

Why You Shouldn't Optimize For VO2 Max!
May 02, 2026
The VO2 Max Trap: Why Chasing Cardio Fitness Alone Could Be Slowly Killing Your Heart
Let me start with a picture most people in the fitness world have never questioned.
You've seen them. The elite marathon runner crossing the finish line, lean to the bone, veins threading across arms that look like they belong to someone who hasn't eaten in two weeks. The triathlete who can sustain Zone 4 heart rates for hours. The endurance cyclist with a resting heart rate of 38 beats per minute and a VO2 max that would make a cardiologist weep with envy.
The fitness industry and a significant chunk of the medical community would have you believe these people represent the pinnacle of human health. High VO2 max. Incredible aerobic engine. Pure cardiorespiratory fitness.
Here's what they don't tell you: that picture is dangerously incomplete. For a meaningful subset of people who worship at the altar of aerobic fitness, it may be setting them up for premature cardiovascular disease, overtraining, chronic injury, and an early loss of the functional independence they trained so hard to protect.
That's not clickbait. That's the science.
First: What Is VO2 Max, and Why Has It Become an Idol?
VO2 max is widely regarded as the gold standard for cardiovascular fitness. It measures the maximum rate at which your body can consume oxygen during exhaustive exercise, and it is an extraordinarily powerful predictor of health outcomes. The research is rock solid. A 2009 meta-analysis in JAMA pooled data from 33 studies and found that higher cardiorespiratory fitness is associated with 30% to 50% reductions in cardiovascular mortality and 20% to 50% reductions in all-cause mortality. Every single MET improvement in fitness is associated with a 13% to 15% reduction in all-cause mortality and cardiovascular events (Tucker et al., JACC 2022). Being unfit is a more powerful independent risk factor for coronary heart disease than smoking or diabetes.
So the relationship between aerobic fitness and cardiovascular health is real, durable, and dose-dependent up to a point. If you are coming from the couch, getting fit will extend and improve your life in ways that no medication can fully replicate.
But here is where the fitness industry and a lot of well-meaning clinicians went off the rails: they assumed that if more aerobic fitness is good, then maximum aerobic fitness must be best. They made VO2 max a destination rather than a tool. And in doing so, they ignored the full picture of what the human body actually needs to survive and thrive long-term.
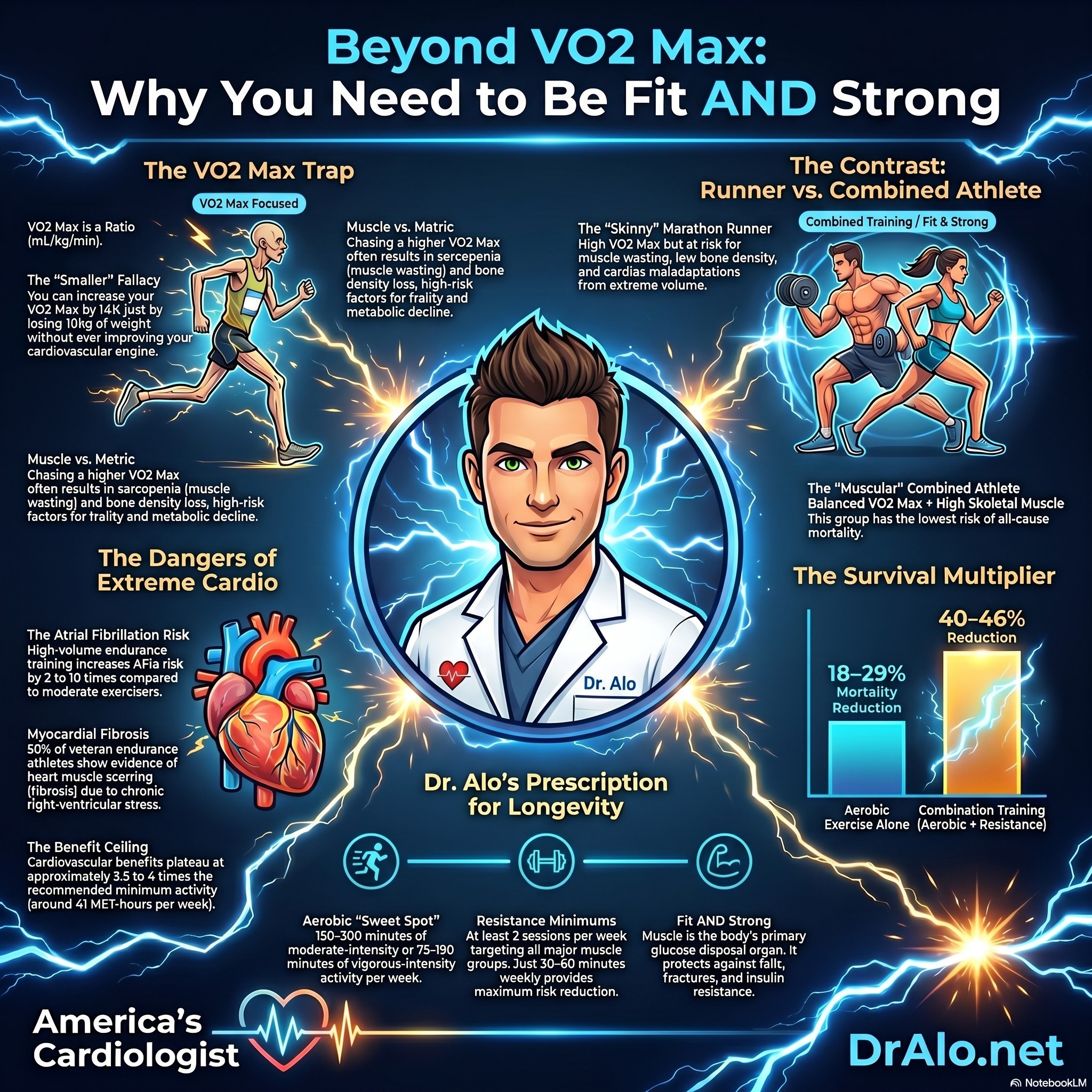
VO2 Max Infographic Summary:
The Dirty Math Secret Nobody Talks About: VO2 Max Is a Ratio
Here is the first thing I need you to understand, because it is foundational to everything else in this post.
