

Why Desis Get Heart Disease? Earlier And More Severe
Jun 03, 2026
Why Do Desis Get So Much Heart Disease? A Cardiologist Explains.
Why people from India and Pakistan develop heart disease earlier, more often, and more severely than almost any other ethnic population on Earth, and what the actual science says you can do about it.
Let me tell you about a pattern I see in my office that should make every Desi family sit up and pay attention.
A 46-year-old Indian or Pakistani man walks in. He is not overweight. He does not smoke. His total cholesterol looks "fine." His doctor told him his LDL was "a little high but nothing to worry about." And he is sitting across from me three weeks after a heart attack that nearly killed him.
I am a cardiologist in Toledo, Ohio. I take care of a lot of South Asian patients, and I have spent years reading the research on exactly why this keeps happening. So here is the one-sentence version, and then I will walk you through the evidence in plain English.
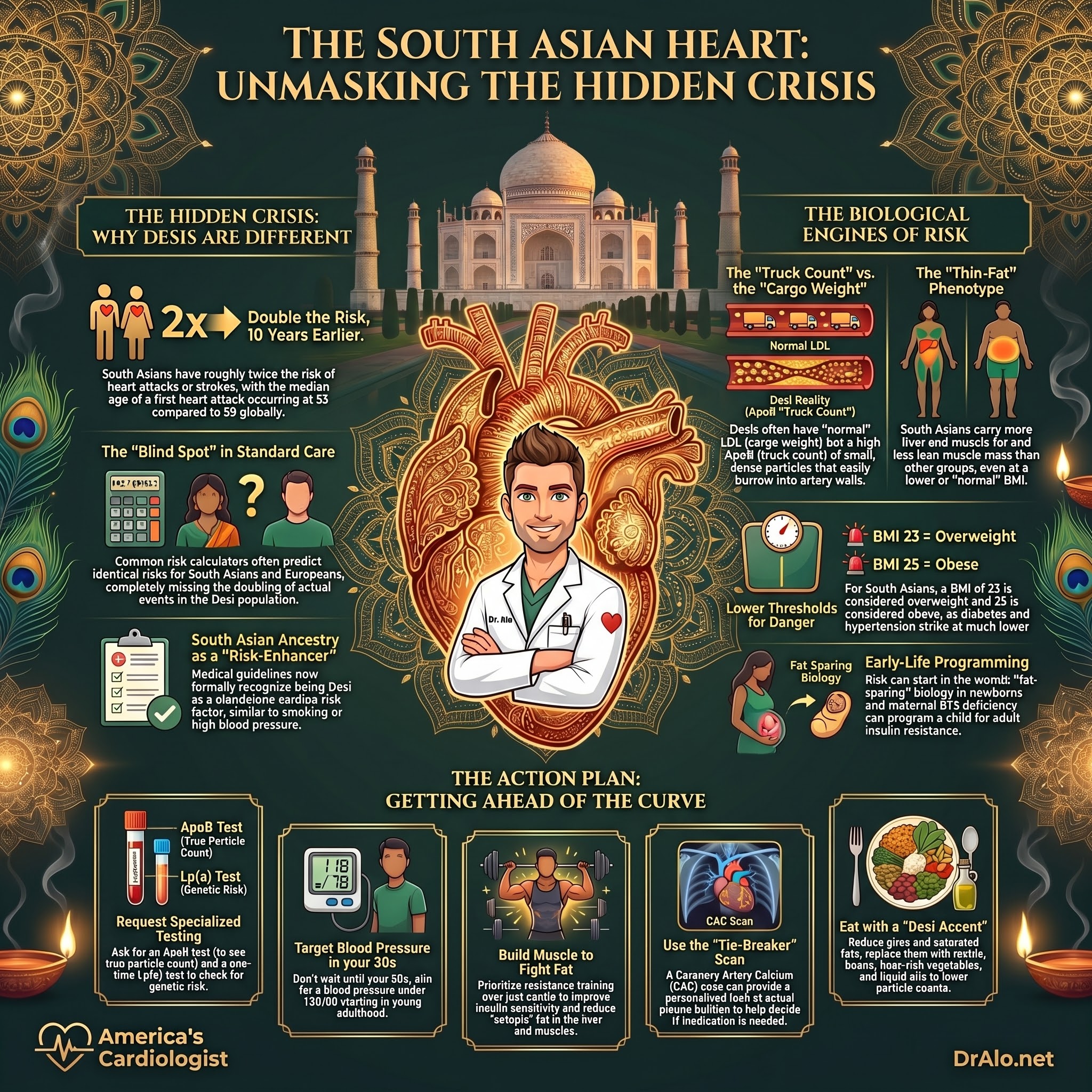
Desis, people from India, Pakistan, Bangladesh, Sri Lanka, and Nepal, carry the highest burden of heart disease of any major ethnic group on the planet, it shows up about a decade earlier, it is more severe when it shows up, and your standard risk calculator does not see it coming.
