

Debunking Very Low Cholesterol Myths
May 14, 2026
Is Very Low LDL Cholesterol Dangerous?
10 Common Fears, Debunked by a Cardiologist
Every week, I see patients who are reluctant to take their statin. Some have stopped their PCSK9 inhibitor. Others are terrified that driving their LDL cholesterol too low will melt their brain, cause cancer, destroy their hormones, or strip them of their muscle. These fears are everywhere online. Wellness influencers and supplement gurus are having a field day with them.
Let me be direct with you: nearly every major safety concern about very low LDL cholesterol has been studied, tested in rigorous randomized trials, and overwhelmingly not supported by the evidence. This does not mean there are zero risks. There are two real ones, and I will cover those honestly. But the list of confirmed dangers is far shorter than social media would have you believe.
A fresh narrative review published in Atherosclerosis in 2026, authored by lipid specialists from across Latin America, Turkey, and Greece and aligned with the 2025 ESC/EAS focused update, systematically addressed the ten most common fears surrounding very low and ultra-low LDL-C levels. I am going to walk you through each one, in plain language, the way I explain it to my own patients.
The science on this is clear: achieving very low LDL cholesterol provides proportional cardiovascular protection, and the vast majority of feared side effects are not supported by randomized clinical trial data.
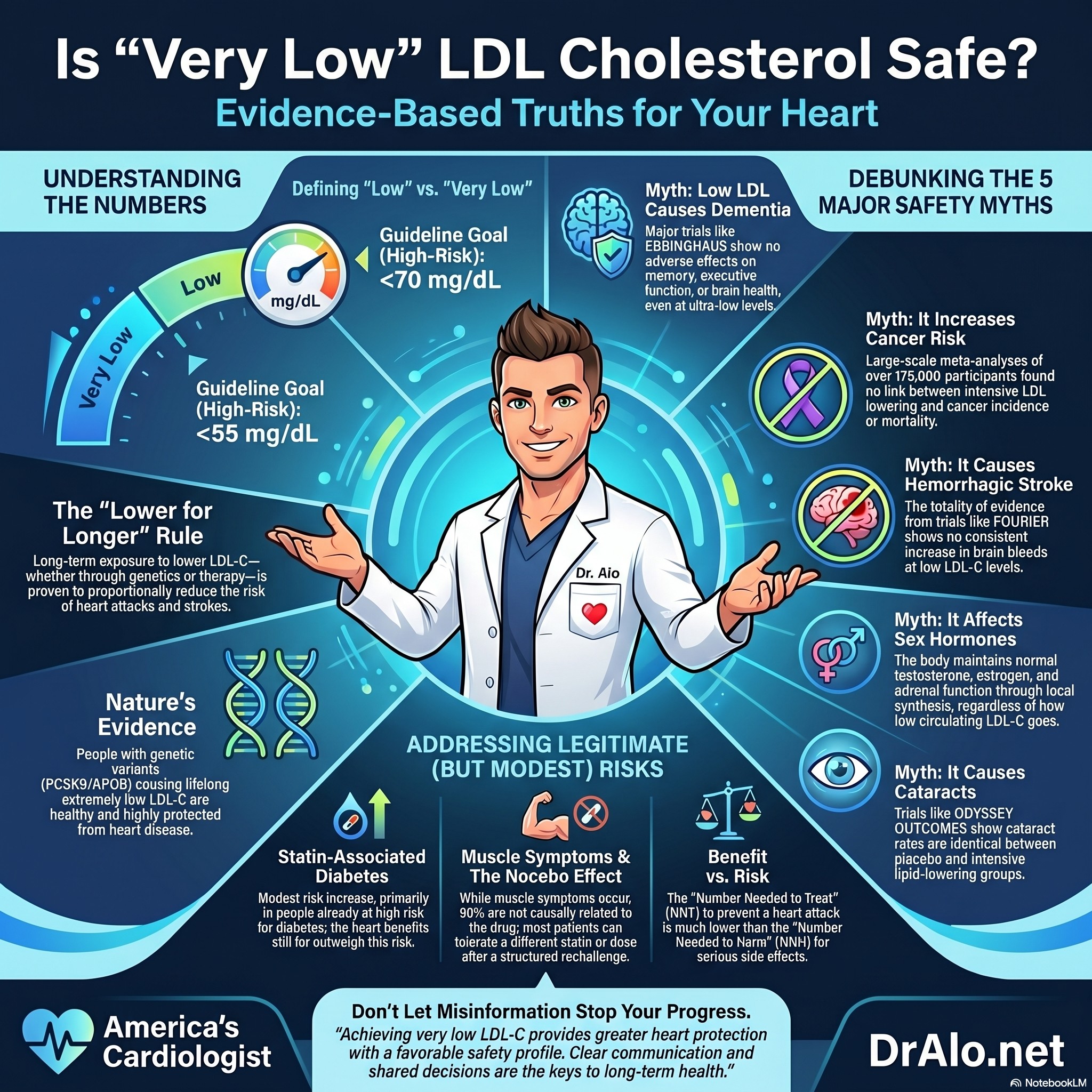
Very Low LDL Myths Infographic Summary:
First: What Do We Actually Mean by "Very Low" LDL?
