Why Most Heart Attacks Happen With Normal LDL Levels: Understanding the Real Data
Jun 23, 2026
Why Most Heart Attacks Happen With Normal Cholesterol?
Every single day on social media, I get the same question: "Dr. Alo, if most people having heart attacks have normal cholesterol, then isn't cholesterol the real problem? Isn't it something else?" The answer is surprisingly simple, but online grifters profit from making it complicated by claiming this statistic proves cholesterol is irrelevant.
This interpretation shows a severe lack of understanding of the data. Let me walk you through exactly what's happening, why it's happening, and why it actually proves the opposite of what the cholesterol deniers claim.
The Paradox: Why Do 50-73% of Heart Attack Patients Have "Normal" Cholesterol?
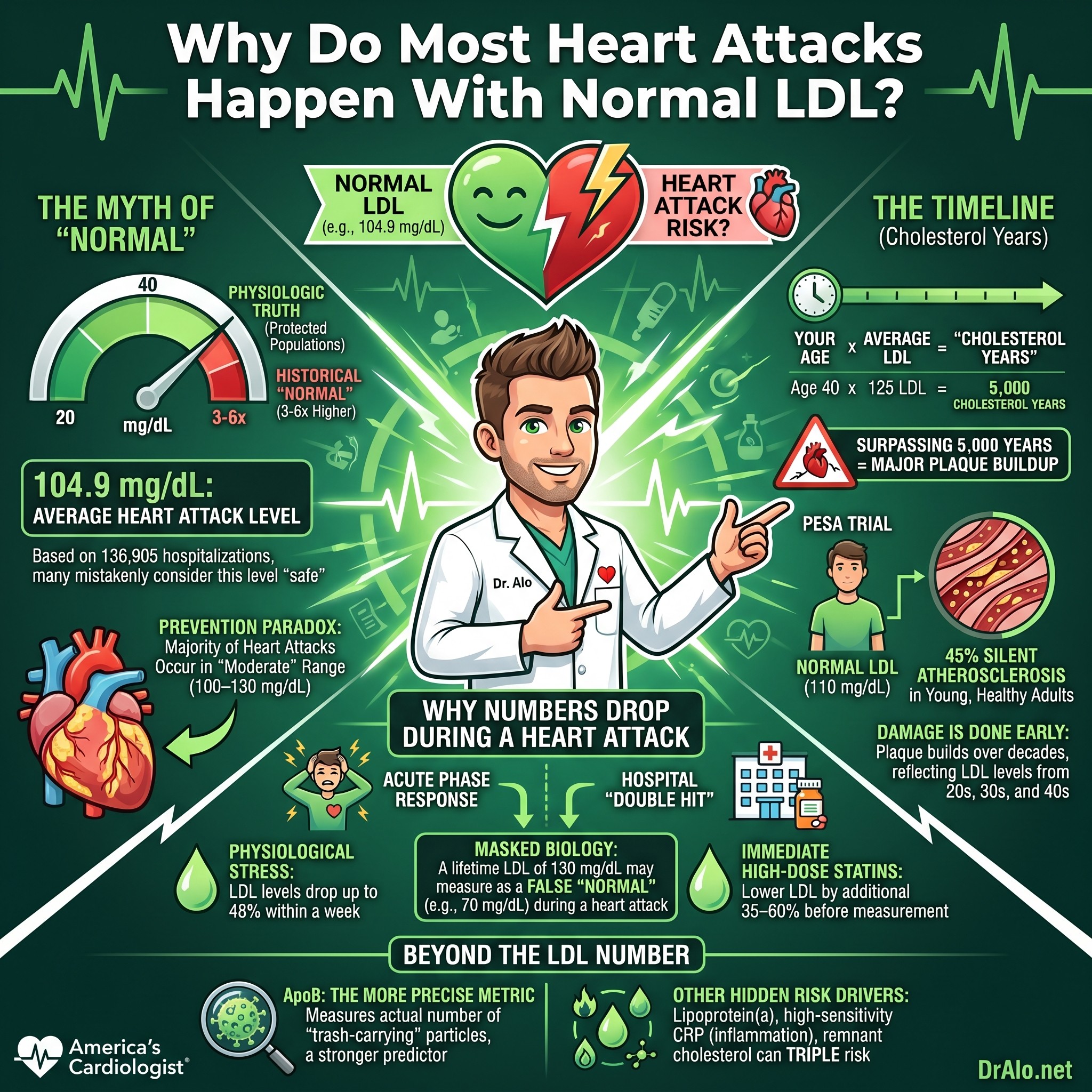
When studies examine people walking through the door having a heart attack, they find that anywhere between 50 and 73% have what's called "normal" cholesterol levels according to older guidelines. A massive analysis of 136,905 CAD hospitalizations from Get With The Guidelines found that the mean admission LDL-C was only 104.9 mg/dL, with nearly half of patients having LDL-C below 100 mg/dL at admission. This statistic gets weaponized by people selling conspiracy theories and supplement nonsense as proof that cholesterol doesn't matter. But the answer lies in understanding what "normal" actually means and why these numbers don't tell the whole story.