That is not an opinion. It is one of the most consistent findings in all of cardiovascular epidemiology, replicated across more than two decades of studies on three continents. Let me show you.
Infographic Summary:
How big is the problem, really?
The cleanest number comes from the UK Biobank study published in Circulation in 2021 (Patel and colleagues). They followed 8,124 middle-aged South Asians and 449,349 Europeans who started out free of heart disease, for a median of 11 years.
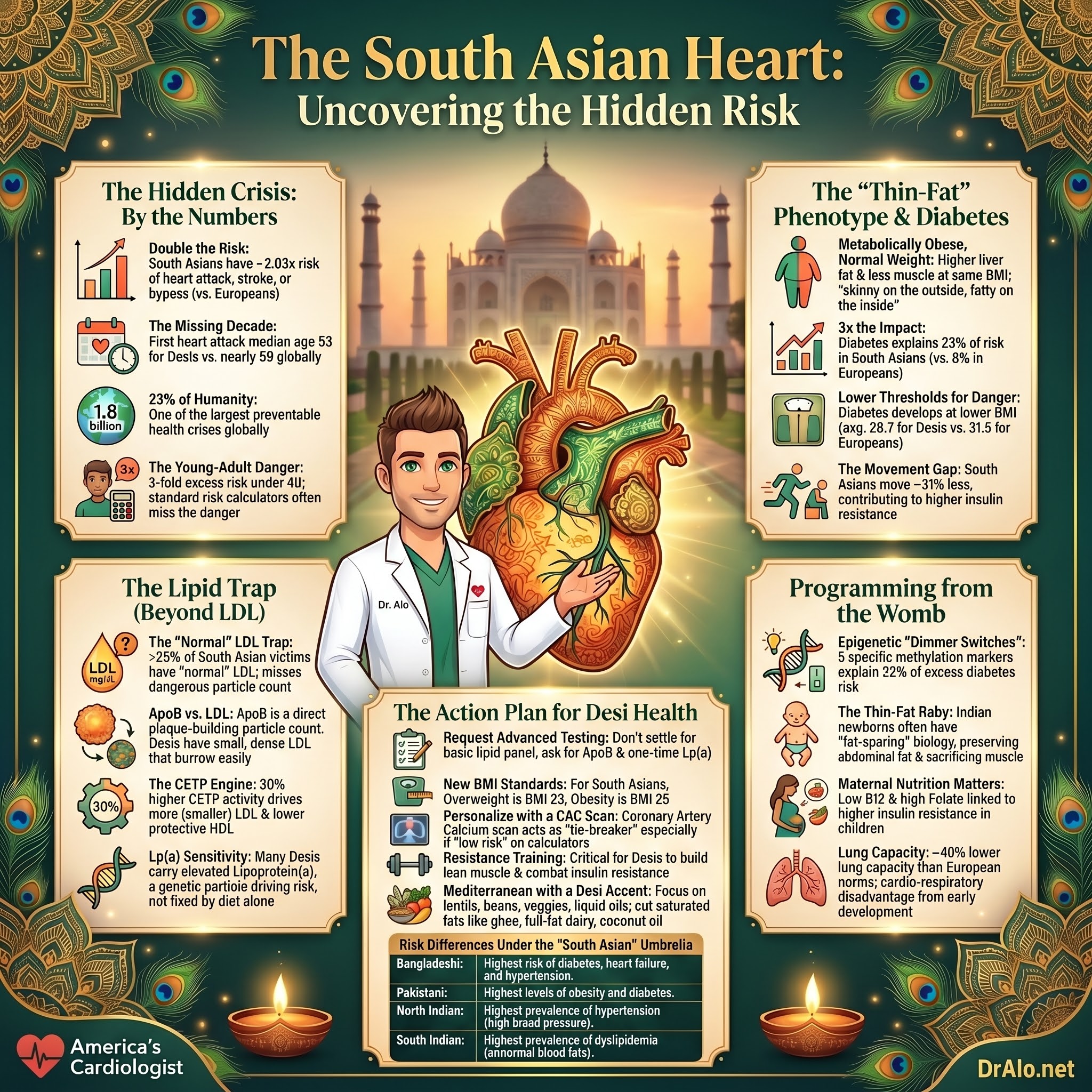
The result: South Asians had roughly double the risk of a heart attack, coronary stent or bypass, or ischemic stroke, a hazard ratio of 2.03 (95% CI 1.86 to 2.22). Double. In a modern healthcare system, with statins and blood pressure pills available to everyone.
