

Does Berberine Lower Blood Sugar?
Apr 09, 2026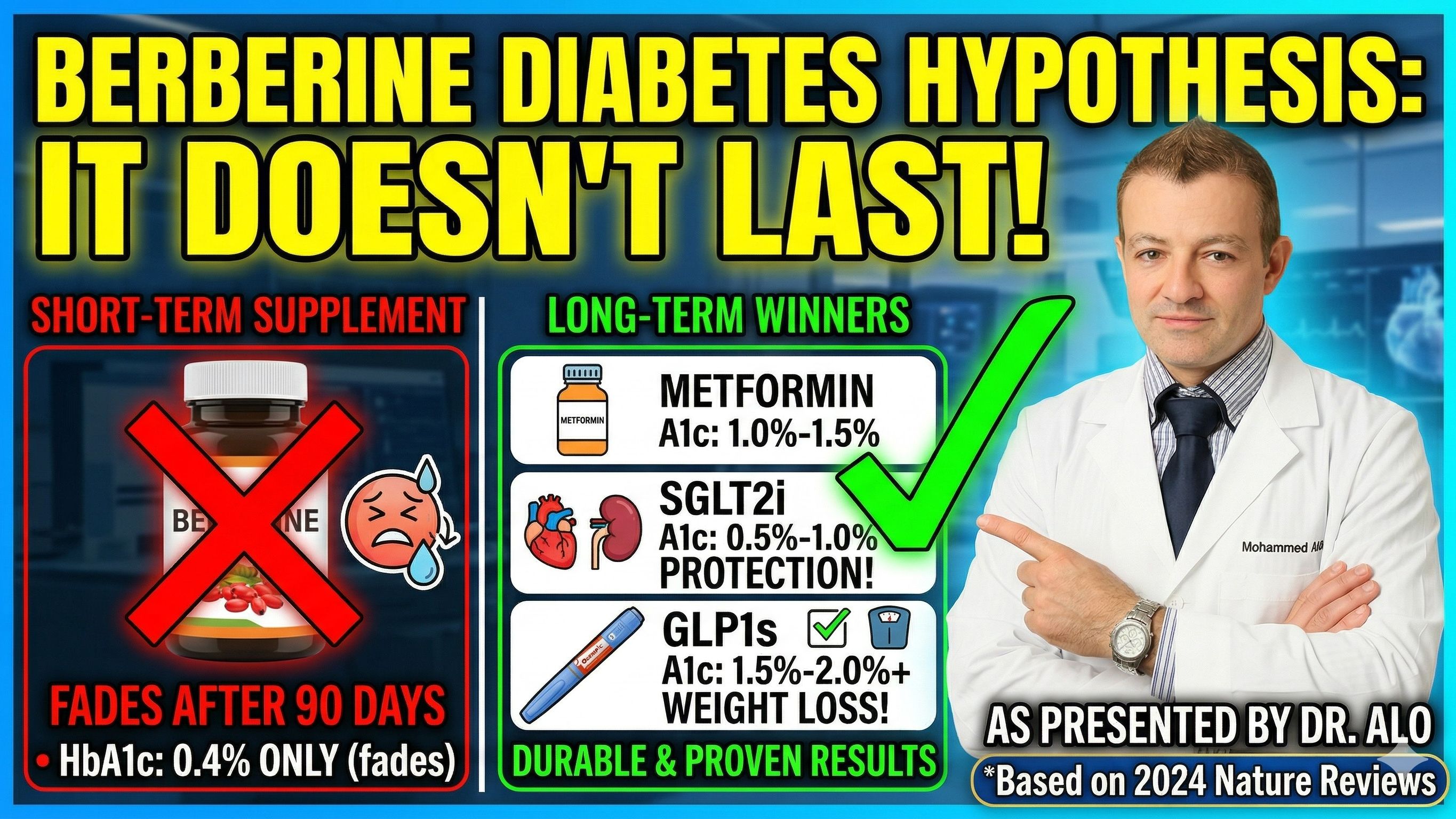
Does Berberine Work for Diabetes? Here's What the Science Actually Shows
If you've been researching natural approaches to managing type 2 diabetes, you've likely come across berberine. It's a compound extracted from various plants and has been used in traditional medicine for thousands of years. Supplement companies market it aggressively, and social media has turned it into something of a phenomenon. Before you spend money on it, though, you need to understand what the clinical data actually shows, and more importantly, what it doesn't show.
