

What Is apoB? Cardiologist Explains!
May 29, 2026
What Is ApoB? A Cardiologist Explains Apolipoprotein B, the Best Predictor of Heart Attack Risk
Let me tell you the number I care about more than almost anything else on your lipid panel. It is not your LDL cholesterol. It is your ApoB, short for apolipoprotein B. If your doctor has told you your LDL is fine but you still want to know your real risk of a heart attack, ApoB is the test you should be asking for.
So here is the one sentence answer. ApoB is a direct count of every cholesterol particle in your blood that can lodge in your artery wall and build plaque. LDL cholesterol estimates how much cholesterol those particles are carrying. ApoB counts the particles themselves, and particle count is what actually drives heart disease.
I am a cardiologist and a lipid specialist, and I have spent years watching patients get a falsely reassuring LDL number while their real risk kept climbing. ApoB is the fix for that problem. In 2026 the major guidelines finally caught up to what the science has been saying for two decades. Let me walk you through it in plain English.
Infographic Summary:
What Is ApoB (Apolipoprotein B)?
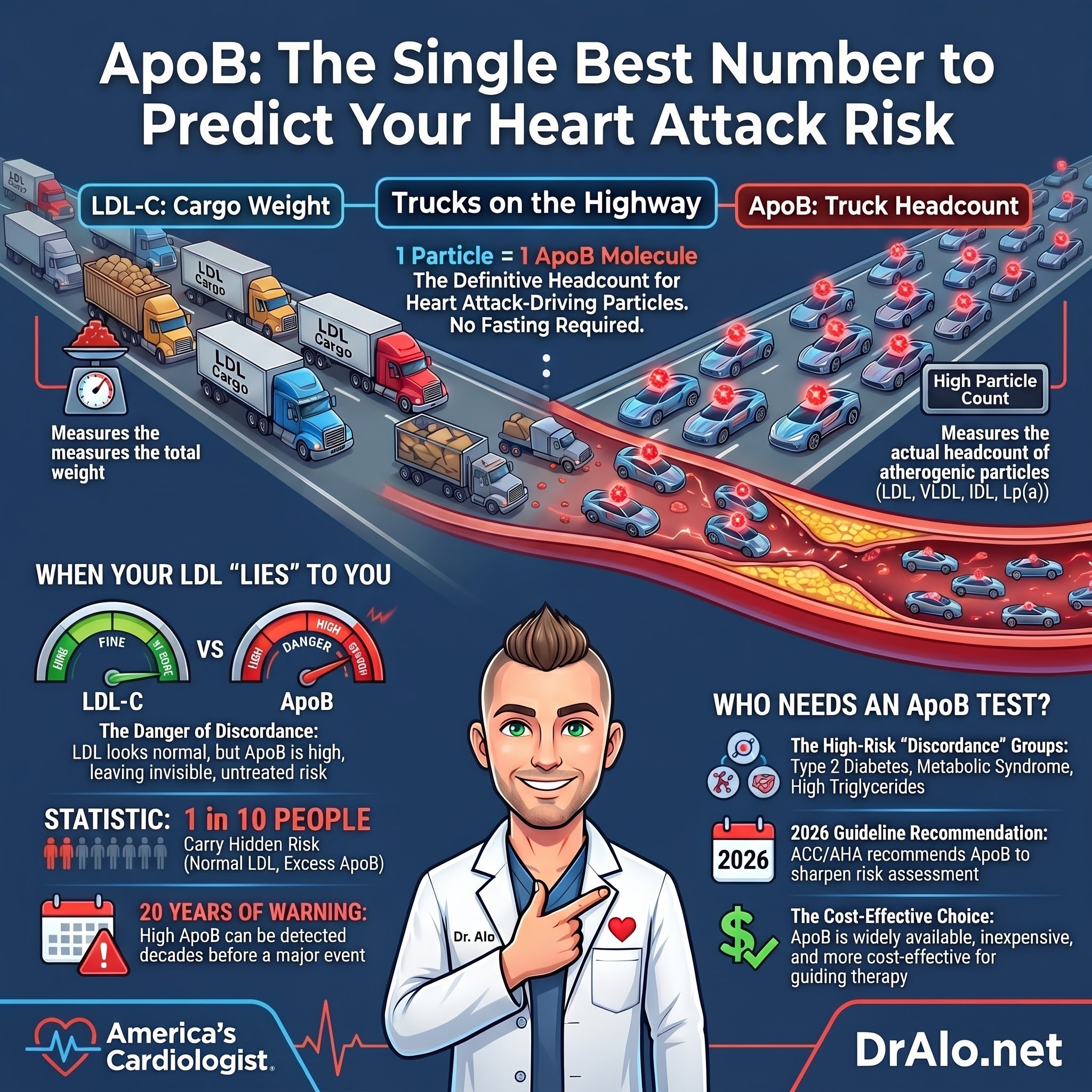
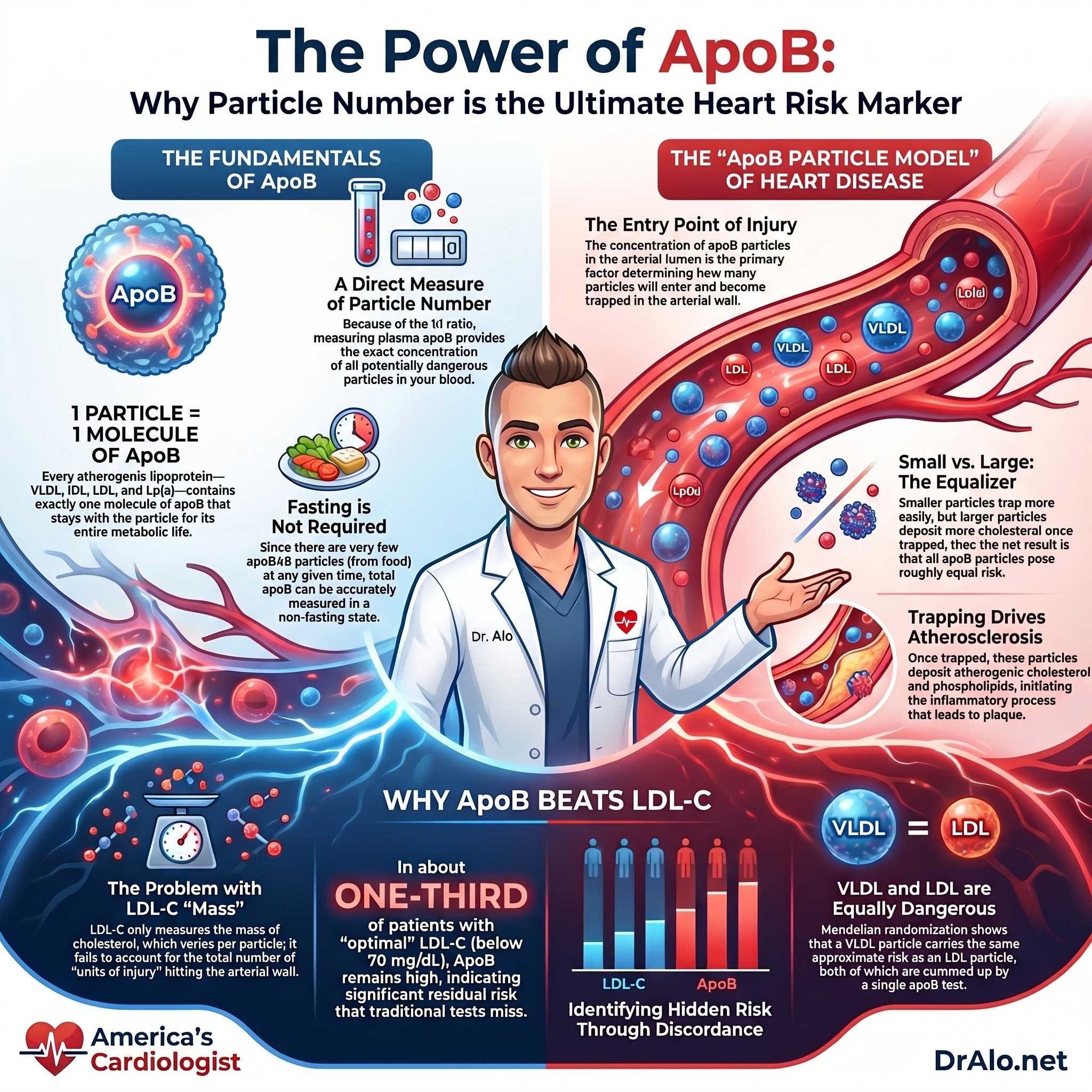
ApoB is a protein, and here is the only fact about it you truly need to remember: there is exactly one ApoB molecule on every single atherogenic particle in your blood. One particle, one ApoB. That includes LDL, VLDL, IDL, and Lp(a). These are the particles that build plaque, and ApoB counts every one of them.
Now compare that to LDL cholesterol. LDL-C measures the cholesterol cargo packed inside your LDL particles. It is a measure of weight, not headcount. ApoB, by contrast, directly quantifies the total number of atherogenic particles floating in your circulation.