Before diving in, let me set the table on terminology, because this matters for understanding the evidence:
- Low LDL-C: below 70 mg/dL
- Very low LDL-C: below 55 mg/dL (the current ESC/EAS 2025 goal for very high-risk patients)
- Extremely low LDL-C: below 40 mg/dL (seen in some trial participants, not a recommended target)
- Ultra-low LDL-C: below 25 mg/dL (seen in PCSK9 inhibitor trials, not a recommended target)
These are not arbitrary numbers. They reflect decades of trial data and increasingly aggressive guideline targets as we have learned that lower LDL, sustained over time, translates to fewer heart attacks, strokes, and cardiovascular deaths. The 2025 ESC/EAS focused update doubles down on this. So does the emerging 2026 ACC/AHA framework.
Now, let us go through the ten fears one by one.
Fear #1: Will Very Low LDL Cause Dementia or Cognitive Decline?
This is arguably the most common patient concern I hear. People are afraid that lowering LDL too aggressively will impair brain function. The mechanism people imagine is that cholesterol is needed for the brain, so lower must mean worse.
Here is the biological reality: LDL particles do not cross the blood-brain barrier. Brain cholesterol is manufactured locally by astrocytes and oligodendrocytes and transported within the brain by apolipoprotein E-containing lipoproteins that are produced inside the brain itself. Your plasma LDL-C level has essentially no bearing on what your brain has access to for its cholesterol needs.
What does the randomized evidence say? A meta-analysis of 25 randomized controlled trials covering nearly 47,000 participants found no difference between statin and placebo groups in cognitive events or cognitive test performance. The EBBINGHAUS study, which was embedded within the landmark FOURIER trial, specifically evaluated patients achieving LDL-C below 25 mg/dL on evolocumab and found no adverse effects on executive function, memory, or overall cognitive performance. The 2026 CTT Collaboration individual-participant meta-analysis of large double-blind statin trials found no excess risk of cognitive impairment from statin therapy.
There is a Mendelian randomization signal suggesting that genetically proxied HMGCR inhibition (the statin pathway) and NPC1L1 inhibition (the ezetimibe pathway) may modestly affect cognitive performance. But critically, these genetic models reflect lifelong pathway modulation from birth, not the clinical reality of starting a statin in your 50s or 60s. And they have not translated into any cognitive harm signal in actual randomized trials.
One very large updated meta-analysis of observational studies covering over 7 million individuals found that statin use was actually associated with a lower risk of dementia, including Alzheimer's disease and vascular dementia, with a hazard ratio of 0.86.
The brain makes its own cholesterol and does not rely on your plasma LDL. Decades of randomized trial data, including at ultra-low LDL levels, show no cognitive harm from aggressive lipid lowering.
I have an entire article on Statins and Dementia.
Fear #2: Does Low LDL Increase Cancer Risk?
This fear originated in epidemiological observations from the late 1990s noting an inverse association between cholesterol levels and cancer. In other words, people with lower cholesterol seemed to have higher cancer rates. That sounds alarming. But here is the problem: this is a textbook case of reverse causality.
Cancer causes cholesterol to drop. Occult malignancy, through inflammation, cachexia, and altered metabolism, lowers circulating cholesterol before the cancer is ever diagnosed. Early studies did not account for this adequately.
The gold standard evidence comes from the Cholesterol Treatment Trialists Collaboration, which conducted pre-specified analyses of cancer incidence and cancer mortality across more than 175,000 participants from 27 randomized trials. Statin therapy was not associated with any increase in incident cancer or cancer mortality, across 23 site-specific cancers, across different treatment durations, and across every achieved LDL subgroup studied.