Now here is the part that should genuinely worry you. When the researchers plugged these same people into the standard American risk calculator (the Pooled Cohort Equations) and the British one (QRISK3), the calculators predicted almost identical risk for South Asians and Europeans. The tools we use every day to decide who gets a statin completely missed a doubling of risk.
This is why, back in 2018, the American Heart Association and American College of Cardiology formally added "South Asian ancestry" to their official list of risk-enhancing factors in the cholesterol guidelines. Being Desi is, on paper, a cardiac risk factor, like high blood pressure or smoking.
And it is not just the UK. In the United States, Asian Indian men have the highest coronary artery disease prevalence of any Asian subgroup, at 13.0%. South Asians make up about 23% of humanity, roughly 1.8 billion people, so this is not a rare curiosity. It is one of the largest preventable health problems in the world.
Why so young? The decade we lose.
Here is what makes Desi heart disease so cruel: it strikes early, in people's 40s and 50s, right when they have young kids and aging parents and careers to run.
The landmark INTERHEART study (Yusuf, Lancet 2004) enrolled about 15,000 first heart attacks and 15,000 matched controls across 52 countries. Its famous finding was that just nine modifiable risk factors, abnormal lipids, smoking, high blood pressure, diabetes, belly fat, stress, too little fruit and vegetables, too little exercise, and (in some groups) alcohol, accounted for about 90% of heart attack risk worldwide, in every region, both sexes, young and old. Heart attacks are not bad luck. They are overwhelmingly the product of measurable, fixable things.
INTERHEART then ran a dedicated South Asian analysis (Joshi, JAMA 2007) with 1,732 South Asian heart attack cases and 2,204 controls from India, Pakistan, Bangladesh, Sri Lanka, and Nepal. The headline number: the median age of a first heart attack was 53 years in South Asians versus 58.8 years in people from the rest of the world. UK mortality data tells the same story even more dramatically, the excess risk is about 3-fold in Desis under 40, but only about 1.5-fold over 60. The younger you are, the more disproportionate the danger.
Now, why the early onset? This is the elegant and important part. When INTERHEART compared the strength of each risk factor, the odds ratios, they were remarkably similar in South Asians and everyone else. Smoking is just as bad for a Pakistani as for a Pole. What differed was how common the risk factors were, and how early they appeared. South Asian cases and controls under 60 already had high levels of these risk factors. The risk factors loaded earlier in life, so the disease arrived earlier. As the authors put it, the higher prevalence of risk factors in people under 60 explains the earlier onset of heart disease in South Asians.
Look at the country-specific data from that study and the picture sharpens:
- The ApoB/ApoA-I ratio (the best lipid marker, more on this below) carried an odds ratio of roughly 2.3 to 2.5 and a population-attributable risk of 43 to 49% across India, Pakistan, and the smaller countries. This is not clinically relevant and used in research.
- Belly fat (waist-to-hip ratio) had an odds ratio of 4.29 in India, meaning central obesity was hammering Indian hearts.
- High blood pressure reached an odds ratio of 4.07 in the Bangladesh/Sri Lanka/Nepal group.
- Diabetes reached an odds ratio of 3.92 in that same group.
- And the protective factors were missing: in the control groups, only 3.4% to 8.1% were doing regular moderate or vigorous exercise.
In other words, Desis are not genetically doomed to die young. They are loading the same nine risk factors earlier and heavier, and they are missing the protective habits that buffer everyone else.
It is not that Desis have "more cholesterol." It is the kind.
This is my favorite part, because it is the single most misunderstood thing about Desi heart disease, and it is exactly the area I spend my career on.
Walk into a clinic and you will hear: "But his LDL cholesterol was normal!" And that is often true. Here is the trap.
The INTERHEART lipid substudy (Karthikeyan, JACC 2009) measured lipids and apolipoproteins in 5,731 Asian heart attack cases and 6,459 controls. Two findings should be tattooed on the wall of every doctor who treats Desi patients:
- For any given LDL cholesterol level, South Asians had the highest ApoB of any group studied.
- For any given HDL cholesterol level, South Asians had the lowest ApoA-1.
Let me translate. ApoB is a direct headcount of the dangerous, plaque-building particles in your blood, there is exactly one ApoB molecule on every LDL, VLDL, and Lp(a) particle. LDL cholesterol, by contrast, just measures the cholesterol cargo riding inside those particles. It is a measure of weight, not headcount.
