told them, or they watched a video where someone explained that cholesterol is the precursor to all your sex hormones, so of course lowering it would lower your testosterone.
It is a reasonable thing to wonder about. Cholesterol is indeed the biochemical starting point for every steroid hormone in the body, including testosterone, estrogen, cortisol, and DHEA. Statins work by inhibiting HMG-CoA reductase, the rate-limiting enzyme in cholesterol synthesis. On paper, the concern seems logical.
Clinical reality, however, is not always what theory predicts. And in this case, the gap between the theoretical risk and what actually happens in the human body is substantial.
Let me take you through the evidence, because this is a question that deserves a real answer, not a dismissal and not a scare.
Statins do not cause clinically meaningful reductions in testosterone or other steroid hormones. This conclusion is supported by randomized trials, systematic reviews, large observational cohorts, and the explicit statements of two major medical societies.
Why This Fear Has Persisted
The concern has two sources: basic biochemistry and the internet.
The biochemistry is legitimate as a theoretical starting point. Steroidogenic tissues, the adrenal glands, testes, and ovaries, use cholesterol as their raw material for hormone synthesis. If you dramatically reduce circulating cholesterol, the theory goes, those tissues might be starved of substrate.
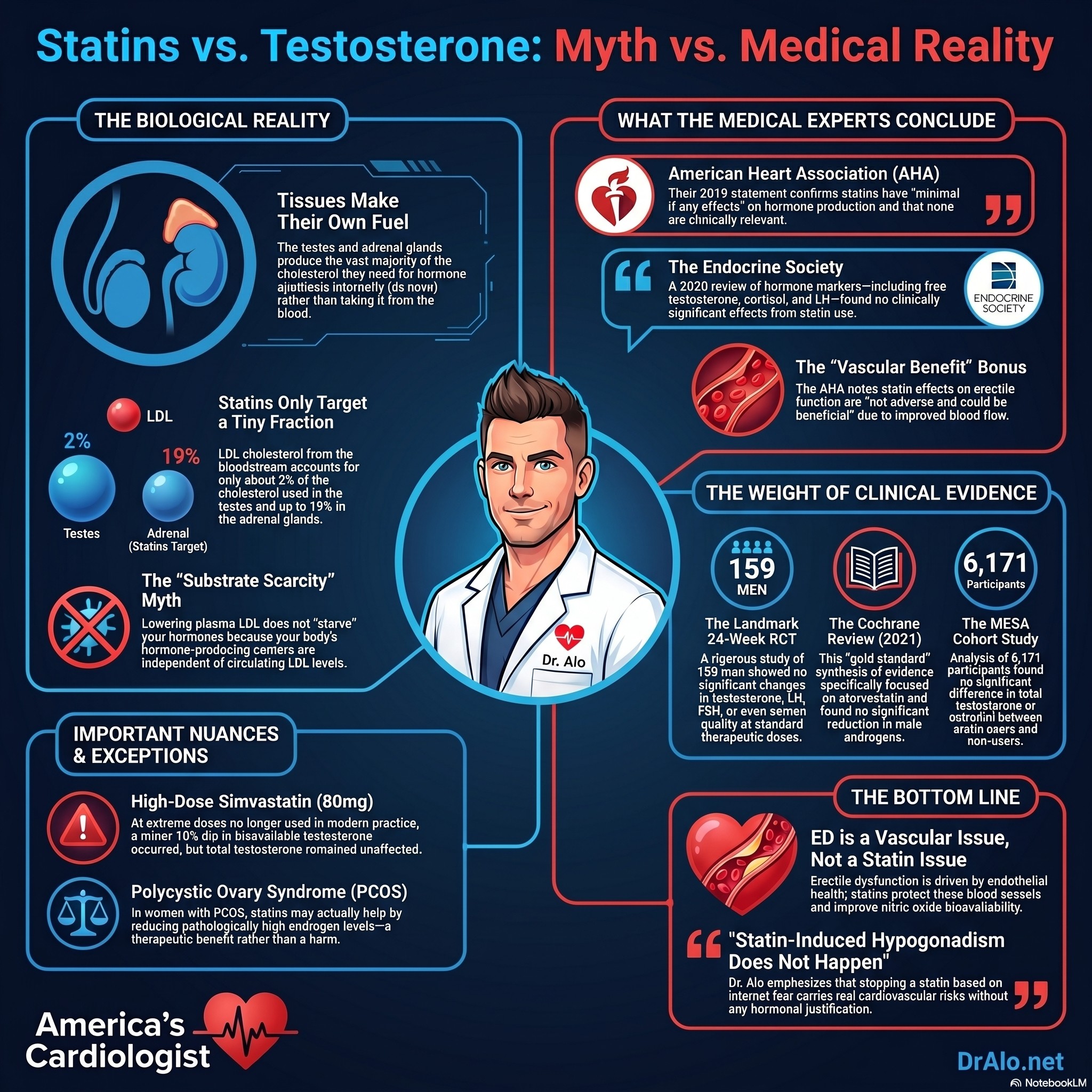
The problem with this theory is that it ignores how these tissues actually operate. They do not depend primarily on circulating LDL cholesterol for their hormone production. Steroidogenic tissues get the vast majority of their cholesterol from two sources: de novo synthesis within the tissue itself, and selective uptake of HDL cholesteryl esters via the SR-BI receptor. LDL uptake through the classical clathrin-coated pit pathway contributes a minor fraction, roughly 2% in the testes and up to 19% in the adrenal glands. These tissues are largely self-sufficient in cholesterol supply, independent of what your plasma LDL does.