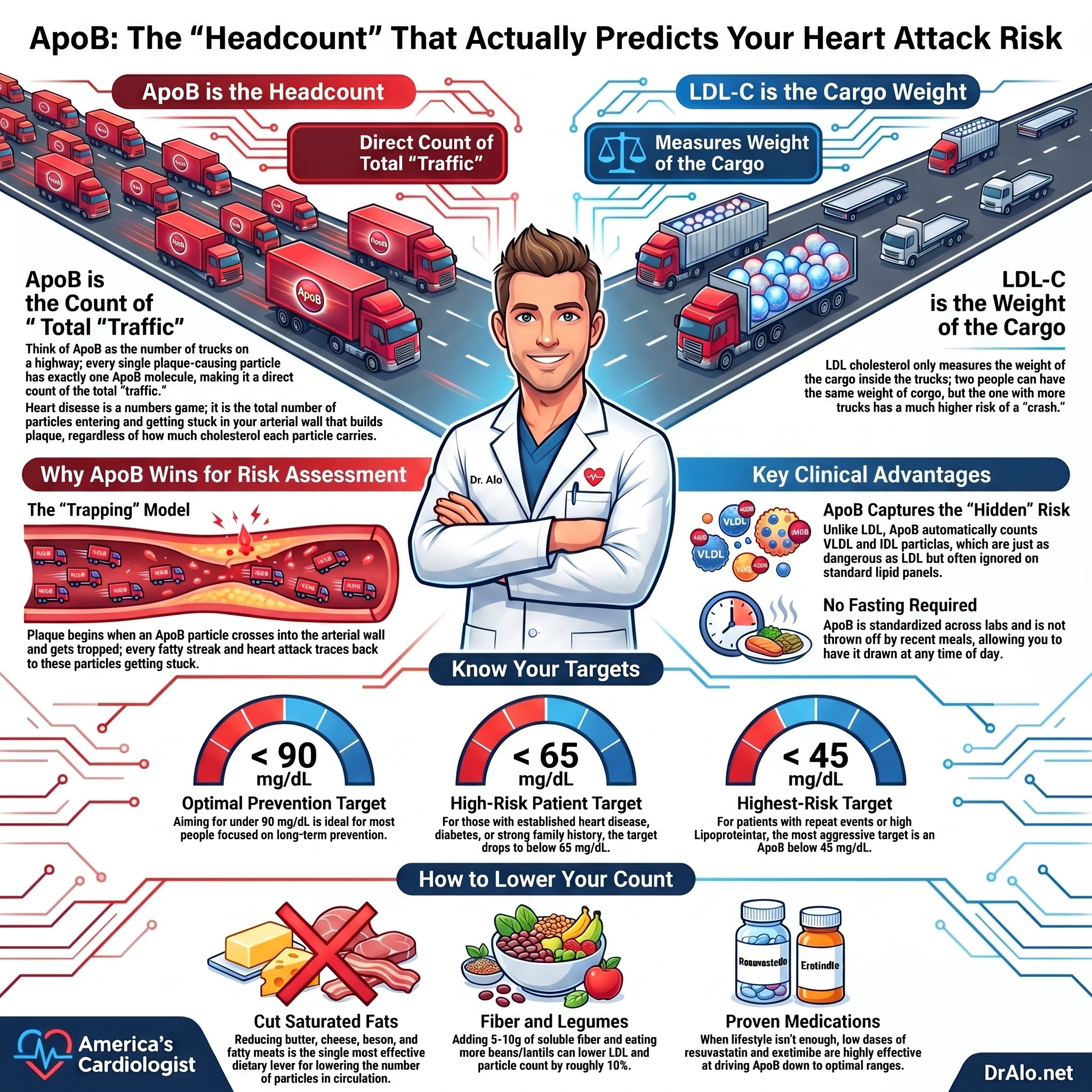
Why does headcount matter more than weight? Because atherosclerosis is a numbers game. It is the number of particles entering and getting stuck in your arterial wall that builds plaque, not how much cholesterol each individual particle happens to be carrying. Two people can have the identical LDL cholesterol while one has far more particles than the other. Same weight on the scale, very different number of trucks on the highway. The person with more trucks has more risk, and ApoB is the only routine test that tells you how many trucks you have.
ApoB vs LDL: What Is the Difference?
This is the question I get more than any other, so let me be direct. ApoB and LDL are not the same thing, and the difference is the whole point.
LDL cholesterol tells you the amount of cholesterol inside one type of particle. ApoB tells you the total number of all the plaque-causing particles you have, LDL and VLDL and IDL and Lp(a) combined. Most of the time the two numbers agree. The problem is the times they do not, because that is exactly when LDL gives you a false sense of safety. We have a name for that mismatch, and I will get to it below.
How Plaque Actually Starts: The Trapping Model
To understand why ApoB wins, you have to understand how a plaque begins. The whole process starts with a single event repeated millions of times: an ApoB particle crosses into your arterial wall and gets trapped there. That trapped particle dumps its cholesterol into the wall, and that is the seed of atherosclerosis. Everything that follows, from the first fatty streak to the unstable plaque that ruptures and causes a heart attack, traces back to ApoB particles getting stuck in the wall.