VO2 max is not an absolute number. It is expressed as milliliters of oxygen consumed per kilogram of body weight per minute, written as mL/kg/min.
Read that again. Per kilogram of body weight.
This means that VO2 max goes up every time body weight goes down, even if actual oxygen consumption stays exactly the same. The formula is simple arithmetic:
VO2 max = Total O2 consumed (mL/min) divided by Body weight (kg)
If you consume 4,000 mL of oxygen per minute and weigh 80 kg, your VO2 max is 50 mL/kg/min. Lose 10 kg, drop to 70 kg, and that same cardiovascular engine now produces a VO2 max of 57 mL/kg/min. You improved your VO2 max by 14% without doing a single additional training session. You simply got smaller.
This is not a rounding error. This is the fundamental mathematics of the most celebrated fitness metric in cardiology and sports science.
And this is exactly why elite marathon runners have the highest VO2 max values in the world: not just because their hearts are extraordinarily efficient, but because they are extraordinarily light. Male elite marathoners frequently race at 55 to 60 kg with VO2 max values of 70 to 85 mL/kg/min. These are athletes whose training methodology explicitly involves minimizing body mass, because every kilogram they drop mathematically improves their most important performance metric.
Here is the question that should now be burning in your mind: What are they actually losing when they lose all that weight?
The answer, as we are about to see, is muscle. And that is a catastrophic trade-off for long-term health.
The Marathoner's Paradox: Highest VO2 Max, Worst Body Composition
Let's be honest about what extreme endurance training does to the human body: not what it looks like on a heart rate monitor, but what it actually does to tissue and mass.
Prolonged, high-volume aerobic training is catabolic. It is muscle-wasting by design. When you chronically deplete glycogen through aerobic exercise, prioritize caloric restriction to maintain a performance weight, and perform exercise that provides essentially no stimulus for skeletal muscle hypertrophy, your body does something very predictable: it breaks down muscle tissue. Not fat. Not bone. Skeletal muscle, the very tissue that determines your metabolic rate, your functional independence, your capacity to resist falls and fractures, your insulin sensitivity, and your long-term mortality risk.
The extreme marathon runner who weighs 58 kg with a body fat percentage of 7% is not the picture of health. They are a living example of optimizing one metric, VO2 max, while catastrophically depleting another: skeletal muscle mass.
This has a medical name. Sarcopenia, the loss of skeletal muscle mass and strength, is one of the most powerful predictors of mortality, frailty, institutionalization, and loss of independence in aging adults. Greater skeletal muscle mass in older adults is independently associated with better physical performance, mobility, and the prevention of injurious falls (Paluch et al., Circulation 2024). The person who optimizes for endurance at the expense of muscle is, paradoxically, accelerating many of the physiological hallmarks of aging.
Muscle is your body's primary glucose disposal organ. It is where insulin sensitivity lives. A person with high muscle mass who exercises moderately has vastly better glycemic control than a sarcopenic marathoner whose insulin receptors are starved of the tissue that makes them work. Resistance training alone is associated with a 17% lower incidence of type 2 diabetes compared with no resistance training (Paluch et al., Circulation 2024).
The picture becomes even starker when you consider bone. Extreme endurance athletes, especially female runners, face elevated risks of stress fractures and reduced bone mineral density, driven by low body weight, hormonal disruption from excessive training loads, and the absence of the mechanical loading stimulus that resistance exercise provides. VO2 max says nothing about your bones.