The internet amplifies the fear beyond what any evidence supports. Wellness forums, supplement marketers, and people who sell testosterone optimization programs have a financial interest in making you afraid of your statin. I want you to have the actual data.
Statin Testosterone Infographic Summary:
What the Major Medical Societies Have Concluded
Two of the most respected bodies in medicine have addressed this directly.
The American Heart Association concluded in its 2019 Scientific Statement on statin safety that statins have "minimal if any effects on steroidogenesis, and none are clinically relevant." The statement also noted that the effect of statins on erectile function "is not adverse and could be beneficial." That last point is worth emphasizing: not neutral, potentially beneficial. The reason is that cardiovascular disease is a leading driver of erectile dysfunction, and statins protect vascular endothelial function.
The Endocrine Society reached the same conclusion in its 2020 Clinical Practice Guideline on lipid management in patients with endocrine disorders. After reviewing studies of lovastatin, simvastatin, and pravastatin, the Society found no clinically significant effect on cortisol, ACTH, basal and HCG-stimulated testosterone, free testosterone index, SHBG, LH, or FSH. Every major hormone marker evaluated came back clean.
Two independent societies, one focused on the heart and one focused on the endocrine system, reviewed the same body of evidence and arrived at the same conclusion. That level of concordance carries real weight.
What the Randomized Trial Data Show
The Landmark 24-Week RCT
The most rigorous study on this question randomized 159 men to one of four groups: simvastatin 20 mg, simvastatin 40 mg, pravastatin 40 mg, or placebo. The trial ran for 24 weeks, long enough to detect any sustained hormonal effects.
Results: no significant between-group differences in basal or stimulated testosterone, free testosterone index, SHBG, LH, FSH, or semen quality. At standard therapeutic doses across two different statins, there was simply no signal.
The Supratherapeutic Dose Study
A separate trial pushed simvastatin to 80 mg, a dose that is no longer recommended in routine clinical practice due to muscle-related risks. Even at this supra-therapeutic level, only one finding emerged: approximately a 10% decline in bioavailable testosterone relative to placebo.
Total testosterone, free testosterone, gonadotropins, and SHBG remained completely unaffected. A 10% shift in a single testosterone fraction at a dose nobody should be taking sits well within normal physiological variation and is not associated with any symptoms of hypogonadism.
Women: The Simvastatin Menstrual Cycle Study
In premenopausal women, a study of simvastatin 40 mg found no effect on the menstrual cycle or progesterone synthesis compared to placebo. Hormonal regulation in premenopausal women is highly sensitive and tightly coordinated. If statins disrupted the endocrine axis in any meaningful way, this is where you would expect to see it. You do not.
Systematic Reviews and Large Cohort Data
The Cochrane Review on Atorvastatin
Cochrane Reviews represent the top tier of evidence synthesis in medicine. A 2021 Cochrane systematic review specifically examined the effect of atorvastatin on testosterone levels in male patients. The conclusion: no significant reduction in androgens.
The authors appropriately noted limitations including potential publication bias and modest study sizes. But the directional consistency with the full evidence base is clear.
The MESA Cohort
The Multi-Ethnic Study of Atherosclerosis (MESA) is one of the most rigorously characterized cardiovascular cohort studies in the literature, covering 6,171 participants. A cross-sectional analysis of statin users versus non-users in this cohort found modestly lower SHBG and DHEA in statin users. However, there were no statistically significant differences in total testosterone, bioavailable testosterone, or estradiol.
Observational data cannot establish causation. But MESA adds to the consistent picture: across different study designs, at scale, statins are not associated with meaningful changes in testosterone.
