

Treating Diabetes In 2026: The New ADA Guidelines Explained!
May 03, 2026
The 2026 Diabetes Standards of Care: Start With Lifestyle and Metformin, Then Protect the Heart, Kidney, and Liver Early
The 2026 American Diabetes Association (ADA) Standards of Care reflect a powerful evolution in diabetes management. But before discussing SGLT2 inhibitors, GLP-1 receptor agonists, dual incretin therapies, and advanced technology, we must be clear about something foundational:
First and foremost, diabetes care begins with lifestyle intervention and metformin.
That has not changed.
What has changed is how quickly, and strategically, we add therapies that protect the cardiovascular system, kidneys, and liver.
As a cardiologist, I view this update not as a replacement of traditional care, but as an expansion of it.
ADA Diabetes Infographic Summary:
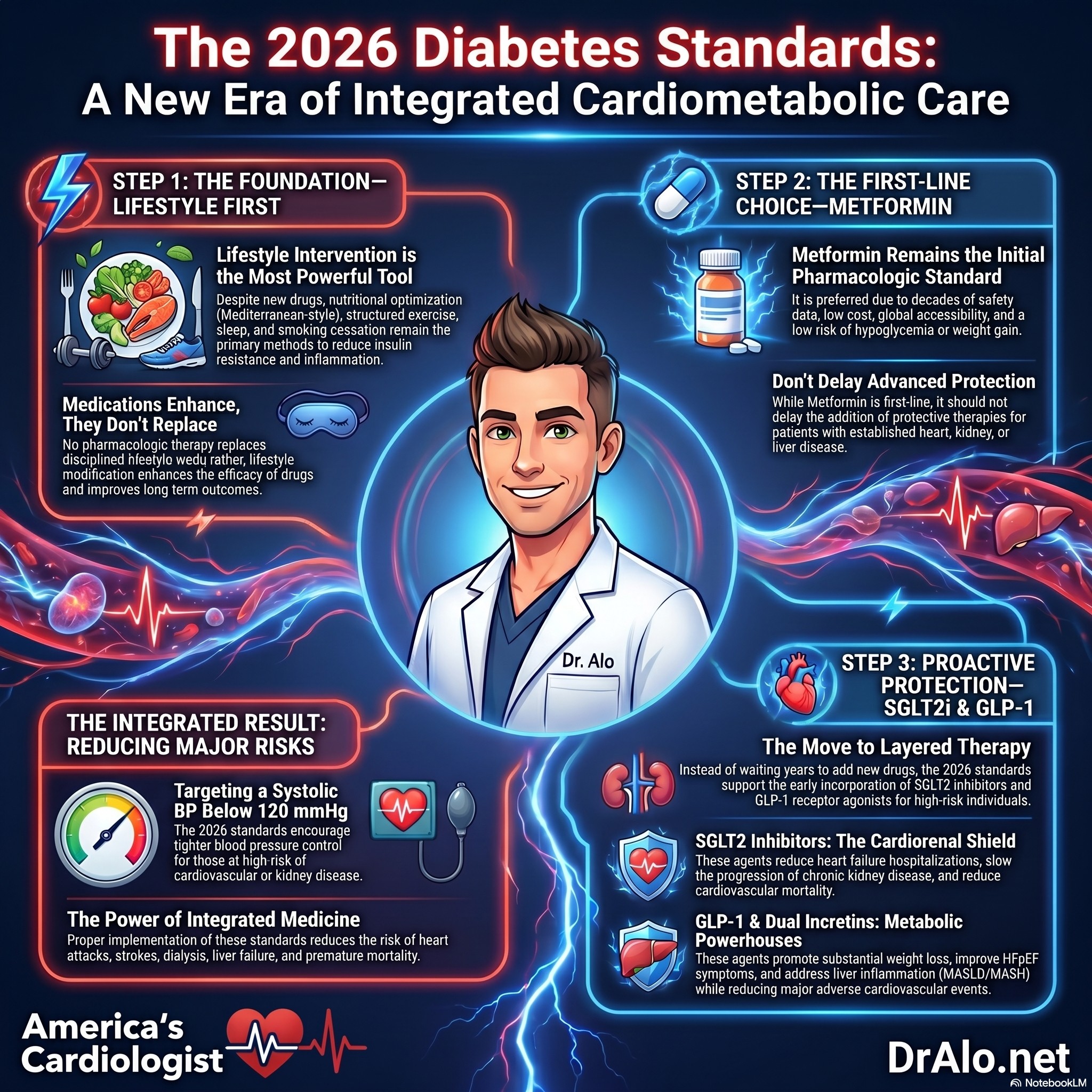
Step One: Lifestyle Is Still the Foundation
The 2026 Standards continue to emphasize intensive lifestyle intervention as first-line therapy in type 2 diabetes.
This includes:
- Nutritional optimization (Mediterranean-style, plant-forward, reduced refined carbohydrates)
- Structured aerobic and resistance training
- Weight management
- Sleep optimization
- Smoking cessation
- Blood pressure and lipid control
Lifestyle intervention remains the most powerful tool for:
- Reducing insulin resistance
- Lowering blood pressure
- Improving lipid profiles
- Reducing systemic inflammation
- Lowering cardiovascular risk
No medication replaces disciplined lifestyle work.