And it gets worse. Higher training volumes are consistently linked to increased musculoskeletal injury risk. Stress fractures, tendinopathies, and patellofemoral pain are common in endurance athletes, and years of high-impact training may increase the risk of osteoarthritis. The strongest and most consistent predictor of injury in endurance sport populations is total training load (Johnston et al., 2018). You cannot optimize VO2 max indefinitely without accumulating a corresponding injury debt.
The Dose-Response Curve: Where Aerobic Exercise Stops Protecting and May Start Harming
Now we get to the cardiovascular evidence, and this is where the data becomes genuinely important for anyone who has been led to believe that more aerobic exercise is always better.
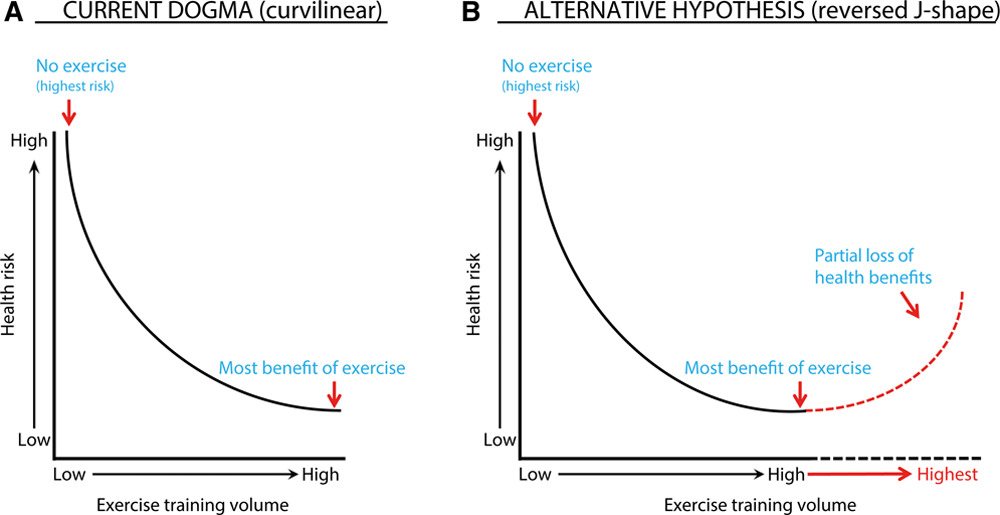
The relationship between physical activity and cardiovascular mortality has been described for decades as curvilinear: going from no exercise to moderate exercise produces the largest risk reduction, and further increases produce smaller but continued benefits. This is the prevailing dogma.
But there is a growing body of evidence supporting what researchers now call the 'extreme exercise hypothesis', that at very high volumes and intensities, aerobic exercise may paradoxically begin to increase cardiovascular risk, producing a U-shaped or reverse J-shaped curve. The partial loss of health benefits at extreme exercise volumes is documented, and a 2026 systematic review (Saulicz et al., European Journal of Epidemiology) found that while a true U-shape where extreme exercise becomes acutely harmful is not yet conclusively established, benefits clearly plateau well before the training levels most serious endurance athletes reach. The evidence for continued benefit beyond 3 to 5 times the recommended guidelines is limited at best.
The Optimal Exercise Volume: Where Is the Ceiling?
Data pooled from large epidemiological studies, including Taiwanese cohorts (Wen et al., Lancet 2011) and a massive American and European meta-analysis of 661,137 subjects (Arem et al., JAMA Internal Medicine 2015), suggest that maximal cardiovascular mortality risk reduction occurs at approximately 41 MET-hours per week of physical activity. This is approximately 3.5 to 4 times the current recommended minimum (Eijsvogels et al., JACC 2016).
That maximal benefit group experienced a 45% lower risk for cardiovascular mortality compared to inactive individuals. But here is the critical finding: individuals who exceeded this optimal volume, those performing more than 75 MET-hours per week, showed attenuated risk reduction. Their cardiovascular mortality reduction was lower than the optimal group, despite exercising significantly more.
The people doing the most exercise were getting less cardiovascular protection than the people doing the right amount of exercise.
For vigorous-intensity exercise specifically, the dose-response curve flattens even earlier, at just 11 MET-hours per week. After that point, increasing vigorous exercise volume provides no further reduction in cardiovascular mortality (Eijsvogels et al., JACC 2016). You hit the ceiling of benefit far sooner than most fitness enthusiasts realize.
For cardiac patients, the picture is even more concerning. Among 2,377 heart attack survivors in the National Runners' and Walkers' Health Studies, cardiovascular mortality decreased progressively with increasing exercise up to a volume of 38 to 50 MET-hours per week, where the mortality reduction hit 63%. But in the most active exercisers, those running more than 7.1 km per day, the reduction in CVD mortality collapsed to just 12%, statistically indistinguishable from the least active group (Williams and Thompson, Mayo Clinic Proceedings 2014). The protection had essentially vanished at extreme volumes.