Desis tend to carry small, dense LDL particles. A small particle holds less cholesterol but is just as good, actually better, at burrowing into your artery wall. So a South Asian can have a "normal-looking" LDL cholesterol while actually carrying a large number of dangerous particles (apoB). The cholesterol weight on the scale looks fine; the truck count on the highway is dangerously high. That is why, in this study, more than a quarter of South Asian heart attack victims had an LDL under 100 mg/dL, a number most doctors would have called reassuring.
And the ApoB/ApoA-1 ratio was the single strongest lipid predictor of heart attack across every Asian subgroup. Not LDL. Not the cholesterol ratio. ApoB.
It gets worse on the HDL side. South Asians have a high prevalence of low HDL, in this study, 82% of South Asian cases had low HDL versus 57% of other Asians. But even their HDL is less protective, because they carry lower ApoA-1 and more small HDL particles that do a worse job of cleaning up cholesterol.
There is a mechanism underneath all this. The AHA Scientific Statement (Volgman, Circulation 2018) notes that South Asian populations have about 30% higher activity of an enzyme called CETP (cholesteryl ester transfer protein) compared with Europeans, even after adjusting for age, sex, BMI, and waist size. Higher CETP activity pushes you toward exactly this pattern: more LDL particles, smaller LDL particles, and lower HDL. On top of that, many Desis carry elevated lipoprotein(a), a genetic, ApoB-containing particle that independently drives heart attacks and aortic valve disease and does not budge with diet.
Bottom line on lipids: if you are Desi and your doctor only checks your LDL cholesterol, you are flying half-blind. Ask for an ApoB and, once in your life, an Lp(a). I will give you the script at the end.
The diabetes engine: skinny on the outside, fatty on the inside
If lipids are one engine of Desi heart disease, diabetes is the other, and it runs hotter and earlier in this population than almost anywhere.
Start with the body. The MASALA study in the US (and parallel UK work) showed that compared with White, Black, Hispanic, and Chinese Americans, South Asians carry more liver fat, more fat marbled into their muscle, and less lean muscle mass, at the same or even lower BMI. A UK study found South Asians had about 30% more triglyceride stuffed inside their muscle than BMI-matched Europeans. This is the "thin-fat" or "metabolically obese, normal weight" phenotype. You can look slim in a shirt and be metabolically on fire.
That ectopic fat, fat in the liver and muscle where it does not belong, drives insulin resistance. And South Asians appear to have weaker insulin-secreting beta cells to begin with, so they tip into diabetes faster and at lower body weights. In the Patel UK Biobank data, South Asians with diabetes had an average BMI of 28.7 versus 31.5 in Europeans with diabetes. They get the disease while still looking "less heavy."
How much does diabetes matter for Desi hearts? In that same study, diabetes explained 23% of the heart-disease risk in South Asians versus only 8% in Europeans. Diabetes is doing roughly three times the damage in this group.
Two more pieces fill in the engine:
Movement. A LOLIPOP substudy (Afaq, PLoS One 2019) strapped validated accelerometers on people and measured what they actually did, not what they claimed. South Asians moved about 31% less than Europeans (1,505 vs 2,051 MET-minutes per week), and the gap held even after accounting for age, sex, and body fat. Type 2 diabetes was about three times more common in the South Asians (17.7% vs 5.9%). Lower activity was independently tied to higher insulin resistance and glucose.
Epigenetics, and this one is wild. A nested study within LOLIPOP (Chambers, Lancet Diabetes & Endocrinology 2015) followed people who started out without diabetes and looked at chemical "dimmer switches" on their DNA (methylation marks) in blood drawn before anyone got sick. Indian Asians developed diabetes at 11.9% versus 4.3% in Europeans, a 3.1-fold higher rate that stayed 2.5-fold higher even after adjusting for body fat, blood sugar, and physical activity. The researchers found five methylation markers (at genes called ABCG1, PHOSPHO1, SOCS3, SREBF1, and TXNIP) that predicted future diabetes. A combined methylation score was 0.86 standard deviations higher in Indian Asians than Europeans, and it explained roughly 32% of the excess diabetes risk that nothing else could account for. This is among the first hard evidence that gene-environment programming, possibly set in early life, even in the womb, is baked into Desi metabolic risk.
I do not say that to make you feel doomed. I say it because it tells you to start early and treat the modifiable stuff aggressively, since you are starting from behind.
Where the "thin-fat" or "skinny-fat" body comes from: it starts in the womb
That thin-fat adult body I just described? In many Desis, it does not start in adulthood. It starts before birth.