The problem starts with our outdated definitions. We used to think an LDL cholesterol of 130 was normal. We used to think total cholesterol of 200 was normal. These guidelines changed in 2018, and for good reason. We now recommend LDL under 100 for the general population and ideally much lower for those at risk. But the real issue is even more fundamental than that.
Infographic Summary:
What Is Actually Normal? The Physiologic Truth About LDL Cholesterol
Here's what most people don't understand: physiologic LDL cholesterol in humans is 20 to 40 mg/dL. This is what we see in populations with lifelong protection from atherosclerotic cardiovascular disease. We know with absolute certainty that ASCVD does not occur with lifelong LDL-C of 20 to 40 mg/dL. This is not a debate. This is established fact.
So when we were calling LDL of 130 "normal," we were off by a factor of three to six. No wonder half the people having heart attacks appeared to have "normal" cholesterol. By today's standards, which are much closer to reality, the picture is completely different.
The data is crystal clear: the lower your LDL cholesterol, the less atherosclerosis, less heart disease, less mortality. Period. This relationship holds true regardless of how you lower it. Whether it's through genetic mutations, medications, diet, or lifestyle, the mechanism doesn't matter. Lower LDL equals better outcomes. This isn't debatable. If you want to debate it, you're anti-science and anti-evidence.
Cholesterol Years: Why Lifetime Exposure Matters More Than a Single Number
Here's the critical insight that changes everything: at an LDL cholesterol of about 60 mg/dL or higher, most people are laying down plaque. But the real damage isn't done in a day or a year. It's done over decades.
This is where the concept of "cholesterol years" comes in, a framework published by Dr. Michael Shapiro. Think of it like "pack years" in smoking. If you smoke 1 pack a day for 20 years, we say you have a 20 pack-year history. Dr. Shapiro argues we should use the same concept for cholesterol.
If you multiply your age by your LDL cholesterol, you get your cholesterol years. A 40-year-old with an LDL of 125? That's 5,000 cholesterol years. The threshold is approximately 5,000. Above that, you definitely have plaque. Below that, you have less. This simple calculation explains why lifetime exposure matters infinitely more than a single cholesterol number at the time of your heart attack.
In his groundbreaking paper, Dr. Shapiro illustrates this beautifully. If you have severe familial hypercholesterolemia from birth with lifelong high LDL, you'll have cardiovascular events at a very early age. On the flip side, individuals with lifelong very low LDL cholesterol, either from genetics or from very early lipid-lowering therapy, never develop ASCVD. Everyone else falls somewhere in between. The lower your LDL for longer, the longer the delay before atherosclerotic disease emerges.
The PESA Trial: Subclinical Atherosclerosis in Healthy Young Adults
The Prevention of Early Subclinical Atherosclerosis (PESA) trial examined young people with no other risk factors. These were lean, active people, average age around 40, with no metabolic syndrome, no obesity, and no insulin resistance. Researchers looked purely at LDL cholesterol levels and what they found was shocking:
People with "normal" LDL of 110 mg/dL? 45% already had atherosclerosis. People with LDL of 130? 54% had atherosclerosis. People with LDL of 150? 68% had atherosclerosis. None of them had symptoms yet. The disease was brewing silently in their arteries, building plaque for years before they would ever have a clinical event.
Here's the really concerning part: of the people who had atherosclerosis, 63% had it in more than one arterial bed. They didn't just have it in their coronaries. They had it in their femorals, their carotids, their kidney arteries, and everywhere else researchers measured. This isn't localized disease. This is systemic plaque burden throughout the body.
Why Heart Attack Patients Appear to Have Normal Cholesterol: The Timing Problem
The vast majority of people who have heart attacks are men in their 50s and 60s, and women in their 60s and 70s. In the United States, we don't put people on lipid-lowering therapy until it's far too late. We use 10-year risk calculators that tell us a 40-year-old with an LDL of 110 to 130 has only a 3% risk of a heart attack in the next decade. So we don't treat them.