When Aerobic Exercise Damages the Heart: The Four Cardinal Maladaptations
This is the part that should fundamentally change how you think about excessive endurance training. The American Heart Association issued a major 2020 scientific statement (Franklin et al., Circulation 2020) documenting four well-established potential cardiac maladaptations from high-volume, high-intensity long-term exercise training. Let me walk through each one.
1. Atrial Fibrillation: The Arrhythmia of Elite Endurance
Atrial fibrillation (AF) is the most common cardiac arrhythmia in the general population, carrying serious consequences: elevated stroke risk, increased risk of heart failure, worse cardiac mortality, and dramatically reduced quality of life.
The relationship between exercise and AF is shaped like the letter J, and not in a good way. Moderate amounts of physical activity reduce AF risk. But high-volume, high-intensity endurance training substantially increases it.
Three separate meta-analyses have found that AF risk is 2 to 10 times higher in endurance athletes compared with control subjects (Franklin et al., Circulation 2020). Men who jogged 5 to 7 times per week had a 50% higher risk of AF than men who exercised less vigorously, even after controlling for multiple cardiovascular risk factors. Long-term exercise volume exceeding 2,000 hours of training or more than 20 years of vigorous endurance training was strongly associated with increased risk of lone AF.
A nonlinear meta-regression including 19 studies and nearly 30,000 AF cases found a clear J-shaped association between physical activity volume and AF risk. Individuals performing 5 to 20 MET-hours per week had the lowest AF risk. Highly active individuals performing more than 55 MET-hours per week trended back toward elevated risk.
Why does this happen? High-volume endurance training triggers a cascade of structural, electrical, and autonomic changes in the heart. Prolonged training causes continuous left atrial enlargement and remodeling: the atria do not plateau in their structural response even when training volume stabilizes. Increased parasympathetic tone combined with atrial dilation creates the perfect substrate for chaotic electrical activity.
2. Myocardial Fibrosis: Scar Tissue in a Healthy Heart
Myocardial fibrosis, the infiltration of the heart muscle with collagen scar tissue, is something most people associate with heart attacks or end-stage heart failure. It is not supposed to appear in healthy athletes. And yet it does.
Detected using cardiac MRI with late gadolinium enhancement (LGE), multiple studies have found evidence of fibrosis in otherwise healthy endurance athletes. A systematic review of 19 studies reported LGE in 5.9% of 509 athletes examined (Franklin et al., Circulation 2020). In studies comparing competitive master endurance athletes with sedentary controls, the prevalence of LGE was 12% in athletes versus just 1.5% in controls.
More disturbing: in veteran endurance athletes who had completed the most marathons and had the longest training histories, LGE prevalence reached 50% in one study. This was dose-dependent: more years of training, more marathons completed, more fibrosis.
The fibrosis tends to appear at the insertion points of the right ventricle into the ventricular septum. During prolonged vigorous exercise, right ventricular wall stress increases by an estimated 125%, compared with just 4% for the left ventricle (Franklin et al., Circulation 2020). The thin-walled right ventricle bears the brunt.
Athletes with LGE on cardiac MRI demonstrated significantly worse event-free survival compared with those without imaging abnormalities, 75% vs. 99% in one study. Case series have documented nonsustained ventricular arrhythmias, symptomatic ventricular tachycardia, and progressive left ventricular dysfunction in athletes with subepicardial fibrosis.
3. Coronary Artery Calcification: The Calcified Paradox
Shouldn't all that aerobic exercise protect the coronary arteries? It does, but with an important caveat the fitness world has largely ignored.
Multiple studies have found that veteran endurance athletes have higher coronary artery calcium (CAC) scores than age- and risk-factor-matched sedentary controls. A Dutch study of male amateur athletes found progressively higher CAC prevalence across exercise volume tertiles: 43%, 50%, and 68% respectively, with the most active athletes carrying the highest calcium burden.
The important nuance is that not all coronary plaque is equal. Calcified (stable) plaques carry low rupture risk. Endurance athletes with higher CAC tend to have more stable calcified plaques and fewer unstable mixed plaques. Very high exercise volumes may promote plaque stabilization.
That said, this finding is not benign. It demonstrates that extreme aerobic exercise accelerates coronary artery atherosclerosis even if the plaque morphology is more favorable. For athletes who carry underlying risk factors or genetic predispositions, this calcification trajectory may prove clinically significant in ways that won't become apparent until decades later.
4. Cardiac Troponin Release and Post-Exercise Dysfunction
After endurance events such as marathons, triathlons, and ultramarathons, exercise-induced elevations in cardiac troponin T and I are nearly universal. In more than 50% of athletes competing in endurance events, post-exercise troponin concentrations exceed the upper reference limit used to diagnose acute myocardial infarction (Eijsvogels et al., JACC 2016). Concentrations rise with increasing race distance and exercise intensity.