This is the world of what scientists call the developmental origins of health and disease, the idea, first championed by David Barker, that adverse conditions in the womb and early infancy permanently "program" your metabolism for trouble later in life. India has produced some of the best evidence for it on Earth, from four landmark birth cohorts followed for decades: the Pune Maternal Nutrition Study, the New Delhi Birth Cohort, the Vellore Birth Cohort, and the Mysore Birth Records Cohort. A 2023 review in The Lancet Regional Health, Southeast Asia (Kalra and colleagues) pulled this work together, and the findings are striking.
The "thin-fat Indian baby." When researchers (Yajnik and colleagues) compared rural Indian newborns with White British babies, the Indian babies were lighter, thinner, and shorter, but they had preserved their body fat, especially the central, truncal, abdominal fat, while sacrificing lean tissue and muscle. They called it "fat-sparing." For the same birth weight, Indian babies carried more central fat than White babies. And this is not something they grow out of: Indian children continue to have a higher body-fat percentage despite lower BMI, waist, and skinfold measurements, and they are more insulin resistant with higher fasting glucose and insulin than UK children, before puberty. The adult "skinny outside, fatty inside" phenotype I described above is, for many Desis, the same body they were born with.
Maternal nutrition shapes the baby's metabolism. The Pune study found that what the mother ate mattered more than how much. Micronutrient-rich foods, green vegetables, milk, fruit, and maternal fat intake were tied to healthier birth size, while raw calories and protein were not. And here is the finding with the biggest public-health punch: a combination of high folate and low vitamin B12 in the mother produced the most insulin resistance in her child at age six. Low maternal B12 alone predicted higher insulin resistance in the kids. India runs universal folate supplementation in pregnancy but typically not B12, and many vegetarian Desi mothers are low in B12. Adding B12 is cheap and feasible, though it still needs to be proven in a trial.
Low birth weight plus rapid catch-up is the worst combination. Across the New Delhi and Vellore cohorts, the pattern that predicted adult diabetes, impaired glucose tolerance, metabolic syndrome, and even thicker carotid arteries was a baby who was born small and thin and then gained weight rapidly in childhood (an early "adiposity rebound"). Being born small was linked to more heart disease in the Mysore cohort. In other words, it is not just the low birth weight, it is the small baby dropped into an abundant, calorie-rich modern environment, where the body that was programmed for scarcity gets flooded with surplus.
One more curveball from this work: Indians have, on average, the lowest lung capacity of any population measured globally, roughly 40% would fall in the "restrictive" range by White-European norms. Low vital capacity is itself a strong predictor of cardiovascular death. It looks like the same early-life programming that shrinks lean muscle and spares fat may also shrink lung development, producing a combined cardio-respiratory disadvantage.
Why does this matter for you, today? Two reasons. First, it explains the residual risk that survives every adult risk-factor adjustment, some of your risk was set before you took your first breath, which is exactly why standard mid-life risk calculators miss it. Second, it widens the prevention window in both directions: it argues for taking the metabolic health of Desi mothers and children seriously (B12 and overall nutrition in pregnancy, avoiding rapid childhood weight gain on top of a small birth size), and it tells you, the adult, that since you started behind the line, you cannot afford to coast. You have to actively out-work a head start that disease got on you decades ago.
Infographic Summary:
Blood pressure that starts climbing in your 30s
Most people think of high blood pressure as a problem for your 60s. For Desis, the clock starts decades earlier.
A 2025 UK Biobank analysis (Cho, Hypertension) reconstructed lifetime blood pressure trajectories and found that South Asians reach a systolic pressure of 130 mm Hg by about age 40, while East Asians don't get there until about 49. By age 40, nearly 20% of South Asians already met criteria for hypertension, versus about 11% of East Asians, almost double, in young adulthood.
And that early pressure matters more. Each standard-deviation rise in young-adult systolic pressure was associated with a 41% higher odds of future heart disease in South Asians (OR 1.41), while young-adult pressure barely registered in East Asians. Over a lifetime, South Asians had a four-fold higher cumulative heart-disease incidence than East Asians (3.5 vs 0.9 per 1,000 person-years). South Asians also started blood pressure medication younger and needed more aggressive regimens, yet treatment rates were still poor in every group.
The lesson: if you are Desi, your blood pressure deserves attention in your 30s, not your 60s.
The clot factor, and a paradox worth understanding
Here is something that puzzled researchers for years. In several studies, Desis had more heart attacks and strokes despite having a similar or even smaller amount of visible plaque in their neck and heart arteries.