Some preclinical and observational data hint at possible anti-tumor effects of statins. Those findings are biologically interesting but not proven. Current evidence does not support using statins as cancer prevention agents outside of clinical trials. The one exception: statins may be considered in patients at high or very high risk of chemotherapy-related cardiovascular toxicity, specifically to reduce the risk of anthracycline-induced cardiac dysfunction, as a Class IIa recommendation in the 2025 ESC/EAS guidelines.
Low LDL does not cause cancer. Early data suggesting a link were driven by reverse causality. The randomized evidence is clear and reassuring.
I have an entire article on how Statins Reduce Cancer.
Fear #3: Will Low LDL Give Me Cataracts?
This one comes from early animal studies, specifically dogs and rats exposed to very high doses of statins, that showed lens opacities. Alarming in the lab, irrelevant in clinical practice.
In the ODYSSEY OUTCOMES trial, which randomized nearly 19,000 patients with recent acute coronary syndrome to alirocumab versus placebo, cataracts were a pre-specified outcome. The results: cataracts occurred in 1.3% of the alirocumab group and 1.4% of the placebo group, with a hazard ratio of 0.94. No signal.
A meta-analysis of 10 randomized controlled trials covering 38,427 patients achieving LDL-C below 40 mg/dL found no significant increase in cataract risk compared to control groups with higher LDL-C levels. The odds ratio was 1.28, and the confidence interval crossed 1.0 handily, indicating a non-significant and non-causal association.
Animal studies do not translate here. Human randomized trials, including at very low LDL levels, show no meaningful increase in cataract risk.
Fear #4: Will Lowering LDL Wreck My Hormones or Cause Sexual Dysfunction?
This concern makes intuitive sense to people because cholesterol is the raw material for sex hormones like testosterone and estrogen. Surely driving LDL very low would reduce hormone production, right?
Wrong, and here is why.
Steroidogenic tissues, meaning the adrenal glands, ovaries, and testes, get the vast majority of their cholesterol from two sources: de novo synthesis (making it from scratch internally) and selective uptake of HDL cholesteryl esters via the SR-BI receptor. LDL particle uptake through the classic clathrin-coated pathway contributes approximately 2% in the testes and up to 19% in the adrenal glands. That is a minor contribution, and the body compensates easily.
Genetic proof comes from rare cases of complete PCSK9 deficiency. One of the first documented cases was a healthy, fertile, physically active 40-year-old woman with lifelong LDL-C levels between 14 and 29 mg/dL due to total absence of PCSK9. Normal hormones. Normal sexual development. Normal liver and kidney function. A subsequent case report described a 21-year-old woman homozygous for a PCSK9 loss-of-function variant with an LDL-C of 16 mg/dL and no adverse effects including normal sexual development.
In the DESCARTES trial evaluating evolocumab, gonadal hormone levels remained unchanged despite massive LDL-C reductions. In male patients, testosterone was stable from baseline through the entire follow-up. The 2026 CTT Collaboration meta-analysis of blinded statin trials found no excess risk of erectile or sexual dysfunction.
Your steroidogenic tissues make their own cholesterol and do not depend on your plasma LDL. The evidence from genetic models and clinical trials is consistent: low LDL does not impair hormonal function.
Fear #5: Does Lowering LDL Actually Reduce Cardiovascular Events?
Yes. Unambiguously, emphatically yes. This is not even a close call in the evidence.
I include this because I actually encounter patients who have been told by wellness influencers or online communities that the LDL-cardiovascular disease connection is a pharmaceutical industry fabrication. This is demonstrably false, and it puts people in real danger.
The relationship between LDL-C reduction and MACE reduction is continuous and proportional. There is no lower threshold below which further LDL lowering stops providing benefit. This is supported by Mendelian randomization data, observational epidemiology, and randomized controlled trial meta-analyses covering hundreds of thousands of patients.
In the FOURIER trial, patients achieving LDL-C below 10 mg/dL in pre-specified analyses showed continued cardiovascular risk reduction without any excess of serious adverse events. The FOURIER open-label extension, with follow-up extending to 7 years on evolocumab, demonstrated reductions in cardiovascular mortality and no new safety signals. This is what a legacy effect looks like.
A 2016 Danish nationwide cohort study drove home the real-world stakes. Among over 674,000 individuals, those who stopped statins early after exposure to negative media coverage had a 26% higher risk of myocardial infarction and an 18% higher risk of cardiovascular death compared with those who continued treatment. Misinformation literally kills people.
Lower LDL, sustained over time, means fewer heart attacks, fewer strokes, and fewer cardiovascular deaths. The evidence for this is among the most robust in all of medicine. Stopping your therapy based on social media fear is not a neutral decision.