Post-exercise decreases in both left and right ventricular function are documented, with the right ventricle showing the larger functional decrement. This 'cardiac fatigue' typically resolves within 48 hours, but in athletes who train through it repeatedly over years and decades, the cumulative stress may leave permanent marks in the form of the fibrosis and arrhythmias described above.
The Right Ventricular Problem Nobody Discusses
The right ventricle is thin-walled and designed for low-pressure work. During prolonged vigorous exercise, pulmonary vascular resistance rises, forcing the right ventricle to dramatically increase its work output. Animal studies have documented myocardial fibrosis specifically in the right ventricle after chronic endurance exercise training, accompanied by myofiber disarray, leukocyte infiltration, and pro-inflammatory markers (Franklin et al., Circulation 2020).
The pattern of cardiac stress in extreme endurance athletes, primarily affecting the right ventricle and the atria, mirrors arrhythmogenic right ventricular cardiomyopathy (ARVC), an inherited condition. It is now well established that exercise accelerates the penetrance and clinical manifestation of ARVC in individuals with desmosomal gene mutations. Among gene carriers, those who were competitive athletes were significantly more likely to meet diagnostic criteria for ARVC and had worse prognoses. The heart is telling us something important about the limits of repeated mechanical stress on specific chambers.
The Sudden Cardiac Death Reality
The relative risk of sudden cardiac death during and up to 30 minutes after vigorous exercise is transiently elevated, approximately 17-fold higher than during rest in some studies. Vigorous exercise also transiently elevates the risk of acute myocardial infarction by approximately 2 to 10-fold in the hour following exertion (Franklin et al., Circulation 2020).
The absolute risks remain very low, roughly 1 sudden cardiac death per 1.5 million episodes of vigorous exercise. But as exercise volume and competition intensity increase, so does the absolute incidence. Triathlon participation carries a higher rate of sudden cardiac death than marathon running (1.74 vs. 1.01 per 100,000 participants). The final mile of a marathon accounts for nearly 50% of sudden cardiac deaths during the race, when athletes are most physiologically compromised.
Importantly, the relative risk of exercise-induced cardiac events is dramatically higher in the least habitually active individuals who perform sudden, unaccustomed vigorous exercise. The sedentary person who decides to run a half-marathon after months of inactivity faces staggeringly higher acute risk than a trained athlete. But even among the most habitually active men, the risk of sudden cardiac death remains elevated during vigorous exertion.
Overtraining Syndrome: When More Becomes Less
One of the cruelest ironies of chasing VO2 max is that pushing too hard without adequate recovery can actually decrease it. Overtraining syndrome (OTS) is a recognized clinical condition characterized by persistent fatigue, declining performance, sleep disturbances, mood changes, and hormonal disruption. A decreased VO2 max is, paradoxically, one of its hallmark findings.
OTS represents the body's failure to adapt to a cumulative training load that has outpaced its capacity to recover. The cascade of consequences is systemic: the hypothalamic-pituitary-adrenal axis becomes dysregulated, cortisol patterns flatten, testosterone drops, sleep architecture deteriorates, and the very aerobic adaptations the athlete trained to achieve begin to reverse. The heart that was supposed to be getting stronger is now underperforming.
Recovery from OTS is not a matter of taking a rest day. It can require weeks to months of dramatically reduced training. The European College of Sport Science and the American College of Sports Medicine have issued a joint consensus statement emphasizing that prevention through periodized training and adequate recovery is far more effective than treatment after the fact (Meeusen et al., MSSE 2013).
The athlete who believes that more miles and higher intensity will always produce a higher VO2 max is operating on a model that the physiology does not support. There is a ceiling to productive stimulus, and exceeding it does not elevate fitness. It destroys it.
The Immune System Open Window
Prolonged, intense exercise temporarily suppresses several immune parameters for roughly 3 to 24 hours afterward. This period, often called the 'open window', is associated with higher rates of upper respiratory infections, particularly around major competitions and periods of heavy training load. Endurance athletes competing in ultramarathons and ironman events have well-documented higher rates of post-race illness.
That said, this picture is more nuanced than it first appears. Some researchers argue that exercise redistributes immune cells rather than truly suppressing them, and that regular moderate exercise actually enhances immune function across the lifespan (Campbell and Turner, Frontiers in Immunology 2018). The immune costs appear to be concentrated at the extreme, unrecovered end of the training spectrum.
The practical implication is straightforward: the person training at volumes that maximize VO2 max is also the person most likely to be cycling through periods of immune vulnerability. Racing weight, caloric restriction, sleep disruption from heavy training blocks, and the physiological stress of overreaching all compound the immune burden. Health is not one-dimensional. You cannot maximize one physiological system while systematically depleting others.
So What Does Protect Life? The Case for Muscle
We have established that aerobic exercise has a ceiling of benefit, that extreme endurance training carries real cardiac risks, that overtraining can reverse the very adaptations you sought, and that the joint, bone, and immune costs of extreme training loads are well documented. Now let me make the affirmative case for what the evidence actually shows preserves life, prevents frailty, and extends functional independence: the combination of cardiorespiratory fitness and skeletal muscle mass.