The Canadian SHARE study (Anand, Lancet 2000) found South Asians had the highest rate of cardiovascular disease (11%) versus Europeans (5%) and Chinese (2%), even though Europeans actually had slightly more thickening in their carotid arteries. The London LOLIPOP carotid and coronary-calcium substudies found similar amounts of subclinical atherosclerosis between Indian Asians and White Europeans, yet far more actual clinical events in the Desis.
So if it is not always more plaque, what is it? The leading explanation is a prothrombotic state, blood that clots too readily and plaque that is more prone to rupture. SHARE found markedly elevated fibrinogen, homocysteine, lipoprotein(a), and PAI-1 (a clotting factor) in South Asians. Add to this that Desis tend to have smaller-caliber coronary arteries and a higher rate of multivessel disease when they do get sick, and you have a recipe for a small plaque causing a big, deadly event.
Translation: in Desis, it may be less about how much plaque you have and more about how unstable it is and how readily your blood clots on top of it. That shifts the strategy toward controlling the particle count (ApoB) and the other rupture-and-clot drivers, hard and early.
Family history hits harder if you're Desi
We all know "heart disease runs in the family." But a SABRE analysis (Wang, Int J Cardiol 2020) showed family history is a stronger signal in South Asians. A family history of coronary disease carried an odds ratio of 1.71 in South Asians versus 1.11 in Europeans, and in Desis, that association held up even after adjusting for all the usual biological and social risk factors. In Europeans, family history mostly washed out once you accounted for their blood pressure and lipids; in South Asians, it pointed at something extra, genetics or shared early-life environment, that we still cannot fully measure.
If a parent or sibling had an early heart attack, take it seriously. In your family, it carries more weight.
Your risk calculator is lying to you
I said this at the top, but it deserves its own section because it is where the most damage is done.
The standard tools, the American Pooled Cohort Equations, the British QRISK3, the old Framingham score, were largely built on White populations. When you run a Desi through them, they systematically underestimate the real risk. In the Patel UK Biobank study, the predicted 10-year risk came out nearly identical for South Asians and Europeans despite the South Asians having double the actual events. The SABRE investigators found these scores underestimated risk especially badly in South Asian women.
What works better?
- The newer AHA PREVENT equations show nearly perfect calibration for Asian Indians specifically (Yan, JAMA Cardiology 2025), which is real progress.
- But the single most useful tool to personalize the decision is a coronary artery calcium (CAC) scan, a quick, low-radiation CT that directly looks for calcified plaque in your heart arteries. In the MASALA study, among intermediate-risk South Asians, 37% had a CAC over 100 (a clear statin indication), while among borderline-risk people, 54% had a CAC of zero. So a calcium scan keeps you from both under-treating the hidden high-risk person and over-treating the genuinely low-risk one. The National Lipid Association recommends CAC as the preferred tie-breaker in Desis.
One caveat I always add: a CAC of zero is reassuring for the near term, but it does not mean your arteries are clean, especially if you are young. Calcium is a late finding. Soft, non-calcified plaque comes first and can still rupture. The real game is keeping your ApoB and blood pressure low for decades so the plaque never gets going. In a young Desi, I treat the lifetime exposure, not just today's calcium score.
Two more recent advances worth knowing: South Asians tend to have lower CAC volume but higher CAC density, a distinctive plaque signature whose meaning we are still learning. And the combined MASALA + DILWALE datasets have now produced the first sex-specific CAC percentile curves for South Asians in the US, so we can finally interpret a Desi's calcium score against Desi norms instead of White norms.
"South Asian" is not one thing
Lumping 1.8 billion people into one box is lazy and it costs lives. The data show meaningful differences within the Desi umbrella.
- PURE (Joseph, European Heart Journal 2022), which followed 33,583 people across India, Bangladesh, and Pakistan for 11 years, found heart-disease incidence was dramatically higher in Bangladesh (17.1 per 1,000 person-years) and Pakistan (9.7) than in India (4.3). Pakistan carried the highest overall INTERHEART risk score. Heart disease was the single most common cause of death across the region (35.5% of all deaths). Rural areas had higher rates than urban; men higher than women.
- A UK primary-care study (Almulhem, 2021) of nearly 95,000 South Asians found the Bangladeshi community had the highest risk of diabetes, hypertension, heart disease, and heart failure, followed by Pakistanis, then Indians.
- In the US MASALA study, diabetes and obesity were highest in Pakistani participants, hypertension was highest in North Indians, and dyslipidemia was highest in South Indians and Pakistanis.
Same umbrella, different storms. Prevention has to be tailored, not one-size-fits-all.