Modern therapeutics can nearly reverse type 2 diabetes completely, how does berberine stack up? Does it even work?
Yes, It Lowers Blood Sugar. But How Much?
Berberine does produce measurable reductions in blood sugar. That part is real. But the size of those reductions deserves an honest look.
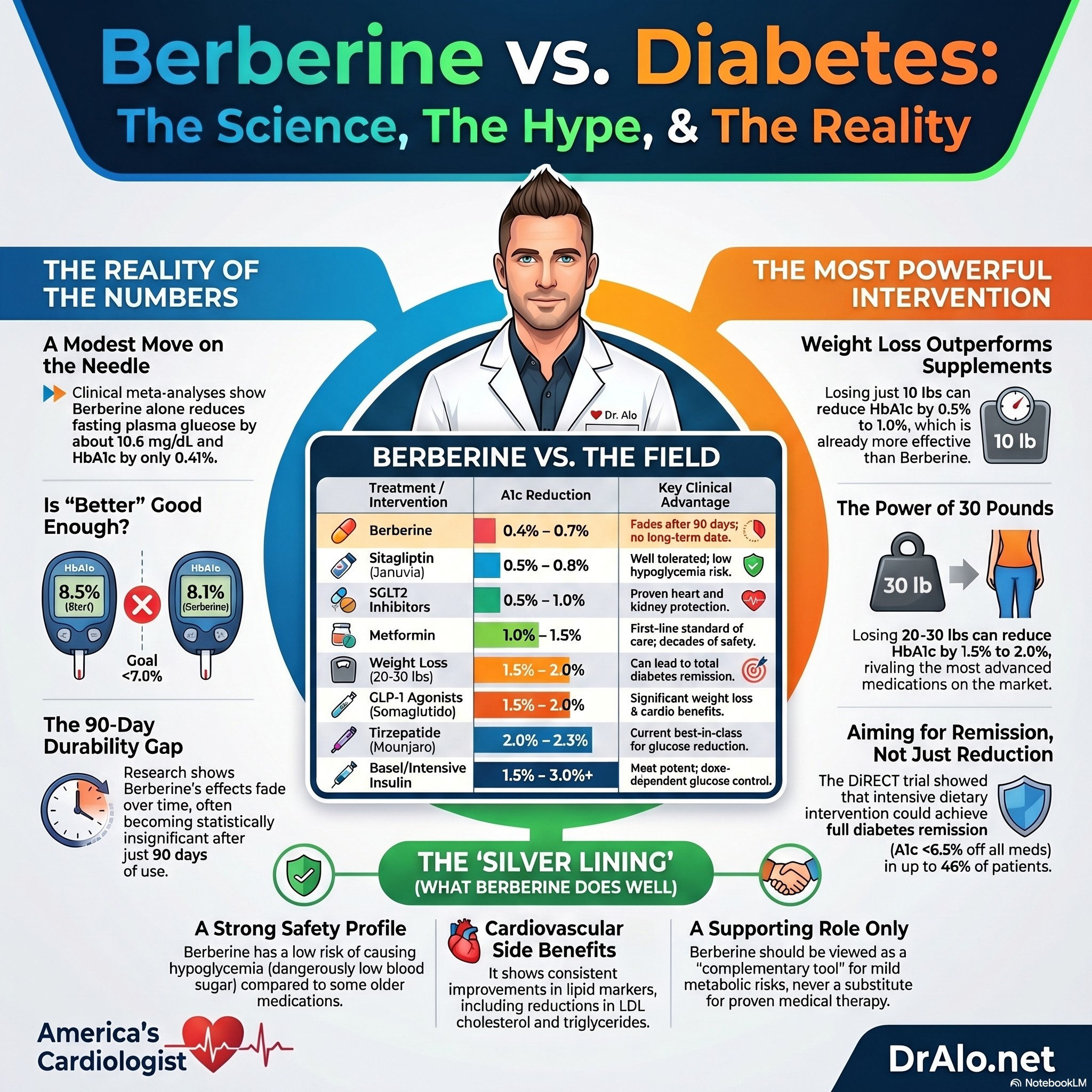
A comprehensive 2024 meta-analysis of 50 randomized controlled trials found that berberine alone reduced fasting plasma glucose by about 10.6 mg/dL. A 2023 analysis of 20 trials found it lowered HbA1c by 0.41%. When combined with standard diabetes medications, some studies show HbA1c reductions closer to 0.69%.