The 2023 American Heart Association scientific statement on resistance training (Paluch et al., Circulation 2024) synthesizes an extraordinary body of evidence that most cardiologists, to say nothing of the general fitness community, have not fully integrated.
Adults who participate in resistance training have approximately 15% lower risk of all-cause mortality and 17% lower risk of cardiovascular disease compared with adults who report no resistance training. Approximately 30 to 60 minutes per week of resistance training is associated with the maximum risk reduction, a remarkably modest investment. But critically, individuals who do both aerobic training and resistance training (combination training) achieve 40% to 46% lower risk of all-cause and cardiovascular mortality, substantially more than either modality alone (Paluch et al., Circulation 2024).
The person who does only aerobic exercise gets an 18% to 29% mortality reduction. The person who combines aerobic and resistance training gets a 40% to 46% reduction. The addition of resistance training, the muscle-preserving, strength-building modality that produces none of the cardiac maladaptations described above, nearly doubles the survival benefit.
Resistance training works through mechanisms entirely different from aerobic exercise. It reduces resting blood pressure. It improves glycemic control and insulin sensitivity through increased skeletal muscle GLUT4 expression. It improves lipid profiles. It reduces systemic inflammation. It improves endothelial function. It enhances sleep quality. It reduces symptoms of depression and anxiety. And it does all of this while building and preserving the most metabolically critical tissue in the human body: skeletal muscle.
For older adults specifically, resistance training is arguably the single most important form of exercise. It slows aging-related declines in muscle mass, power, strength, and function. In populations with frailty, sarcopenia, or osteoarthritis, gains in strength after resistance training meaningfully improve physical function. Greater skeletal muscle mass in older adults is independently associated with better physical performance, mobility, and prevention of injurious falls, the leading cause of chronic disability and loss of independence in the elderly (Paluch et al., Circulation 2024).
The person chasing maximum VO2 max by minimizing body weight is, with every pound of muscle they sacrifice, accelerating their own trajectory toward the very outcomes they fear most: frailty, metabolic decline, and dependence.
The Frailty Problem Is a Muscle Problem
Let me be direct about what frailty actually is, because this word gets thrown around without adequate weight.
Frailty is a clinical syndrome characterized by weakness, slow walking speed, exhaustion, low physical activity, and unintentional weight loss. It affects 10 to 15% of community-dwelling adults over 65 and rises steeply with age. Frail individuals are at dramatically higher risk for falls, fractures, hospitalization, functional dependence, and death.
The physiological substrate of frailty is, at its core, sarcopenia. The frail elder who can no longer rise from a chair without assistance, who falls and fractures a hip and never returns to independent living, did not fail because their heart was weak. Their heart may have been perfectly adequate. They failed because they had no muscle.
Now ask yourself: what does the fitness program of the extreme endurance athlete, optimized relentlessly for VO2 max, for racing weight, for maximum aerobic efficiency, do about sarcopenia prevention? Nothing. In many cases it actively accelerates it.
The marathon runner at age 55 with a VO2 max of 60 mL/kg/min and a body weight of 62 kg may have better aerobic fitness than 99% of their age group. But if their muscle mass is depleted and their strength is poor, they are not protected from the falls, fractures, metabolic decline, and loss of functional independence that will determine the last 20 years of their life. They have traded long-term resilience for short-term performance metrics.
Cardiorespiratory Fitness: Necessary But Not Sufficient
I am not arguing against aerobic fitness. I am arguing against aerobic fitness in isolation, and especially against the optimization of VO2 max as the primary or sole target.
Cardiorespiratory fitness is real, it matters enormously, and the research is unambiguous. The Cooper Clinic data showing that elite cardiorespiratory fitness is associated with an 80% reduction in mortality risk compared with the least fit individuals is one of the most compelling findings in all of preventive medicine. Getting aerobically fit is one of the most important things any person can do for their health.
But there are two critical limits.
First, aerobic fitness has a ceiling of benefit for cardiovascular mortality. The maximal risk reduction occurs at approximately 41 MET-hours per week of total physical activity, or even earlier for vigorous exercise at around 11 MET-hours per week. Beyond those volumes, the mortality benefit plateaus.
Second, aerobic fitness does not protect against the consequences of muscle loss. No VO2 max score prevents sarcopenia. No amount of running preserves bone density in the absence of loading forces and adequate nutrition. No marathon finish time prevents the metabolic disaster of insulin resistance driven by inadequate muscle mass.
The evidence consistently points in one direction: the combination of aerobic fitness and muscular strength produces far better health outcomes than either alone.