And the PURE study added a sobering twist about death (as opposed to just heart attacks): the biggest population-level drivers of mortality were low education (PAF ~19%) and low grip strength (~15%), markers of poverty and frailty, alongside diet, diabetes, tobacco, and hypertension. The biggest drivers of heart disease specifically were hypertension (13%), high non-HDL cholesterol (11%), and diabetes (9%). Social conditions and strength matter enormously, especially back home.
Desi women are getting shortchanged
I need to call this out directly. The DILWALE registry (Agarwala, JACC Advances 2024), the largest electronic-health-record study of South Asians in the US, with 31,781 patients in Texas, found that among people with early-onset heart disease, women were less likely to be put on statins than men: 80.5% versus 92.1%. They were also less likely to get ezetimibe.
This happens partly because the risk calculators underperform even worse in women, so doctors hesitate. But the biology does not hesitate. In that same registry, hypertension and high cholesterol were each associated with a roughly 5- to 6-fold higher odds of premature heart disease. Desi women are not lower-risk; they are under-treated. If you are a South Asian woman, do not let anyone wave you off because you "feel fine" or "look healthy."
The honest counterpoint
I am not in the business of fear-mongering, so here is the fair other side.
When researchers throw everything at the problem, adjusting for 18 different risk factors as Patel did, the doubled risk does shrink, down to a hazard ratio of about 1.45. So a big chunk of Desi excess risk is explained by the things we already know how to fix: blood pressure, lipids, diabetes, belly fat, activity. That is genuinely good news, because it means a lot of this is in your hands.
And on the genetics: the best current evidence suggests the genetic predictors of heart disease are largely similar between South Asians and Europeans, studies just have not been large enough to find Desi-specific genetic culprits yet. So this is not mainly a "bad genes, nothing to do" story.
But a residual gap of around 1.45-fold stubbornly remains even after adjusting for everything we can measure. That leftover risk likely lives in the things we measure poorly, the epigenetic programming, the prothrombotic state, the small dense particles, social determinants, and factors we have not discovered yet. The takeaway is not "give up." It is "control what you can, harder and earlier than you would for someone else."
So what do you actually DO about it?
Enough theory. Here is the action plan I give my Desi patients. None of this is exotic, and most of it is cheap.
1. Get the right blood tests, not just the basic panel. Ask for an ApoB (it doesn't require fasting and it's standardized and inexpensive). Ask once in your life for an Lp(a). If your doctor says LDL is enough, push back politely: in Desis, a "normal" LDL can hide a high particle count.
2. Aim much lower on your particles than the lab "normal." Lab reference ranges tell you what's average in a population where heart disease is the leading killer, average is not the goal. For prevention, I want ApoB comfortably under ~90 mg/dL for most people, and under ~65 mg/dL (with LDL under ~55) for higher-risk patients with diabetes, established disease, or strong family history. Lower is better for the particles that cause plaque.
3. Treat blood pressure starting in your 30s, not your 60s. Know your numbers young. Aim for under 120/80 if you can do it safely. This is the single biggest population-level driver of Desi heart disease in the PURE data.
4. Hunt the "thin-fat" body, not just the scale. Use the lower South Asian BMI thresholds: 23 is overweight, 25 is obesity. Watch your waist. The goal is less liver and muscle fat and more lean muscle, which means resistance training, not just cardio. Lifting weights directly improves insulin sensitivity, the core Desi problem.
5. Move 31% more than you think you need to. Desis under-move by about a third on objective measurement. Build to 7,500+ steps a day plus structured exercise. This independently lowers insulin resistance.
6. Eat like the Mediterranean, with a Desi accent. Cut saturated fat (ghee, full-fat dairy, fatty meats, coconut oil, yes, including the stuff in a lot of traditional cooking). Lean on lentils, beans, vegetables, whole grains, nuts, and liquid oils. Beans and soluble fiber genuinely lower particle number. This is the easiest high-impact lever there is.
7. Do Not Use a CAC scan to personalize the statin decision. If you are thinking of using a calcium score, then you should be on medication. Abnormal calcium means you have late stage ASCVD and it has been there for decades. If your patient refuses to take a proactive approach, you can use a CAC score to convince them. A calcium scan tells you far more than your ethnicity-blind risk score. But remember: a zero in a young person means keep doing the right things, not "you're invincible." You should take the opportunity to get on medications and not delay.
8. When lifestyle isn't enough, use the medicines that actually have outcome data. That means statins first, then ezetimibe, then PCSK9 inhibitors if needed, not red yeast rice, not berberine, not a cabinet of supplements. Two old, cheap drugs (rosuvastatin and ezetimibe) get most people to target. If a product promises to "clean your arteries" without lowering your particle count, it's marketing, not medicine.