Here is the key insight. The number of particles that get trapped in the wall is driven mainly by the number of particles in the bloodstream pressing up against it. More particles in the lumen means more particles forced into the wall. Cholesterol cannot enter your artery wall on its own. It can only get in as cargo inside an ApoB particle. So the amount of cholesterol dumped into your wall over a lifetime is governed by particle number, which is exactly what ApoB measures.
Now a fair question: if some particles carry more cholesterol than others, should not the cholesterol-rich ones be more dangerous? The answer is one of the most elegant findings in lipidology, and it explains why ApoB is so powerful. There is a tradeoff that cancels out. Smaller, cholesterol-poor particles slip into the wall more easily and bind more tightly once they are there, so more of them get trapped. Larger, cholesterol-rich particles get trapped less often, but each one deposits more cholesterol when it does. Greater stickiness for the small ones, greater cargo for the big ones. These two effects balance, and the net result is that every ApoB particle carries roughly equal atherogenic risk. That is why counting particles, not weighing their cargo, is the right approach.
Triglycerides, VLDL, and Why ApoB Captures Both
This is where ApoB pulls off something LDL cholesterol simply cannot do. For years we treated LDL as the dangerous particle and triglyceride-rich VLDL as a side issue. The genetic and epidemiologic evidence now shows that a VLDL particle is about as atherogenic as an LDL particle. Same one molecule of ApoB, same basic capacity to lodge in the wall. It's important to note that 95% of apoB particles are LDL particles, hence, VLDL and IDL make up a very small minority of particles.
So why has cholesterol always tracked more closely with heart disease than triglycerides have? Pure arithmetic. In most people, LDL particles outnumber VLDL particles roughly nine to one. There are simply far more LDL trucks on the road.
But in someone with high triglycerides, the VLDL fraction climbs, and the risk climbs with it. ApoB handles this automatically because it counts the LDL particles and the VLDL particles in one number. You do not have to disentangle the so-called atherogenic triad of high triglycerides, low HDL, and small dense LDL. ApoB sums all of the atherogenic risk into a single figure.
This also explains one of the great disappointments in cardiology: fibrates. These drugs slash triglycerides and VLDL, yet they failed to consistently prevent events in trials. Why? Because VLDL particles are a small slice of total ApoB in most people, so lowering them barely moves the total particle count. The lesson holds in the other direction too. A therapy helps your heart to the degree that it lowers your ApoB. That is the unifying rule.
What Is a Normal ApoB Level?
Labs typically flag ApoB above roughly 100 to 130 mg/dL as elevated, but I want to be honest about what those reference ranges actually mean. A lab reference range tells you what is statistically average in the population. It does not tell you what is optimal for your arteries. In a population where heart disease is the leading cause of death, average is not a goal worth aiming for.
Here is how I think about targets in my own practice. For most people focused on prevention, I want ApoB comfortably under 90 mg/dL. For high-risk patients, those with established heart disease, diabetes, or a strong family history, I target an ApoB below 65 mg/dL, alongside an LDL below 55 mg/dL. Lower is better when it comes to the particles that cause plaque. There is no good evidence that driving these particles down causes harm, and decades of evidence that high numbers cause heart attacks.
For the highest risk populations, those with repeat ischemic events or lipoprotein a, we recommend an LDL cholesterol below 40 mg/dL or an apoB below 45 mg/dL.
When LDL-C is below 50 mg/dL the numbers are not very accurate do to the Friedewald equation. It's more important to follow apoB at very low levels.
What Does a High ApoB Mean?
A high ApoB means you have a large number of particles capable of entering your artery wall and seeding plaque. It is a direct readout of atherogenic risk. The higher the number, the more particles pressing against your arterial wall every day, and the faster plaque tends to accumulate.
What causes a high ApoB? The common drivers are genetics, including familial hypercholesterolemia and familial combined hyperlipidemia, along with diet, insulin resistance, type 2 diabetes, and excess weight. Sometimes ApoB is high even when LDL looks acceptable, and that specific situation is the one I worry about most, because it hides from a standard panel.
The ApoB Blood Test: What to Know
The ApoB test is a simple blood draw, and it is one of the most underused tests in cardiology. A few practical points patients ask about constantly.
You do not need to fast for an ApoB test. That is one of its quiet advantages. Unlike a calculated LDL, ApoB is not thrown off by a recent meal, so you can have it drawn at any time of day. It is also standardized across labs and widely available, so you are not chasing some exotic boutique panel. If your physician is ordering a lipid panel anyway, adding ApoB is straightforward, and I will give you language to ask for it below.
Why the 2026 Guidelines Elevated ApoB
The 2026 ACC/AHA Dyslipidemia Guideline recommends ApoB measurement to sharpen ASCVD risk assessment and guide lipid-lowering therapy, especially once your LDL-C and non-HDL-C goals have already been hit. This is a big deal, and it is built on real data.