What the Research Actually Recommends
For aerobic exercise: 150 to 300 minutes per week of moderate-intensity activity (3 to 6 METs), or 75 to 150 minutes of vigorous-intensity activity (6 METs and above), provides substantial and well-documented mortality reduction. Higher volumes may provide incremental additional benefit up to approximately 41 MET-hours per week, after which benefits plateau. There is no evidence that exceeding 5 times the recommended minimum produces additional mortality benefit, and there is growing evidence that extreme volumes carry cardiac risks.
For resistance training: At least 2 sessions per week targeting all major muscle groups. As little as 30 to 60 minutes per week is associated with maximum risk reduction. Regimens of 8 to 10 exercises, performed in 1 to 3 sets of 8 to 12 repetitions at moderate intensity (40% to 60% of 1-repetition maximum), twice per week, are both evidence-based and achievable. Protein intake following resistance training sessions is essential to support muscle protein synthesis (Paluch et al., Circulation 2024).
For combination training: Both modalities together are strongly superior to either alone. Adults doing both aerobic and resistance training achieve up to 46% lower all-cause mortality risk, the highest mortality reduction associated with any exercise pattern in the literature.
What to avoid: Ultra-high-volume endurance training, more than 75 to 100+ MET-hours per week of vigorous activity sustained over years, carries documented increased risks of atrial fibrillation, myocardial fibrosis, right ventricular stress, accelerated coronary calcification, overtraining syndrome, musculoskeletal injury, and in cardiac patients specifically, a U-shaped pattern of cardiovascular mortality.
The Weight-Loss VO2 Max Trap in Practice
The rise of consumer fitness trackers and VO2 max estimation algorithms has put this metric in the hands of millions of ordinary people. And because VO2 max is expressed per kilogram of body weight, the single most reliable way to 'improve' your VO2 max score on a Garmin or Apple Watch is not to train harder: it is to lose weight.
This creates a perverse incentive. People motivated to improve their VO2 max scores may pursue caloric restriction and weight loss as a primary strategy, without understanding that what they are potentially sacrificing is the muscle mass that actually saves their lives in the long run.
This is especially dangerous in older adults, in whom muscle mass loss is already occurring as a background biological process. Every kilogram of muscle lost to excessive caloric restriction paired with high-volume endurance training is a kilogram that may never return, and whose absence will compound into frailty, metabolic dysfunction, falls, and functional decline.
Losing body fat is genuinely beneficial for health. But there is a profound difference between losing fat and losing weight. The person who follows a muscle-preserving approach, combining resistance training, adequate protein, and moderate aerobic exercise, improves their actual health outcomes across every meaningful dimension. The person who pursues maximum VO2 max by minimizing body weight through excess cardio and caloric restriction may improve a ratio on a display screen while quietly unraveling the biological infrastructure of long-term health.
The Right Framework: Fit AND Strong
What does the evidence-based ideal actually look like? It is not the extreme marathoner, depleted of muscle mass, with a VO2 max of 75 and a heart showing late gadolinium enhancement on MRI. It is not the competitive ironman triathlete with right ventricular dysfunction and paroxysmal atrial fibrillation. It is not the athlete battling overtraining syndrome six months into a training block.
It is the person who has sufficient cardiorespiratory fitness, meaning 150 to 300 minutes per week of moderate-intensity aerobic activity or the vigorous equivalent. The most dramatic health gains occur in the transition from sedentary to moderately active. You do not need to be an endurance athlete to capture these benefits.
It is the person who has meaningful skeletal muscle mass and strength, enough to preserve functional independence, protect against falls and fractures, support metabolic health, and resist the sarcopenic cascade of aging. This means resistance training at least twice weekly with progressive overload and adequate protein intake.
It is the person who maintains sufficient body weight, meaning healthy body composition with preservation of muscle tissue. Not minimum body weight. Not racing weight. Not weight optimized for VO2 max ratios.
It is the person who recovers adequately, because adaptation does not happen in the training session itself. It happens in the recovery. Periodized training, sleep, nutrition, and programmed rest days are not optional extras. They are the mechanism by which training produces its benefit.
And it is the person who does not train for extremes, meaning that recreational running, cycling, and endurance activities are performed at volumes and intensities that sit in the zone of maximal benefit, not the zone of diminishing returns and potential cardiac maladaptation.
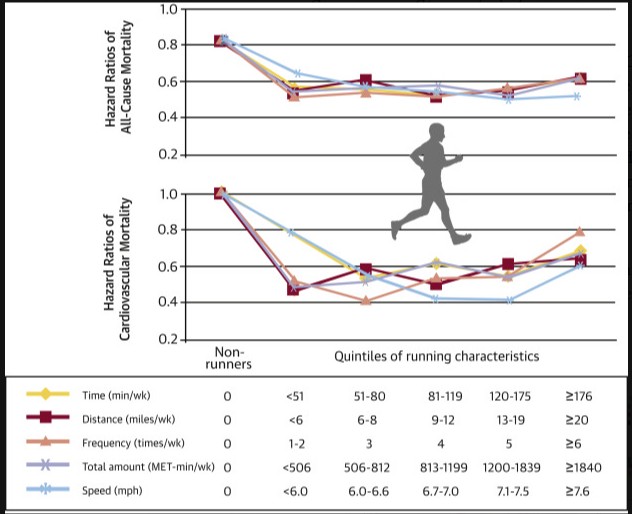
As you can see from above, compared to non-runners, all quintiles of runners did better. And they did better almost equally. Those who ran the least compared to those who ran the most had similar benefits. in fact, after a certain amount of running, the benefits started to diminish and harm began to increase.