9. Desi women: demand the same aggressive prevention as men. You are not lower risk. The data say you are often under-treated.
10. Think about the next generation, too. Because so much of this is programmed early, the metabolic health of Desi mothers and children matters. If you are pregnant or planning to be, talk to your doctor about vitamin B12 as well as folate (many vegetarian South Asian mothers run low on B12), and about overall nutrition quality. In kids born small or thin, avoid pushing rapid catch-up weight gain, build healthy habits early instead. You may be breaking a cycle that started generations ago.
And here is the proof it works: a culturally tailored program inside Kaiser Permanente (the Heart Health for South Asians program) gave South Asian patients a focused class on diet and lifestyle and followed them for years. The matched analysis showed significant reductions in coronary revascularization (about two-thirds lower) and all-cause mortality (about 60% lower). When you target the right risk factors in this population, the needle moves a lot.
Bottom line
Desis get more heart disease, earlier, and more severely because a perfect storm stacks up early in life: small dense atherogenic particles that hide behind a "normal" LDL, an insulin-resistant "thin-fat" body that tips into diabetes at low weights, blood pressure that climbs in the 30s, a clot-prone bloodstream, family-history risk that hits harder, and an epigenetic head start on metabolic disease, all of it invisible to the standard risk calculators that decide who gets treated.
None of that is a death sentence. Most of it is measurable, and most of it is treatable. The Desi who knows their ApoB, controls their blood pressure from young adulthood, builds muscle, eats real food, gets a calcium scan when appropriate, and uses proven medicines when needed can flatten this curve dramatically.
If you are Desi, do not wait for symptoms and do not trust a "normal" basic panel. Start early. Aim lower. Push your doctor. Your arteries have a head start on you, get in front of it.
Want to go deeper on this?
If you or someone in your family is Desi, this is exactly the kind of thing I help people get ahead of. I run a free longevity webinar where I walk through how to read your real numbers and build a prevention plan that fits this risk profile. You can grab a seat at https://dralo.net/webinar.
And if you want ongoing, evidence-based guidance and a community of people taking their heart health seriously, come join my private Heart 2 Heart VIP Community at https://dralo.net/community. It's where I share the practical, no-nonsense version of everything above.
Frequently Asked Questions
Why do Indians and Pakistanis get heart disease so young?
Because the major risk factors, abnormal particles, diabetes, high blood pressure, belly fat, low activity, load up earlier in life and are more common, even though each one is no more dangerous than it is in anyone else. Heart attacks hit a decade earlier on average (median age ~53 vs ~59).
My LDL cholesterol is normal. Am I safe?
Not necessarily, and this is the most dangerous myth for Desis. South Asians carry more, smaller particles for any given LDL number. Get an ApoB to see your true particle count. Over a quarter of South Asian heart attack victims had an LDL under 100.
What blood tests should a Desi person ask for?
A standard lipid panel plus ApoB, and lipoprotein(a) once in adulthood. Know your blood pressure, fasting glucose/HbA1c, and waist measurement too.
At what BMI is a South Asian overweight?
Lower than the Western cutoffs: 23 is overweight, 25 is obesity for South Asians, per the WHO and AHA. You can be metabolically unhealthy at a "normal" Western BMI.
Should I get a coronary calcium scan?
Often, yes, it's the best tool to personalize whether you need a statin, and there are now South Asian-specific reference values. Just remember a zero score in a young person isn't a free pass.
Is this all genetic? Is there anything I can do?
Genetics and early-life programming play a real role, but the majority of the excess risk runs through things you can change: blood pressure, particles, diabetes, weight, and activity. Programs that target these have cut revascularization and mortality substantially in Desi patients.
I've heard heart disease in Indians "starts in the womb." Is that real?
There's strong evidence for it. Indian babies are often born "thin-fat", lighter and with less muscle but preserved central fat, and that body composition, plus early insulin resistance, tracks into childhood and adulthood. Maternal nutrition matters: in the Pune study, high folate combined with low vitamin B12 in mothers produced the most insulin resistance in their children. It doesn't mean your fate is sealed; it means starting prevention early, including in pregnancy and childhood, pays off.
Does it matter if I'm Indian vs Pakistani vs Bangladeshi?
Yes. Risk profiles differ, for example, Bangladeshis tend to carry the highest diabetes and heart-failure risk, Pakistanis high diabetes and obesity, North Indians the most hypertension, South Indians the most dyslipidemia. Prevention should be tailored.
References
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