I have multiple articles showing that lowering LDL cholesterol reduces cardiovascular risk and mortality. Another article on LDL lowering CV risk.
Fear #6: Is Lipid Lowering Less Important in Women?
This misconception is more common among clinicians than among patients, and it contributes to a real and documented problem: women are systematically undertreated for dyslipidemia. They are less likely to receive high-intensity statins, less likely to have therapy intensified, and more likely to have their cardiovascular risk underestimated.
The evidence does not support any clinically meaningful sex-specific difference in the cardiovascular benefit of LDL lowering. Major trial programs have consistently shown that lipid-lowering therapies reduce cardiovascular events to a similar extent in women and men.
On the topic of reproductive safety: a 2026 Norwegian nationwide study found that first-trimester statin exposure was not associated with congenital malformations, including major or cardiac birth defects. There is also no evidence that lipid-lowering therapy adversely affects female fertility or long-term reproductive health.
Cardiovascular disease is the leading killer of women worldwide. LDL-C is atherogenic in women just as it is in men. The treatment approach should be equally aggressive in appropriately selected patients of both sexes.
Fear #7: Will My Statin Give Me Diabetes?
I am going to be straight with you here, because this is one of the two legitimate safety concerns in this entire discussion.
Statins do modestly increase blood glucose, increase HbA1c by small amounts on average, and increase the incidence of new-onset diabetes. This is real. The 2026 CTT individual-participant meta-analysis quantified it clearly: low or moderate-intensity statin therapy increases new-onset diabetes by approximately 10%, while high-intensity statin therapy increases it by approximately 36% relative to placebo and about 10% relative to lower-intensity regimens.
But here is what those relative numbers obscure. The absolute excess risk is small, and the absolute cardiovascular benefit in appropriately selected patients is several-fold larger. A collaborative meta-analysis by Sattar et al. found approximately one additional diabetes case per 225 patients treated over four years. Importantly, 62 to 67% of excess diabetes cases on statins occur in individuals who were already at the diagnostic threshold at baseline. Statins are not creating diabetes out of thin air; they are nudging borderline individuals over the line, often by a year or two.
The CARDS trial showed that atorvastatin 10 mg in diabetic patients increased HbA1c by a mean of just 0.14%, a clinically trivial amount, with no attenuation of cardiovascular protection.
Here is what separates statins from other LDL-lowering agents on this point: ezetimibe, in the IMPROVE-IT trial, did not increase new-onset diabetes. PCSK9 inhibitors in large randomized outcome trials, including FOURIER and ODYSSEY, have not demonstrated clinically meaningful excess diabetes risk even at ultra-low achieved LDL levels. The diabetes signal appears to be pathway-specific to HMGCR inhibition, not a consequence of LDL lowering itself.
My clinical approach: I communicate the diabetes risk honestly, in absolute terms. I emphasize lifestyle interventions, particularly weight management and physical activity, to mitigate it. And I make sure the patient understands that for someone at meaningful cardiovascular risk, refusing a statin over a small diabetes risk is usually not the safer choice.
Statin-associated diabetes is real but modest in absolute terms, concentrated in those already near the diagnostic threshold, and outweighed by cardiovascular benefit in appropriately selected patients. PCSK9 inhibitors have not shown this risk.
Fear #8: Will Low LDL Cause a Brain Bleed?
This concern was largely fueled by a signal in the SPARCL trial, where atorvastatin appeared to be associated with a numerical increase in intracerebral hemorrhage, and by some observational data suggesting an inverse relationship between LDL-C and hemorrhagic stroke.
Here is what the totality of evidence actually shows.
In SPARCL, post-hoc analyses identified that male sex, older age, uncontrolled hypertension, and a history of hemorrhagic stroke were the key drivers of risk, not achieved LDL-C levels. The LDL level itself was not a predictor of hemorrhage within the trial. In the Treat Stroke to Target trial, targeting a lower LDL (mean achieved around 65 mg/dL) versus a higher LDL (around 96 mg/dL) did not produce a statistically significant increase in intracerebral hemorrhage events.
A large Danish nationwide registry covering more than 55,000 patients with prior ischemic stroke found that statin use was associated with an approximately 50% lower risk of intracerebral hemorrhage compared with non-use, with no increase in recurrent hemorrhage among patients with prior hemorrhage history.
A meta-analysis covering both observational studies (355,591 participants) and randomized controlled trials (165,988 participants) found no increased risk of hemorrhagic stroke in individuals achieving LDL below 70 mg/dL, regardless of the lipid-lowering strategy used.