There appears to be a certain threshold of cardiorespiratory fitness after which harm begins to increase.
A Final Word on the Shape of the Curve
The current dogma depicts a smooth curvilinear relationship between exercise volume and cardiovascular health risk, with more exercise always better. The emerging picture is more complex: benefits plateau well before the training volumes that serious endurance athletes routinely reach, and specific outcomes, particularly atrial fibrillation, show a clear J-shaped relationship where extreme exercise increases risk above the untrained baseline.
The American Heart Association's 2020 scientific statement concludes that there is currently no compelling evidence to reject the general curvilinear association for cardiovascular mortality, but explicitly acknowledges AF as an exception where the J-shaped curve is well-established. The 2026 Saulicz et al. systematic review reinforces this picture: the evidence for a true U-shaped mortality curve is currently limited, but the plateau of benefit at extreme volumes is real, and the cardiac maladaptations documented throughout this post are real regardless of what the mortality curves ultimately show.
The data on myocardial fibrosis, right ventricular remodeling, accelerated coronary calcification, overtraining syndrome, immune suppression, and musculoskeletal injury all carry the same directional signal. They all disproportionately affect the very people, extreme endurance athletes and VO2 max maximizers, who have been told they are the healthiest humans alive.
The science of exercise and longevity is not 'do more cardio.' It is 'be both fit and strong.' It is 'find the zone of optimal benefit, not the maximum dose.' It is 'train consistently, recover adequately, build muscle, protect bone, and remember that VO2 max is a ratio, and what you divide by matters as much as what is on top.'
The strongest predictor of healthy aging is not your VO2 max. It is the combination of cardiorespiratory fitness that keeps your heart and vascular system healthy, and skeletal muscle mass that keeps you functional, metabolically robust, and resistant to the frailty that steals life long before life officially ends.
Build both. Protect both. Do not sacrifice one for the other.
References
- Eijsvogels TM, Molossi S, Lee DC, Emery MS, Thompson PD. Exercise at the Extremes: The Amount of Exercise to Reduce Cardiovascular Events. J Am Coll Cardiol. 2016;67(3):316-329.
- Franklin BA, Thompson PD, Al-Zaiti SS, et al. Exercise-Related Acute Cardiovascular Events and Potential Deleterious Adaptations Following Long-Term Exercise Training: Placing the Risks Into Perspective. Circulation. 2020;141:e705-e736.
- Paluch AE, Boyer WR, Franklin BA, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update. Circulation. 2024;149:e217-e231.
- Tucker WJ, Fegers-Wustrow I, Halle M, et al. Exercise for Primary and Secondary Prevention of Cardiovascular Disease: JACC Focus Seminar 1/4. J Am Coll Cardiol. 2022;80(11):1091-1106.
- Martinez MW, Kim JH, Shah AB, et al. Exercise-Induced Cardiovascular Adaptations and Approach to Exercise and Cardiovascular Disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021;78(14):1453-1470.
- Meeusen R, Duclos M, Foster C, et al. Prevention, Diagnosis, and Treatment of the Overtraining Syndrome: Joint Consensus Statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc. 2013;45(1):186-205.
- Johnston R, Cahalan R, O'Keeffe M, O'Sullivan K, Comyns T. The Associations Between Training Load and Baseline Characteristics on Musculoskeletal Injury and Pain in Endurance Sport Populations: A Systematic Review. J Sci Med Sport. 2018;21(9):910-918.
- Campbell JP, Turner JE. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front Immunol. 2018;9:648.
- Saulicz A, Abernethy D, Wraith D. Can Too Much Exercise Kill You? A Systematic Review of the Risk of a Cardiovascular Event or Death From Long Term Strenuous Exercise. European Journal of Epidemiology. 2026.
- Arem H, Moore SC, Patel A, et al. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern Med. 2015;175:959-967.
- Williams PT, Thompson PD. Increased Cardiovascular Disease Mortality Associated With Excessive Exercise in Heart Attack Survivors. Mayo Clin Proc. 2014;89:1187-1194.
- Momma H, Kawakami R, Honda T, Sawada SS. Muscle-Strengthening Activities Are Associated With Lower Risk and Mortality in Major Non-Communicable Diseases: A Systematic Review and Meta-Analysis of Cohort Studies. Br J Sports Med. 2022;56:755-763.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