Here is what convinced them. In primary prevention, when you put atherogenic lipids and ApoB into the same statistical model, only ApoB stays significantly tied to future heart attacks. The adjusted hazard ratio per one standard deviation was 1.27 (95% CI 1.15 to 1.40). When ApoB is in the room, LDL-C loses its independent predictive power.
The guideline also leaned on a concept that trips up a lot of patients and frankly a lot of doctors: discordance.
Discordance: When Your LDL Lies to You
Discordance is when your LDL-C and your ApoB tell you two different stories. Your LDL-C can sit comfortably at goal while your ApoB is still elevated. That gap is dangerous, because it means you have more atherogenic particles than your LDL number suggests, and that residual risk is invisible if you only look at LDL.
Who tends to have this problem? The people I see most often with discordance are patients with established ASCVD, cardiovascular-kidney-metabolic (CKM) syndrome, type 2 diabetes, or triglycerides at or above 150 mg/dL. If that is you, an LDL number alone is simply not good enough.
One practical note: how the lab estimates your LDL matters. When the Martin/Hopkins method is used instead of the older Friedewald equation, discordance between LDL-C and ApoB shrinks considerably. But it does not disappear, and ApoB still settles the question.
ApoB has other advantages too. It is standardized, it is not thrown off by whether you fasted, and it helps diagnose inherited lipid disorders like familial combined hyperlipidemia and familial dysbetalipoproteinemia.
What the ACC/AHA Actually Recommends
Here are the formal recommendations, translated out of guideline-speak:
For adults already on lipid-lowering therapy, particularly those with ASCVD, CKM syndrome, type 2 diabetes, or elevated triglycerides, it is reasonable to measure ApoB to decide whether to intensify treatment once LDL-C and non-HDL-C goals are reached (Class 2a).
For adults not yet on therapy, measuring ApoB may be reasonable to refine ASCVD risk assessment, guide whether to start treatment, and help characterize inherited lipid disorders (Class 2b).
Infographic Summary:
The Evidence Behind ApoB
I'm not asking you to take guidelines on faith. The recommendation rests on observational cohorts, meta-analyses, Mendelian randomization, and post hoc analyses of randomized trials. Let me give you the highlights, because they are genuinely impressive.
The AMORIS cohort. This Swedish study followed 137,100 people for a median of nearly 18 years. Elevated ApoB and the ApoB/apoA-1 ratio were strongly tied to major cardiovascular events across every age group and both sexes. Comparing the top decile to the bottom, the hazard ratio was 1.7 for major events and 2.7 for non-fatal heart attack. The part that should grab your attention: a high ApoB/apoA-1 ratio was detectable roughly 20 years before events happened. Twenty years of warning. That is the case for measuring it early. ApoA-1 is an apoprotein found on HDL particles. So, you are looking at a ratio of atherogenic particles vs non atherogenic particles. This is useful for research but has no clinical applications. There is no need to check this.
The Copenhagen General Population Study. Among 13,015 statin-treated patients, elevated ApoB and non-HDL-C were linked to higher all-cause mortality and heart attack. Elevated LDL-C was not significantly associated with those outcomes. Read that again. In people on statins, LDL-C did not reliably flag who was still at risk, but ApoB did.
The Excess ApoB study. In a primary prevention population, having ApoB above what your LDL-C would predict carried a dose-dependent increase in risk of heart attack, ASCVD, and all-cause mortality. This excess ApoB identified roughly 1 in 10 people who were carrying substantially more risk than their LDL-C alone implied, and it did so across the entire LDL-C spectrum, including in people with low LDL-C. Low LDL does not automatically mean low risk.
The 2026 concordance and discordance analysis. When ApoB and non-HDL-C were both elevated, risk was highest. When they disagreed, each marker added prognostic information the other missed. The practical takeaway is that these measures are most powerful when used together.
The 2012 statin meta-analysis. In statin-treated patients, both ApoB and non-HDL-C outperformed LDL-C for predicting major cardiovascular events, with non-HDL-C showing the strongest association in that particular analysis. The common thread across studies is the same: LDL-C is the weakest of the three.
The Mendelian randomization argument. This is the piece that turned a lot of skeptics, myself included. Researchers used genetics to settle which marker truly drives risk. When you build genetic scores that lower triglycerides versus scores that lower LDL cholesterol, and then normalize both for the same drop in ApoB, the benefit is nearly identical. In other words, it was never really about LDL cholesterol versus triglycerides. It was about ApoB particle number all along. The same approach untangled the puzzle of CETP inhibitor drugs, which lowered LDL-C dramatically but failed to prevent events. The reason was that they barely lowered ApoB. Benefit tracks ApoB, not the cholesterol number.
The treatment-target problem. Here is a finding every patient on a statin should know. In roughly one-third of people who hit an LDL-C below 70 mg/dL, the ApoB was still substantially elevated, signaling residual risk and the potential to benefit from more aggressive therapy. Your LDL can look like a victory while your ApoB is telling you the job is not finished. That is precisely why ApoB is the better gauge of whether your treatment is actually working.