That person spends 40, 50, or 55 years building atherosclerosis while their LDL stays elevated. They had elevated LDL in their 20s, 30s, and 40s and were never placed on therapy. Finally, at 75% risk by the calculator, they get put on a statin at age 50 or 60. A few years later, they have a heart attack, but their LDL is now 70 because they're on therapy. And the study records them as having "normal" cholesterol at the time of their event.
This is exactly backwards. The ideal time to lower LDL is between ages 20 and 50, not between 50 and 80. By age 50, if your LDL has been 110 or higher, you've already built substantial plaque burden. We spend the rest of your life trying to stabilize it, not prevent it.
Michael Makover, Michael Shapiro, and Peter Toth wrote a recent paper making this exact argument: "There is urgent need to treat atherosclerotic cardiovascular disease risk earlier, more intensively, and with greater precision." They argue that we are not doing a good enough job. We wait too long to treat elevations in lipids. They also argue that if we started sooner, then we could eliminate ASCVD nearly completely.
The Acute Phase Response: Why Cholesterol Drops During a Heart Attack
Here's a mechanism that completely changes the picture and explains why so many people appear to have "normal" cholesterol when they have their event. When people have a heart attack, they're under extreme physiological stress. The acute-phase response following myocardial infarction causes LDL-C to decline within 24 to 48 hours, with maximal reductions of up to 48% below baseline by day 7. Even modest declines of 5 to 10% can shift a borderline-high LDL into the "normal" range when measured at admission.
This is not a coincidence. LDL cholesterol, total cholesterol, and apoB are acute phase reactants. Meaning they are altered significantly when someone is having an acute "anything." Any severe stress on the body and they can drop dramatically. Other acute phase reactants may go up. Thyroid hormones, cortisol, and many others can be elevated.
A person with an LDL of 110 or 130 before their heart attack might be down to 90 by the time it's measured in the hospital. It "looks normal." But it's been elevated for decades. Their triglycerides, meanwhile, spike by 17 to 20% as an acute phase reactant response. Their cortisol changes, their thyroid hormones shift, their inflammatory markers elevate. This is the body's stress response, and it temporarily masks the real problem.
The Double Hit: Acute Phase Response Plus Immediate Statin Therapy
Here's where the picture gets even more complicated. When someone walks through the door with an acute myocardial infarction, guidelines require that they get atorvastatin 40 mg or higher immediately. In fact, the second they arrive, most academic centers and guideline-concordant facilities give them Lipitor 80 or Crestor 40. This was established by the PROVE-IT trial, which demonstrated that immediate high-dose statin therapy reduced mortality by 16% even within the first 14 days.
So now we have a double hit. Your LDL-C and apoB are already low due to being acute phase reactants from the stress of the heart attack. Then you add high-dose statin therapy on top of that. Statins will cause a significant reduction in LDL-C and apoB even in just one day. Studies show that on day 1 after a heart attack you can see up to a 9% decline in LDL-C from the acute phase response alone. By day 4 it can be reduced by up to 17% from the stress response. When you add statins, you get an additional 35 to 60% reduction in lipids.
A patient with pre-event LDL of 130 could easily end up at 60 to 70 after the acute drop plus medication. The lipid profile at the time of diagnosis reflects acute stress and early treatment, not the lifetime exposure that caused the disease. This is why so many people having heart attacks appear to have "normal" or even "low" cholesterol. They don't. They have been building disease for decades.
The Lipid-Lowering Therapy Timing Issue
Additionally, some people who are having heart attacks are already on lipid lowering therapy and hence their LDL-C is already reduced. But they haven't been on it long enough. It's lifelong exposure to high LDL-C that causes atherosclerosis, not recent lipid levels.
Many people with heart attacks were started on statin therapy too late in life. They probably had elevated LDL-C in their 20s, 30s, and 40s and were never placed on statin therapy because our risk calculators didn't recommend it. Then they are finally placed on a statin at age 50 or 60 and have a heart attack with "normal" or "low" cholesterol.
Many times, they are not even on a statin at the time of their first heart attack. It's a bit too late and now they have extensive plaque and it's irreversible. Plaque does not magically go away once you reduce your LDL-C at a later age. It just stabilizes. The damage from decades of elevated cholesterol is already done.