In FOURIER, treatment with evolocumab achieving LDL below 30 mg/dL, and in exploratory analyses below 20 mg/dL, was not associated with increased intracerebral hemorrhage.
There is one observational study from the Women's Health Study showing a higher relative risk of hemorrhagic stroke in women with LDL below 70 mg/dL, but the absolute event rates were extremely low (approximately 0.8% versus 0.4%), and residual confounding cannot be excluded. It should be interpreted cautiously within the full evidence context.
The weight of evidence, across meta-analyses, large registries, and randomized trials including at ultra-low LDL levels, does not support a causal link between low LDL and intracerebral hemorrhage. Hypertension control matters far more for brain bleed risk than LDL level.
Fear #9: Is Aggressive LDL Lowering Dangerous or Pointless in Older Adults?
I hear this one constantly, including from clinicians. The assumption is that once someone is 70 or 75, statins are either risky or no longer worth it. Some of this comes from observational data showing U-shaped associations between LDL and mortality in older populations, with low LDL appearing to correlate with higher mortality.
Here is the problem with that observational data: frailty, advanced illness, cancer, and malnutrition all lower LDL independently and also increase mortality. These confounders are nearly impossible to fully adjust for. This is not a causal effect of low cholesterol; it is reverse causality and confounding, the same issues that plagued early cancer-LDL studies.
The randomized evidence tells a different story. In the PROSPER trial, enrolling adults aged 70 to 82 years, pravastatin significantly reduced coronary events without adverse effects on cognition. In the SAGE trial, intensive statin therapy with atorvastatin 80 mg was superior to moderate-intensity therapy in reducing ischemic burden in patients over age 65, without excess safety concerns.
A large Danish nationwide cohort in individuals aged 70 and older without prior ASCVD found that each 1 mmol/L reduction in LDL-C with lipid-lowering therapy was associated with a 23% lower risk of major vascular events. That effect size is comparable to what is seen in younger individuals.
More than 80% of ASCVD-related deaths occur after the age of 65. Abandoning lipid lowering precisely in the demographic bearing the highest absolute cardiovascular risk is a strategy that needs very strong justification.
That said, I do individualize in adults aged 75 and older, particularly in primary prevention. Frailty, polypharmacy, life expectancy, patient preferences, and competing risks all factor in. The ongoing STAREE and PREVENTABLE trials are designed to address this evidence gap more definitively, and I am watching them closely.
Cardiovascular disease kills mostly older adults. The evidence supports statin therapy through at least age 75, particularly in secondary prevention. Age alone is not a reason to withhold effective therapy.
Fear #10: Will My Statin Destroy My Muscles?
This is the second legitimate safety concern, and the most common reason patients stop their statin prematurely. Muscle symptoms, including myalgia, cramps, and nonspecific limb discomfort, are real. But their frequency and severity are often dramatically overstated, and the nocebo effect is a significant contributor.
The CTT Collaboration's individual-participant data meta-analysis from large double-blind randomized trials covering over 150,000 participants found that statin therapy was associated with approximately a 3% relative increase in first reports of muscle symptoms. That is a real signal. It corresponds to an absolute excess of about 11 events per 1,000 person-years. Crucially, more than 90% of muscle symptom reports in statin-treated patients were not causally attributable to the statin when evaluated rigorously in blinded conditions.
Serious muscle injury, meaning myopathy and rhabdomyolysis, is rare. The nocebo effect, where patients experience symptoms because they expect to, is substantial in open-label and observational settings.
Here is the most important clinical point on this topic: most patients who report muscle symptoms on statins can and do tolerate statin therapy on structured rechallenge. A systematic review and meta-analysis confirmed that most individuals with prior statin-associated muscle symptoms successfully resumed treatment when rechallenged with a different statin, a lower dose, or an alternative dosing schedule.
PCSK9 inhibitors have not been associated with increased muscle symptoms or toxicity in large randomized trials, even in patients achieving LDL-C well below 30 mg/dL. This reinforces the conclusion that muscle symptoms are drug-specific to statins (and even then are often not causally driven), not a consequence of low LDL itself.
Muscle symptoms on statins are real but mostly not causally driven by statins in blinded trials. Serious muscle injury is rare. Most patients can be successfully rechallenged. PCSK9 inhibitors carry no muscle toxicity signal even at ultra-low LDL levels.
The Two Real Risks vs. The Myths: A Quick Reference
|
Concern |
Evidence Status |
Bottom Line |
|
Cognitive decline / dementia |
NOT supported by RCTs or meta-analyses |
Brain makes its own cholesterol; no harm shown even at ultra-low LDL |
|
Cancer risk |
NOT supported by randomized data |
Reverse causality explained early signals; CTT shows no cancer association |
|
Cataracts |
NOT supported in humans |
Animal signals did not translate; ODYSSEY OUTCOMES shows no difference |
|
Hormone disruption / sexual dysfunction |
NOT supported by clinical evidence |
Steroidogenic tissues use internal cholesterol; genetic and trial data reassuring |
|
LDL lowering does not work |
FALSE. Robust causal evidence |
Continuous proportional benefit; no lower threshold of benefit identified |
|
Women don't benefit equally |
MYTH. Evidence supports equal benefit |
Undertreatment of women is the real problem, not a lack of efficacy |
|
New-onset diabetes (statins) |
REAL but modest and manageable |
Absolute risk is small; cardiovascular benefit is much larger; communicate honestly |
|
Intracerebral hemorrhage |
NOT causally supported by RCT data |
Hypertension is the driver; low LDL is not; large meta-analysis shows no signal |
|
Risky or pointless in older adults |
NOT supported for those up to age 75+ |
More than 80% of CV deaths occur after age 65; individualize in the very old |
|
Muscle destruction |
REAL but mostly manageable; overblown by nocebo |
True serious injury is rare; most patients tolerate rechallenge successfully |
The Bottom Line from America's Cardiologist
The data are clear. Achieving very low LDL cholesterol provides meaningful cardiovascular protection without the parade of horrors that wellness influencers, YouTube cardiologists, and supplement marketers warn you about. Two adverse effects are real: modest statin-associated diabetes risk, concentrated in those already near the threshold, and statin-associated muscle symptoms, which are manageable and far less common in blinded trials than in open-label settings. Everything else on that list of ten fears lacks support from high-quality randomized trial data.
Therapeutic inertia, meaning the tendency to avoid or delay intensifying treatment, is one of the biggest killers in preventive cardiology. It is not neutral. It is not cautious. When a high-risk patient stops their statin because of a TikTok video, they are making a choice that statistically increases their risk of a heart attack or stroke. We have seen this documented in Danish registry data covering hundreds of thousands of patients.
My job, and the reason I built the America's Cardiologist platform, is to give you accurate information so you can make genuinely informed decisions. That means being honest when risks are real. It also means being direct when fears are unfounded. Most of what you have heard about very low LDL cholesterol being dangerous falls into the second category.
If you have specific concerns about your lipid therapy, whether that is a statin, ezetimibe, a PCSK9 inhibitor, or a newer agent, I want to hear from you. That is exactly what the Heart 2 Heart VIP Community is for. Bring your questions, bring your labs, and let us work through the evidence together.
Lower LDL, achieved earlier and sustained longer, protects your heart. The evidence for this is overwhelming. Do not let misinformation stand between you and a potentially life-saving intervention.
Key Studies Referenced in This Article
This post is grounded in peer-reviewed evidence from the following major sources:
- Zárate-Correa et al. (2026). Safety of Very Low LDL-Cholesterol: Ten Common Concerns, Misconceptions, and Evidence-Based Clarifications. Atherosclerosis. DOI: 10.1016/j.atherosclerosis.2026.120783
- Reith et al. (2026). Assessment of adverse effects attributed to statin therapy: a meta-analysis of double-blind randomised controlled trials. The Lancet.
- Reith et al. (2022). Effect of statin therapy on muscle symptoms: CTT individual participant data meta-analysis. The Lancet.
- Reith et al. (2024). Effects of statin therapy on diagnoses of new-onset diabetes. Lancet Diabetes Endocrinology.
- Sabatine et al. (2017). Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease (FOURIER). NEJM.
- Giugliano et al. (2017). EBBINGHAUS: Cognitive Function in a Randomized Trial of Evolocumab. NEJM.
- Schwartz et al. (2023). ODYSSEY OUTCOMES Trial. European Heart Journal.
- Gaba et al. (2023). FOURIER-OLE: Long-Term Safety and Outcomes. Circulation.
- Mach et al. (2025). 2025 Focused Update of the ESC/EAS Guidelines for Management of Dyslipidaemias. European Heart Journal.
- Nielsen & Nordestgaard (2016). Negative statin-related news stories decrease statin persistence. European Heart Journal.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