Two Important Exceptions
I told you all ApoB particles are roughly equally atherogenic. There are two exceptions worth knowing, because both are clinically important and both can hide from a standard lipid panel.
The first is type III hyperlipoproteinemia, also called familial dysbetalipoproteinemia. In this disorder, the body accumulates abnormal, intensely cholesterol-loaded remnant particles that do far more damage per particle than usual, sometimes present at 20 to 40 times normal remnant levels. A routine cholesterol panel will not catch it, but the combination of total cholesterol, triglycerides, and ApoB can identify it accurately. This is one more reason I want your ApoB number.
The second is lipoprotein(a), or Lp(a). This is an ApoB particle with an extra protein attached, and elevated Lp(a) independently raises your risk of both heart disease and aortic valve disease. It stays a source of risk even when LDL-C is driven to near-optimal levels with statins or PCSK9 inhibitors. Lp(a) is genetically determined and should be measured at least once in every adult. If you have familial hypercholesterolemia, a high Lp(a) on top of it stacks the risk even higher.
The Honest Counterpoint
I am not in the business of cherry-picking, so here is the study that pushes back. The UK Biobank analysis of 346,686 people found that ApoB, LDL-C, and non-HDL-C had similar hazard ratios per standard deviation for composite cardiovascular events, around 1.20 to 1.23. And once total cholesterol and HDL-C were already in the prediction model, adding ApoB or LDL-C barely moved the needle on discrimination.
What this tells me is that for broad, population-level statistical prediction, the extra discriminative value of ApoB may be modest. But population-level discrimination and individual clinical decision-making are not the same thing. For the patient in front of me with diabetes and high triglycerides, ApoB still resolves the discordance question that LDL-C cannot. I want you to know both sides.
Is the ApoB Test Worth It? The Cost Question
A frequent objection is that ApoB is exotic or expensive. It is neither. The AACC working group that reviewed 25 clinical studies endorsed ApoB precisely because it is widely available, scalable, standardized, and relatively cheap, while performing as a stronger risk factor than LDL-C.
A 2026 cost-effectiveness simulation went further. Using ApoB goals to guide therapy intensification was cost-effective compared with LDL-C and non-HDL-C goals. At the $120,000 per QALY threshold, ApoB-guided therapy had a 65% probability of being the optimal strategy, versus just 10% for LDL-C-guided therapy. As the authors put it, ApoB is a more accurate marker of ASCVD risk than LDL-C or non-HDL-C across observational studies, Mendelian randomization, and randomized trials.
The National Lipid Association reached the same conclusion in its 2024 expert consensus: ApoB is superior to LDL-C for risk assessment both before and during treatment, and when the two disagree, your true risk tracks with ApoB. The NLA specifically called for better access and reimbursement for the test.
Infographic Summary:
How to Lower Your ApoB
If your ApoB is high, the good news is that it is very treatable. The same tools that lower LDL lower ApoB, because you are removing particles from circulation. I will write a full deep-dive on this, but here is the honest short version.
Lifestyle moves the needle. Cutting saturated fat, losing excess weight, getting regular exercise, and improving insulin sensitivity all reduce particle number. For many people, lifestyle alone gets ApoB into a much better range. When it is not enough, the medications that work are the ones with decades of outcome data behind them: statins first, then ezetimibe, then PCSK9 inhibitors for those who need more. These drugs lower particle count, and lower particle count is what prevents heart attacks.
Let me also say what does not work, because the wellness industry will happily sell you the difference. Red yeast, berberine, nattokinase, and a cabinet full of supplements are not a substitute for therapies proven to reduce events. If a product promises to clean your arteries without touching your particle number, it is marketing, not medicine. Lower your ApoB with things that are proven to work.
If that doesn't get your apoB down, we can use medications. Two very old, cheap medications can get most people's apoB down to target levels. This would include rosuvastatin and ezetimibe. That's what I take. I take 10mg of each, and that has kept my LDL and apoB in the 40mg/dL range.
How to Lower Your ApoB Naturally
If your ApoB is high, the good news is that it responds well to what you eat. Remember what ApoB measures: the total number of atherogenic particles in your blood. Anything that reduces the number of LDL and VLDL particles in circulation lowers your ApoB. Diet does exactly that. Let me give you the moves that actually work, in order of how much they matter.
Cut Saturated Fat: The Single Biggest Lever
If you do only one thing, do this. Reducing saturated fat is the single most effective dietary change for lowering the particles that drive heart disease. Saturated fats are the ones that are solid at room temperature: butter, cheese, bacon, lard, tallow, ghee, coconut oil, the fat on a steak, and chicken skin. Trans fats from partially hydrogenated oils belong in the same bucket and are even worse.