Evidence at a Glance
|
Source / Study |
Key Finding on Testosterone / Hormones |
|
AHA 2019 Scientific Statement |
Minimal if any effects on steroidogenesis; none are clinically relevant. Erectile function effect "not adverse and could be beneficial." |
|
Endocrine Society 2020 Guideline |
No clinically significant effect on cortisol, testosterone (basal and stimulated), free testosterone index, SHBG, LH, or FSH. |
|
Landmark 24-Week RCT (n=159 men) |
No significant changes in testosterone, free testosterone index, SHBG, LH, FSH, or semen quality at standard statin doses. |
|
Supratherapeutic Simvastatin 80 mg |
~10% decline in bioavailable testosterone only; total T, free T, gonadotropins, and SHBG all unaffected. |
|
Simvastatin 40 mg in women |
No effect on menstrual cycle or progesterone synthesis vs. placebo. |
|
Cochrane Review on Atorvastatin (2021) |
No significant reduction in androgens in male patients. |
|
MESA Cohort (n=6,171) |
No significant differences in total T, bioavailable T, or estradiol between statin users and non-users. |
One Legitimate Nuance: PCOS
No honest review of this topic leaves out polycystic ovary syndrome (now PMOS: polyendocrine metabolic ovarian syndrome). In women with PCOS or PMOS, excess androgens are part of the pathophysiology and drive many of its symptoms. A 2023 Cochrane Review found some evidence that statins may reduce androgen levels in women with PCOS, though the certainty of the evidence was rated as very low.
If this effect is real, it could actually be therapeutically useful in this specific population, not a harm. But more data are needed before drawing firm conclusions.
For everyone else, men and women without PCOS, there is no meaningful androgen reduction with statins at standard doses.
What About Erectile Dysfunction?
Some patients specifically worry that lowering cholesterol will impair erectile function because testosterone is involved in libido and sexual performance. Here is what the evidence actually shows.
Erectile dysfunction is fundamentally a vascular problem. The mechanism is endothelial dysfunction, reduced nitric oxide bioavailability, and impaired smooth muscle relaxation in penile vasculature. The same atherosclerotic process that narrows coronary arteries also narrows the arteries supplying the penis.
Statins improve endothelial function, reduce oxidative stress, and have pleiotropic anti-inflammatory effects that benefit vascular health broadly. This is why the AHA specifically noted that the effect of statins on erectile function is "not adverse and could be beneficial." Treating the cardiovascular disease treats the vascular component of erectile dysfunction.
If a patient is experiencing sexual dysfunction on a statin, the reflex should not be to blame the statin. It should be to look at cardiovascular risk comprehensively, because the more likely explanation is that the underlying vascular disease is progressing.
Statins do not impair testosterone production at standard doses. If anything, their cardiovascular and vascular benefits may support erectile function rather than undermine it.
The Bottom Line from America's Cardiologist
Here is what I tell my patients directly.
The fear that your statin is tanking your testosterone is not supported by the evidence. It is supported by wellness influencers, supplement marketers, and people who would prefer you stop your statin and buy something from them instead. Those are not the same thing as evidence.
Your steroidogenic tissues, the parts of your body responsible for producing testosterone, estrogen, and cortisol, do not depend primarily on circulating LDL cholesterol. They make their own. That is the biology, and it explains why decades of randomized trial data, Cochrane reviews, large observational cohorts, and the formal statements of both the American Heart Association and the Endocrine Society all point in the same direction: statins at standard doses do not cause clinically meaningful reductions in testosterone or other steroid hormones.
There is one real caveat worth knowing: at 80 mg of simvastatin, a dose that is not used in modern practice, a modest reduction in bioavailable testosterone was observed. Total testosterone and every other hormone marker remained unaffected. This is not a clinical concern. It is a data point that deserves context.
If you are experiencing symptoms that make you wonder about your testosterone, that is a conversation worth having with your physician. But stopping your statin based on internet fear is not the answer, and it is a choice that carries real cardiovascular consequences.
The weight of evidence from randomized trials, systematic reviews, large cohort studies, and two major medical societies is consistent: statins at standard doses do not meaningfully lower testosterone or impair steroidogenesis. Cardiovascular disease kills. Statin-induced hypogonadism does not happen.
Key References
Evidence cited in this article includes the following peer-reviewed sources:
- American Heart Association Scientific Statement on Statin Safety (2019). Circulation.
- Endocrine Society Clinical Practice Guideline on Lipid Management in Endocrine Disorders (2020). Journal of Clinical Endocrinology and Metabolism.
- Randomized controlled trial of simvastatin and pravastatin in 159 men: testosterone and reproductive hormone outcomes (24-week follow-up).
- Simvastatin 80 mg and bioavailable testosterone: supratherapeutic dose RCT findings.
- Simvastatin 40 mg in premenopausal women: menstrual cycle and progesterone synthesis RCT.
- Cochrane Systematic Review: Effect of atorvastatin on testosterone levels in male patients (2021).
- Cochrane Systematic Review: Statins and androgen levels in women with PCOS (2023).
- Stamerra et al. (2021). Statins and sex hormones: A comprehensive review. European Journal of Pharmacology.
- MESA Cohort cross-sectional analysis: statin use and sex hormone levels (n=6,171).
- Xie et al. Cholesterol substrate pools and steroid hormone levels in steroidogenic tissues. Journal of Lipid Research.
Dr. Mohammed Alo DO, FACC | Board-Certified Cardiologist & Internist | Advanced Lipidology | Obesity Medicine
Professor of Medicine, Ohio University & Midwestern University | dralo.net
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