To put those numbers in perspective: most patients newly diagnosed with type 2 diabetes have HbA1c levels in the range of 7.5% to 9% or higher. A reduction of 0.41% moves the needle, but it does not come close to bringing most patients to the standard target of below 7%. For someone starting at 8.5%, berberine might get them to 8.1%. That is not controlled diabetes.
Berberine Diabetes Summary Infographic:
The 90-Day Problem Nobody Talks About
Here is the limitation that supplement marketing almost never mentions. One meta-analysis found that berberine's glucose-lowering effects became statistically unremarkable when treatment lasted more than 90 days. The modest reductions seen in shorter trials did not hold up over time.
This is a critical distinction. Type 2 diabetes is a lifelong condition. What matters is not whether a treatment works for two or three months. What matters is whether it works for years, consistently and safely. Berberine has not demonstrated that. The blood sugar reductions, already modest to begin with, appear to fade.
How Does Berberine Compare to Every Major Diabetes Treatment?
This is where the comparison gets stark. Here is how berberine stacks up against every major class of diabetes medication, plus the most powerful intervention of all.
|
Treatment |
A1c Reduction |
Key Notes |
|
Berberine |
0.4% to 0.7% |
Fades after 90 days, no long-term data |
|
Sitagliptin (Januvia) |
0.5% to 0.8% |
Well tolerated, no cardiovascular benefit |
|
SGLT2 inhibitors |
0.5% to 1.0% |
Strong heart and kidney protection |
|
Pioglitazone (Actos) |
0.5% to 1.4% |
Heart failure risk, weight gain |
|
Metformin |
1.0% to 1.5% |
First-line standard of care |
|
Glimepiride |
1.0% to 2.0% |
Hypoglycemia risk, weight gain |
|
GLP-1 agonists (semaglutide) |
1.5% to 2.0% |
Weight loss, proven cardiovascular benefit |
|
Tirzepatide (Mounjaro) |
2.0% to 2.3% |
Best in class currently |
|
Basal insulin |
1.5% to 2.5% |
Most potent add-on, dose dependent |
|
Intensive insulin |
3.0%+ |
Maximum potency, hypoglycemia risk |
|
Weight loss of 20 to 30 lbs |
1.5% to 2.0% |
No prescription required |
Berberine sits at the bottom of this table, with effects that may not even last past three months.
Metformin reduces A1c by 1.0% to 1.5%, two to three times more than berberine, with decades of safety data, proven durability, and a well-understood mechanism. It costs pennies a day as a generic.
SGLT2 inhibitors such as empagliflozin, canagliflozin, and dapagliflozin reduce A1c by 0.5% to 1.0%. On raw glucose-lowering, this class overlaps somewhat with berberine's numbers. But the comparison stops there. The EMPA-REG, CANVAS, and DECLARE cardiovascular outcome trials demonstrated that SGLT2 inhibitors significantly reduce the risk of heart failure hospitalization, cardiovascular death, and kidney disease progression. Berberine has no such outcome data.
GLP-1 receptor agonists such as semaglutide (Ozempic, Wegovy) reduce A1c by 1.5% to 2.0%. Tirzepatide (Mounjaro), a dual GIP/GLP-1 agonist, has shown reductions up to 2.0% to 2.3% in the SURPASS trials. These medications also drive substantial weight loss, reduce cardiovascular events, and in recent trials have demonstrated benefits in heart failure and kidney disease. They are in a completely different category.
Sulfonylureas like glimepiride reduce A1c by 1.0% to 2.0%, making them potent glucose-lowering agents, though they come with meaningful hypoglycemia risk and tend to cause weight gain of 2 to 4 kg. Their durability also wanes over time as beta cell function declines.
Pioglitazone reduces A1c by 0.5% to 1.4% by improving insulin sensitivity. It has relatively durable effects but carries significant downsides including weight gain, fluid retention, increased fracture risk, and a black box warning for heart failure. It has largely fallen out of favor in cardiology-informed diabetes management for those reasons.
Sitagliptin (Januvia) is both the brand and generic name for the same drug. It reduces A1c by 0.5% to 0.8%, is well tolerated with low hypoglycemia risk, but showed no cardiovascular outcome benefit in the TECOS trial. A safe but modest option.