Here is the mechanism, because it matters. Saturated fat does two harmful things at once. It increases cholesterol synthesis, and it reduces the number of LDL receptors your liver uses to pull LDL particles out of your blood. Fewer receptors means particles stay in circulation longer, so your ApoB climbs. Cut the saturated fat and you flip both switches in the right direction. Saturated fat also increases inflammation.
Swap In Healthy Fats, Do Not Just Remove Fat
The goal is not to go fat-free. It is to replace saturated fat with monounsaturated and polyunsaturated fats. When you trade butter for olive oil, or fatty meat for nuts and avocado, the particle-lowering effect is far larger than just cutting fat alone. These fats lower LDL particle number and have been tied to fewer cardiovascular events and lower mortality, and the benefit is strongest precisely when they replace saturated fat rather than just adding to your plate. This is also why the Mediterranean diet works so well. In a systematic review of 13 randomized trials it lowered LDL by an average of 18.5 mg/dL, and that drop reflects fewer atherogenic particles, which is a lower ApoB.
Add Soluble Fiber
Fiber is the supporting actor here, not the star, but it adds up, and the little things compound. Soluble fiber binds cholesterol in your gut and carries it out before it can be absorbed, which nudges your particle number down. A review of 11 studies published in JAMA found that adding 5 to 10 grams of soluble fiber per day lowered LDL by about 3 to 5 percent, with the bonus of better blood sugar and insulin sensitivity. You get soluble fiber from oats, barley, beans, apples, and pears. If you cannot get enough from food, plain psyllium husk, the active ingredient in Metamucil, is cheap, proven, and does the job. That is not a supplement gimmick, it is just fiber.
Eat More Beans and Legumes
Beans deserve their own line because the data is strong. Regularly eating beans and legumes, including lentils, chickpeas, kidney beans, and soybeans, has been shown to lower LDL by roughly 10 percent. They are loaded with soluble fiber, they crowd saturated-fat-heavy foods off your plate, and they carry their own cardioprotective benefits. Very few single foods move your particle number this reliably.
The Honest Limit of Diet
Now the part the wellness influencers will not tell you. Your cholesterol is largely genetic, and for many people diet alone will not get ApoB all the way to target. That is not a personal failure, and it is not a reason to quit, because every bit of particle lowering reduces your lifetime risk. But if you have familial hypercholesterolemia, established heart disease, or an ApoB that stays elevated despite doing all of this well, you will likely need medication too. Diet and drugs are not rivals. They are partners, and they share one goal: fewer particles, lower ApoB. And no, a cabinet of supplements is not the answer. If a product promises to clean out your arteries without lowering your particle number, it is selling you marketing, not medicine.
Frequently Asked Questions About ApoB
What is ApoB in a blood test?
ApoB measures the total number of atherogenic particles in your blood, the LDL, VLDL, IDL, and Lp(a) particles that cause plaque. There is one ApoB protein on each of these particles, so the number is a direct headcount of the particles that drive heart disease.
Is ApoB the same as LDL?
No. LDL cholesterol measures the cholesterol carried inside your LDL particles. ApoB counts all of your plaque-causing particles, not just LDL, and it counts them rather than weighing their cargo. They usually agree, but when they disagree your true risk tracks with ApoB.
What is a normal ApoB level?
Labs often flag ApoB above roughly 100 to 130 mg/dL as elevated, but those are population averages, not optimal targets. For prevention I want most people under 90 mg/dL, and for high-risk patients I target below 65 mg/dL.
What does a high ApoB mean?
It means you have a large number of particles capable of entering your artery wall and building plaque. The higher the number, the higher your risk of a future heart attack or stroke.
What causes high ApoB?
The usual drivers are genetics (including familial hypercholesterolemia and familial combined hyperlipidemia), diet high in saturated fat, insulin resistance, type 2 diabetes, and excess weight.
How do you lower ApoB?
Lifestyle changes such as reducing saturated fat, losing weight, and exercising lower particle number, and when those are not enough, statins, ezetimibe, and PCSK9 inhibitors are the proven medications. Supplements marketed for cholesterol are not a substitute for therapies with outcome data.
Do you have to fast for an ApoB test?
No. ApoB does not require fasting, which is one of its advantages over a calculated LDL. You can have it drawn at any time of day.
Which is more important, Lp(a) or ApoB?
They answer different questions. ApoB tells you your overall atherogenic particle burden, which you can lower with lifestyle and medication. Lp(a) is a specific, largely genetic particle type that adds independent risk and should be measured at least once in every adult. You want to know both.
Bottom Line on ApoB
ApoB measures the thing that actually causes heart disease: the total number of particles capable of entering and lodging in your arterial wall. LDL-C remains a useful primary treatment target, and I still track it. But ApoB gives you additive and sometimes superior information, especially if you have cardiometabolic disease, you are on a statin, or your triglycerides are up and your LDL-C is quietly underestimating your real burden.