Even when pharmacologic therapy is required, lifestyle modification enhances drug efficacy and improves long-term outcomes.
Step Two: Metformin Remains First-Line Pharmacologic Therapy
Metformin continues to be the preferred initial medication in most patients with type 2 diabetes unless contraindicated.
It remains foundational because of:
- Decades of safety and outcome data
- Low cost and global accessibility
- Low hypoglycemia risk
- Weight neutrality or modest loss
- Favorable metabolic effects
The 2026 ADA Standards do not remove metformin from first-line therapy.
However, they recognize that for many patients, especially those with established cardiovascular disease, heart failure, chronic kidney disease, obesity, or high cardiometabolic risk, we should not delay additional protective therapies.
Step Three: Early Addition of SGLT2 Inhibitors and GLP-1 Receptor Agonists
After lifestyle optimization and metformin initiation, the 2026 guidelines support early incorporation of SGLT2 inhibitors and/or GLP-1 receptor agonists in appropriate high-risk patients.
These include individuals with:
- Established atherosclerotic cardiovascular disease
- Heart failure (particularly HFpEF)
- Chronic kidney disease
- Obesity
- Elevated cardiovascular risk
These agents are no longer viewed solely as glucose-lowering medications.
They are:
- Cardiovascular protective therapies
- Kidney protective therapies
- Weight reduction therapies
- Anti-inflammatory metabolic agents
SGLT2 Inhibitors
These medications:
- Reduce heart failure hospitalizations
- Slow chronic kidney disease progression
- Reduce cardiovascular mortality in high-risk patients
- Provide modest but meaningful glucose reduction
The 2026 Standards further clarify use across CKD stages and support combination cardiorenal protective strategies in selected patients.
GLP-1 Receptor Agonists and Dual GIP/GLP-1 Therapies
These agents:
- Promote substantial weight loss
- Reduce major adverse cardiovascular events
- Improve glycemic control
- Improve HFpEF symptoms in patients with obesity
- Demonstrate benefit in metabolic liver disease (MASLD/MASH)
The new model is layered therapy:
Lifestyle → Metformin → Add SGLT2 inhibitor and/or GLP-1 receptor agonist early when risk warrants.
Not sequential over years, but risk-stratified and proactive.
Cardiovascular and Renal Risk: More Aggressive and More Integrated
The 2026 Standards encourage tighter blood pressure control in individuals at high cardiovascular or kidney risk, supporting systolic blood pressure targets below 120 mmHg when safely achievable.
Renin–angiotensin system blockade remains foundational in albuminuric kidney disease, with expanded monitoring guidance for kidney function and potassium when combining cardiorenal agents.
For patients with type 2 diabetes and symptomatic HFpEF with obesity, incretin-based therapies are recognized for improving symptoms and reducing heart failure events.
This reinforces a fundamental truth:
Diabetes is a vascular disease accelerator.
And modern therapy must reflect that biology.
Liver Disease Moves to the Center
For patients with type 2 diabetes and metabolic dysfunction–associated steatotic liver disease (MASLD/MASH), the 2026 Standards prioritize GLP-1–based therapies with demonstrated liver benefit.
This signals an integrated cardiometabolic approach where one therapeutic class addresses:
- Weight
- Glycemia
- Liver inflammation
- Cardiovascular risk
The silos are dissolving.
Oncology and Steroid-Associated Hyperglycemia
A major practical addition in 2026 includes detailed monitoring guidance for hyperglycemia associated with:
- Immune checkpoint inhibitors
- PI3K inhibitors
- mTOR inhibitors
- High-dose or recurrent glucocorticoids
Metformin remains first-line in many cases, with insulin reserved when necessary to prevent metabolic crisis.
This reflects modern interdisciplinary medicine.
Technology Expansion: CGM and Automated Insulin Delivery
Continuous glucose monitoring is now recommended earlier and more broadly, including in older adults on insulin therapy.
Barriers to automated insulin delivery systems have been reduced, eliminating unnecessary prerequisites such as C-peptide testing.
Technology improves:
- Time in range
- Hypoglycemia reduction
- Patient engagement
- Behavioral insight
But again, it complements lifestyle and foundational pharmacology.
Lipid Therapy: Evidence-Based Simplicity
The Standards discourage adding fibrates, niacin, or dietary omega-3 supplements solely for cardiovascular risk reduction in statin-treated patients unless otherwise indicated.
The focus remains on therapies with proven cardiovascular outcome benefit.
The Big Diabetes Takeaway
The 2026 ADA Standards reinforce a layered, risk-based approach:
- Lifestyle optimization is foundational.
- Metformin remains first-line therapy in most patients.
- SGLT2 inhibitors and GLP-1 receptor agonists are added early when cardiovascular, renal, hepatic, or obesity risk is present.
This is no longer glucose-centric care.
It is integrated cardiometabolic medicine.
And when implemented properly, it has the power to reduce:
- Heart attacks
- Stroke
- Heart failure hospitalizations
- Dialysis
- Liver failure
- Premature mortality
That is the true promise of the 2026 Standards.
References
- American Diabetes Association. Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl. 1).
- American Diabetes Association. Summary of Revisions: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49 (Suppl. 1).
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