Insulin remains the most potent glucose-lowering agent available. Basal insulin alone typically reduces A1c by 1.5% to 2.5% when added to oral agents. Intensive basal-bolus regimens can reduce A1c by 3% or more, though with increasing hypoglycemia risk and weight gain.
The Most Powerful Intervention Isn't a Pill at All
Here is the most important point in this entire article, and the one most often buried in supplement discussions: weight loss is one of the most potent tools available for improving blood sugar control, and it requires no prescription.
As a general benchmark, losing 1 kg (about 2.2 lbs) of body weight produces roughly a 0.1% reduction in HbA1c. Losing 10 lbs can reduce HbA1c by approximately 0.5% to 1.0%, comparable to adding a second oral medication. Losing 20 to 30 lbs can reduce HbA1c by 1.5% to 2.0%, putting it firmly in GLP-1 territory.
The DiRECT trial is the most compelling demonstration of this principle. Intensive dietary intervention producing around 15 kg (33 lbs) of weight loss achieved diabetes remission, defined as HbA1c below 6.5% off all medications, in 46% of patients at one year and 36% at two years. Not reduction. Remission.
A motivated patient who loses 20 to 30 lbs through diet and exercise may achieve more A1c reduction than any single medication on the market, including drugs far more potent than berberine. And the modern GLP-1 and dual GIP/GLP-1 medications are so effective in part because they drive exactly this kind of meaningful, sustained weight loss.
Berberine, by contrast, produces modest BMI reductions in clinical trials. It is not remotely in the same category as either significant weight loss or modern diabetes pharmacotherapy.
What Berberine Does Well
Its safety profile is a real advantage. Studies have not found a significant increase in hypoglycemia risk, which is a legitimate concern with several older diabetes medications. None of teh modern diabetes medications cause hypoglycemia. This includes everything from metformin, SGLT2i, GLP1 medications and many others.
The problem is that many supplements do not contain what they say they contain. Recent studies looking at supplements have found that up to 95% of supplements sold do not contain what they say tehy contain, and are often contaminated with toxic substances.
Who Might Respond, and Who Likely Won't
The data shows meaningful variation in who benefits from berberine. Patients with higher starting blood glucose and HbA1c tend to show the greatest responses. This is the case for all diabetes medications and is not unique to berberine.
Effects appear larger in women than men and more pronounced in Asian populations. Berberine also appears less effective in patients older than 60, and benefits seem to decrease at doses above 2 grams per day. Again, this is the case for all diabetes medications and is not unique to berberine. But it is worth noting.
That degree of variability, combined with the 90-day durability concern, makes it very difficult to predict who, if anyone, will see meaningful and sustained benefit.
Berberine Bottom Line
No one should be using berberine for diabetes and it is not a cure. Because it is unregulated, it's hard to know if it is even berberine or placebo effect. Many diabetes studies have shown similar results with placebo.
Berberine produces real but modest blood sugar reductions, and the evidence suggests those reductions may not be sustained beyond 90 days. Compared to the full range of options available today, including metformin, SGLT2 inhibitors with proven cardiovascular protection, GLP-1 medications that reduce HbA1c by up to 2% or more while driving substantial weight loss, and even older agents like glimepiride and insulin, berberine is not in the same conversation as a diabetes treatment.
Because the other classes of medications cause weight loss, you get real remission and regression of diabetes.
Most importantly, berberine cannot compete with weight loss itself. A patient who commits to meaningful dietary change and loses 20 to 30 lbs will almost certainly achieve far greater and more durable improvements in blood sugar than any supplement can offer, with benefits that extend well beyond blood glucose to blood pressure, lipids, inflammation, and cardiovascular risk. Metformin, SGLT2i, and GLP1s all cause significant weight loss.
If you are managing type 2 diabetes or prediabetes, the most important conversation you can have is with your physician or cardiologist, not with a supplement label. Berberine may have a place as a complementary tool in carefully selected patients. It should never substitute for the medications, lifestyle interventions, and weight management strategies that have actually been proven to work long-term.
Another problem is that supplements are not free. You may be paying $60-80 per bottle for life, when most medications are covered by insurance and are free. Medications are not contaminated and are tightly regulated and pure.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