Here is my advice. The next time you get a lipid panel, ask for an ApoB. If your doctor tells you it is unnecessary because your LDL is fine, gently push back. Your LDL can be fine and your ApoB can still be telling you that you are building plaque. I would rather you know.
For high-risk patients, I target an ApoB below 65 mg/dL, alongside an LDL below 55 mg/dL. We will cover how to get there with lifestyle and medication in a future post. For now, get the number.
References
1. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Blumenthal RS, Morris PB, Gaudino M, et al. Journal of the American College of Cardiology. 2026. https://doi.org/10.1016/j.jacc.2025.11.016
2. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. Sniderman AD, Thanassoulis G, Glavinovic T, et al. JAMA Cardiology. 2019;4(12):1287-1295. https://doi.org/10.1001/jamacardio.2019.3780
3. Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk. Glavinovic T, Thanassoulis G, de Graaf J, et al. Journal of the American Heart Association. 2022;11(20):e025858. https://doi.org/10.1161/JAHA.122.025858
4. Apolipoprotein B Compared With Low-Density Lipoprotein Cholesterol in the Atherosclerotic Cardiovascular Diseases Risk Assessment. Galimberti F, Casula M, Olmastroni E. Pharmacological Research. 2023;195:106873. https://doi.org/10.1016/j.phrs.2023.106873
5. Long-Term Risk of a Major Cardiovascular Event by apoB, apoA-1, and the apoB/apoA-1 Ratio: Experience From the Swedish AMORIS Cohort. Walldius G, de Faire U, Alfredsson L, et al. PLoS Medicine. 2021;18(12):e1003853. https://doi.org/10.1371/journal.pmed.1003853
6. Association of LDL Cholesterol, Non-HDL Cholesterol, and Apolipoprotein B Levels With Risk of Cardiovascular Events Among Patients Treated With Statins: A Meta-analysis. Boekholdt SM, Arsenault BJ, Mora S, et al. JAMA. 2012;307(12):1302-1309. https://doi.org/10.1001/jama.2012.366
7. Apolipoprotein B and Non-HDL Cholesterol Better Reflect Residual Risk Than LDL Cholesterol in Statin-Treated Patients. Johannesen CDL, Mortensen MB, Langsted A, Nordestgaard BG. Journal of the American College of Cardiology. 2021;77(11):1439-1450. https://doi.org/10.1016/j.jacc.2021.01.027
8. Excess Apolipoprotein B and Cardiovascular Risk in Women and Men. Johannesen CDL, Langsted A, Nordestgaard BG, Mortensen MB. Journal of the American College of Cardiology. 2024;83(23):2262-2273. https://doi.org/10.1016/j.jacc.2024.03.423
9. Non-HDL Cholesterol and Apolipoprotein B Measures and Risk of Atherosclerotic Cardiovascular Disease. Johannesen CDL, Langsted A, Nordestgaard BG, Mortensen MB. JAMA Cardiology. 2026. https://doi.org/10.1001/jamacardio.2026.0898
10. Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease. Welsh C, Celis-Morales CA, Brown R, et al. Circulation. 2019;140(7):542-552. https://doi.org/10.1161/CIRCULATIONAHA.119.041149
11. Association of Apolipoprotein B and Nuclear Magnetic Resonance Spectroscopy-Derived LDL Particle Number With Outcomes in 25 Clinical Studies. Cole TG, Contois JH, Csako G, et al. Clinical Chemistry. 2013;59(5):752-770. https://doi.org/10.1373/clinchem.2012.196733
12. Cost-Effectiveness of ApoB, Non-HDL-C, and LDL-C Goals for Primary Prevention Lipid-Lowering Therapy. Luebbe S, Sniderman AD, Moran AE, Wilkins JT, Kohli-Lynch CN. JAMA. 2026. https://doi.org/10.1001/jama.2026.2986
13. Role of Apolipoprotein B in the Clinical Management of Cardiovascular Risk in Adults: An Expert Clinical Consensus From the National Lipid Association. Soffer DE, Marston NA, Maki KC, et al. Journal of Clinical Lipidology. 2024;18(5):e647-e663. https://doi.org/10.1016/j.jacl.2024.08.013
14. Saturated fat raises LDL by increasing cholesterol synthesis and reducing LDL receptor activity. https://pubmed.ncbi.nlm.nih.gov/32428300/
15. Mediterranean diet and LDL reduction: systematic review of 13 randomized controlled trials. https://www.sciencedirect.com/science/article/pii/S266614972200038X
16. Replacing saturated fat with monounsaturated and polyunsaturated fats and cardiovascular outcomes. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6517012/ and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6513455/
17. Soluble fiber and LDL cholesterol: review of 11 studies. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5413815/ and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6566984/
18. Beans and legumes and LDL cholesterol reduction. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7915747/
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