Beyond LDL-C: Why ApoB and Other Risk Factors Matter
Here's something that just came out in the 2026 ACC/AHA Dyslipidemia Guidelines and I want you to understand it clearly. LDL-C measures cholesterol mass, not atherogenic particle number. That's a critical distinction. Apolipoprotein B (apoB), which directly quantifies the actual number of atherogenic particles, is a stronger predictor of cardiovascular events than LDL-C, particularly in patients with metabolic syndrome, diabetes, or elevated triglycerides.
This means you can have "normal" LDL-C but elevated apoB due to an abundance of small, cholesterol-depleted LDL particles. This is called LDL-C/apoB discordance, and it's far more common than people realize. The new guidelines now recommend apoB measurement in patients with cardiometabolic disease. Even more importantly, in primary prevention, when researchers assessed both metrics together, only apoB remained significantly associated with incident heart attacks. LDL-C alone wasn't the predictor. This is a major shift in how we should be thinking about cholesterol risk.
But LDL and apoB are only part of the story. Even at low LDL-C levels, several independent pathways drive heart attack risk. One in three patients under 50 years old having a heart attack has elevated lipoprotein(a), or Lp(a). I've covered Lp(a) extensively because it's 3 to 6 times more atherogenic than normal lipoproteins and many people don't know they have it.
Inflammation is another major factor. High-sensitivity CRP is actually a stronger predictor of cardiovascular events than LDL-C in patients already on statins. A recent collaborative analysis of three randomized trials found that hsCRP quartiles were more robustly associated with major cardiovascular events than LDL-C quartiles. This doesn't mean cholesterol doesn't matter. It means the picture is more complex than one number.
Remnant cholesterol from triglyceride-rich lipoproteins also contributes to atherogenesis independently of LDL-C. These are captured by non-HDL-C and apoB but not by LDL-C alone. When researchers looked at over 300,000 individuals in UK Biobank, they found that the combination of elevated Lp(a), remnant cholesterol, and hsCRP identified individuals at nearly 3-fold higher heart attack risk compared to those with none elevated, all independent of LDL-C. This is why I'm always telling people it's not just one number. It's the whole picture.
The Prevention Paradox: Why Most Events Occur in the "Normal" Range
Here's something most people don't understand about statistics. Because most adults have LDL-C in the "normal" range of 100 to 130 mg/dL, the majority of heart attacks will inevitably occur in this large group, even though higher LDL-C confers higher per-person risk. This is a classic example of the "prevention paradox." Most events come from the large moderate-risk population, not the small high-risk tail. It's a population statistics issue, not evidence that cholesterol is irrelevant.
The Critical Truth: Why This Actually Proves Cholesterol Matters
So when you see statistics saying "most heart attacks happen in people with normal cholesterol," remember what's really happening:
Our "normal" ranges were always too high by a factor of three or more. Many of these patients have been on lipid-lowering therapy for years, but started too late. Many got high-dose statins the moment they arrived at the hospital, which normalized their cholesterol by measurement but not by biology. Many had subclinical atherosclerosis for decades before their event as demonstrated in the PESA trial. And the acute phase response of a heart attack itself, combined with immediate statin therapy, drops cholesterol dramatically.
This is well-established science. It's been demonstrated since 1913 when researchers infused animals and humans with high lipoproteins and watched fatty streaks develop within hours. It's not debatable. It's not mysterious. And it's absolutely not a conspiracy.
The real message is this: prevention starts early. If you spend 30 years with an LDL of 50 between ages 20 and 50, your outcomes will be dramatically better than if you spend those years at LDL of 110 and try to fix it between ages 50 and 80. By then, the plaque is already there.
We know that it's better to treat elevated LDL-C sooner, younger, and stronger. But unfortunately, many doctors have not been treating lipids aggressively enough. If we started lipid-lowering therapy earlier and more intensively in people who need it, we could eliminate atherosclerotic cardiovascular disease nearly completely.
References
Get With The Guidelines: Lipid Levels in 136,905 CAD Hospitalizations
PESA Trial: Subclinical atherosclerosis in lean and healthy young people
PROVE-IT Trial: High-dose statin therapy in acute coronary syndromes
Shapiro M. Cholesterol Years as a metric for lifetime LDL exposure
2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia
JAMA: Association of ApoB, Non-HDL, and LDL With Cardiovascular Risk
Acute phase response: lipid and apoB changes during myocardial infarction
LDL cholesterol changes during acute coronary syndrome
Acute phase reactants in myocardial infarction
Statin therapy and lipid lowering in acute MI
JAMA: Cholesterol levels and cardiovascular events
Lipid changes during acute myocardial infarction
Historical perspective: Atherosclerosis and cholesterol
Early lipid changes in acute coronary disease
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine