

Do GLP1 Medications Cause Muscle Loss? 2026 Study Reveals All!
Apr 24, 2026
Are GLP-1 Medications Destroying Your Muscle? Here Is What the Research Actually Shows.
The muscle wasting narrative around Ozempic and Wegovy has been everywhere. A 2026 study in Cell Reports Medicine just put it to the test with four preclinical studies and a human clinical trial.
If you or someone you love is taking semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro, Zepbound), or any other GLP-1 based medication for weight loss, you have almost certainly heard some version of this warning: "These drugs are melting away your muscle."
It has been all over social media. Trainers are saying it. Some physicians are saying it. Supplement companies are absolutely loving it because it gives them an excuse to sell you protein powder and creatine "to protect your gains" while you are on these medications.
As the number one prescriber in the country of every GLP1 medication, I can say that I have the most experience with these medications. I can speak from experience, as well as the science, studies, and data.
I am going to do what I always do: take you directly to the data.
A March 2026 paper published in Cell Reports Medicine by Langer, Baar, and colleagues is the most comprehensive preclinical and clinical assessment of GLP-1 medicines and skeletal muscle published to date. Four preclinical studies in obese mice. One proof-of-concept clinical trial in patients with obesity and type 2 diabetes. Direct measurements of muscle mass, muscle strength, running performance, and even molecular proteomic profiling of the muscle itself.
Here is what they found, and here is what it means for your patients and for you.
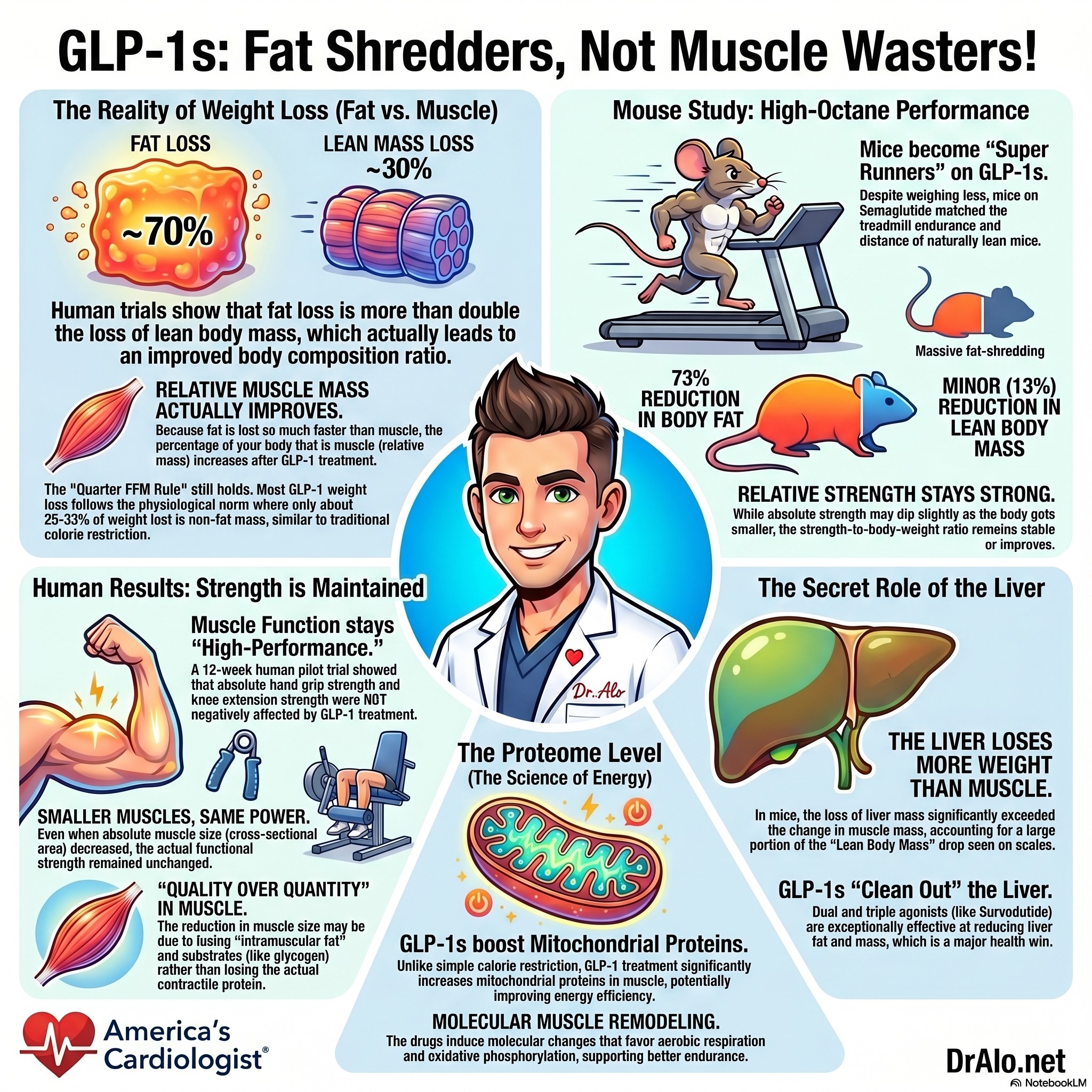
GLP1 Muscle Loss Summary Infographic:
First, Let's Address the Legitimate Concern
The worry about muscle loss with GLP-1 medications is not coming from nowhere. Large-scale clinical trials with semaglutide (STEP 1) found that roughly 40% of total weight loss came from lean body mass (LBM), which is higher than the roughly 25% expected during typical physiological weight loss (the so-called "quarter fat-free mass rule"). Similar patterns were reported with the triple agonist retatrutide.
If lean body mass is dropping at a higher rate than expected, the concern makes sense on the surface. But here is where the narrative starts to fall apart when you look more carefully.
The Critical Distinction Most People Are Missing
Lean body mass (LBM) is not the same thing as skeletal muscle. LBM includes the liver, heart, bones, other organs, and even fat that resides within lean tissue compartments. A decrease in LBM does not mean your muscles are wasting. When GLP-1 medications dramatically shrink a fatty liver, that reduction gets counted as LBM loss on a standard DXA scan. This is a methodological limitation that has been misrepresented in both the scientific literature and in popular media.
What the Studies Actually Showed: Preclinical Data
Study 1: Fat and Liver Mass Drop Far Faster Than Muscle
In diet-induced obese mice treated with tirzepatide (the dual GLP-1/GIP agonist in Mounjaro and Zepbound) for 14 days, researchers found a 73% reduction in body fat and only a 13% reduction in LBM. Within that LBM reduction, liver mass dropped approximately 20% while skeletal muscle showed only modest, often non-significant changes. Of the five lower limb muscles measured, only two showed statistically significant reductions, each in the range of roughly 10%.
Critically, because fat mass was lost so much faster than muscle, the muscle-to-body-weight ratio actually improved across multiple muscle groups. Your muscles did not get smaller relative to the rest of your body. Your fat got much smaller, making muscle look proportionally larger.
Study 2: Running Performance Improved, Not Declined
This is the finding that should settle the debate for most people.
In the next set of obese mice treated with semaglutide for 28 days, researchers measured not just muscle mass but actual functional performance: grip strength, treadmill time to exhaustion, and in vivo muscle contractility. Here is what happened:
- Absolute grip strength decreased slightly with semaglutide compared to untreated obese mice.
- Relative grip strength improved (strength normalized to body weight).
- Time to exhaustion on the treadmill increased significantly in the semaglutide group, matching near-lean control performance.
- Fat mass predicted final body weight with r² = 0.90. LBM did not predict final body weight at all (r² = 0.03).
- Time to exhaustion was negatively associated with fat mass (r² = 0.91) but not with LBM (r² = 0.12).
Translation: the animals got leaner, stronger relative to their body weight, and ran better. Fat loss, not muscle loss, drove almost every meaningful functional improvement. The mice treated with GLP-1 medication were more mobile and more physically capable than the untreated obese control group.
Study 3: Immobilization Did Not Make Things Worse
Critics of GLP-1 medications sometimes argue that the real danger is for patients who are sedentary or recovering from illness, where muscle wasting is already a concern. This study directly tested that hypothesis.
Obese mice were treated with semaglutide or a GLP-1/glucagon dual agonist (survodutide) and then had one limb immobilized with a cast for 7 days. A calorie-restriction group was included as a physiological weight loss comparison.
The result: pharmacological and physiological weight loss produced nearly identical muscle mass changes during immobilization. GLP-1 medication did not accelerate disuse atrophy beyond what calorie restriction alone produced. Liver mass, on the other hand, was strongly reduced in all groups and correlated tightly with body weight change (r² = 0.71), while muscle mass in the uncasted leg was a remarkably poor predictor of body weight (r² = 0.09).
Study 4: The Muscle Proteome Story
This is the most fascinating and underreported finding in the paper. Even though GLP-1 treatment and calorie restriction produced the same body weight loss and similar muscle mass changes, the molecular environment inside the muscle was very different.
GLP-1RA treatment upregulated mitochondrial proteins in skeletal muscle of the unimmobilized leg, including proteins involved in the aerobic electron transport chain and oxidative phosphorylation. In the immobilized leg, GLP-1RA induced increases in pathways associated with the proteasome and muscle remodeling, including MUSTN1, a protein involved in myogenesis and muscle regeneration after injury.
These findings suggest that GLP-1 medications are doing something biologically distinct in muscle beyond simply causing weight loss. And importantly, skeletal muscle does not appear to have a functional GLP-1 receptor, meaning these molecular effects are being mediated through indirect signaling pathways that we do not yet fully understand. This is an active and important area of ongoing research.
The Human Clinical Trial: What Happened in Real Patients
The researchers conducted a 12-week proof-of-concept clinical trial in patients with obesity and type 2 diabetes treated with semaglutide, escalated from 0.25 mg to 1 mg weekly. Body weight, body composition, muscle size, and direct measurements of muscle strength were collected before and after treatment. This is, to my knowledge, one of the first clinical trials to directly measure both muscle mass and muscle function together in incretin-treated patients.
Here is what they found in the human patients:
- Fat-to-body-weight ratio significantly decreased.
- Lean-to-body-weight ratio significantly increased, meaning body composition improved.
- Absolute muscle cross-sectional area of the vastus lateralis decreased significantly.
- Relative muscle size (normalized to body weight) was not negatively affected.
- Maximum voluntary contraction of the knee extensors (a direct strength test): Both absolute and relative muscle strength were preserved.
- Hand grip strength: unchanged in both absolute and relative terms.
Let me be very clear about what this means clinically: patients lost significant weight and body fat, their body composition improved, and their muscle strength was fully preserved. The reduction in muscle cross-sectional area without any reduction in strength likely reflects loss of intramuscular substrate (triglycerides, glycogen) rather than contractile proteins. Other trials have confirmed robust reductions in intramuscular fat with prolonged GLP-1 treatment.
The Functional Bottom Line
In middle-aged obese patients treated with semaglutide for 12 weeks, muscle strength was completely preserved despite a reduction in muscle size. Body composition improved. Fat was lost preferentially over muscle. And the larger clinical trial evidence (STEP 9 in knee osteoarthritis patients, the SLIM LIVER study) supports the view that the disproportionately larger loss of fat relative to LBM results in improved mobility and physical function, even when absolute LBM declines.
The DXA Problem Nobody Is Talking About
One underappreciated issue in this entire debate is the limitation of the measurement tool most clinical trials use to assess body composition: dual X-ray absorptiometry (DXA).
DXA cannot distinguish between actual skeletal muscle and the fat that resides within lean tissue compartments. It cannot differentiate intramuscular triglycerides from contractile protein. It cannot accurately capture reductions in hepatic glycogen or liver fat, both of which are known to decrease dramatically with GLP-1 treatment.
When GLP-1 medications reduce intrahepatic fat and glycogen by 40 to 50% (as multiple trials have shown), DXA reads that as lean body mass loss. This is a critical methodological confounder that has been inflating the perceived muscle wasting signal in large clinical trials. The Langer et al. paper makes this point explicitly, and it deserves far more attention in the clinical discussion.
What About Long-Term Use and Stopping the Medication?
This paper is appropriately honest about its limitations. The clinical trial was 12 weeks, and it was powered as a proof-of-concept study. We need large-scale, long-duration trials with direct muscle function measurements to draw firm conclusions across broader patient populations, including those with sarcopenia, cachexia, or heart disease.
One legitimate concern the authors raise is discontinuation. Real-world data shows that over half of patients on GLP-1 medications stop treatment within one year. Repeated cycles of weight loss and regain can deteriorate body composition over time. Whether GLP-1 medications exacerbate those effects is an important unanswered question that future studies need to address.
This does not undermine the findings of this study. It means the clinical conversation should include a realistic discussion of adherence, long-term maintenance strategies, and the importance of resistance training as a complementary intervention to preserve and build muscle during pharmacological weight loss.
The Numbers at a Glance
|
Outcome / Measure |
Key Finding |
|
Fat mass reduction (tirzepatide, mice, 14 days) |
73% reduction |
|
LBM reduction (tirzepatide, mice, 14 days) |
13% reduction |
|
Muscle-to-body-weight ratio (mice) |
Improved significantly |
|
Treadmill performance (semaglutide mice) |
Near-lean control levels |
|
Fat mass as predictor of body weight |
r² = 0.90 (strong) |
|
LBM as predictor of body weight |
r² = 0.03 (essentially none) |
|
Muscle atrophy during immobilization |
Similar to calorie restriction |
|
Muscle strength in human patients (12 weeks) |
Fully preserved |
|
Body composition in human patients |
Improved (fat:BW down, LBM:BW up) |
What Should Clinicians and Patients Actually Do?
This is not a paper that says GLP-1 medications are perfect and muscle loss is a myth. It is a paper that says the muscle loss is real but not disproportionate, not pathological, and not a reason to avoid these medications. Here is my clinical translation:
- Do not stop GLP-1 medications out of fear of muscle wasting. The current evidence does not support that concern for middle-aged patients with obesity. The functional data, including strength and mobility, consistently improves or is preserved.
- Do add resistance training. This is good advice regardless of medication status. Maintaining muscle protein synthesis during a caloric deficit is always beneficial, and resistance training has well-established cardiovascular benefits that I write about regularly.
- Prioritize protein intake. During significant caloric restriction, ensuring adequate dietary protein (at minimum 1.2 to 1.6 grams per kilogram of body weight) supports muscle preservation and complements the favorable body composition changes these medications produce.
- Be skeptical of supplement marketing. If you are seeing ads for "muscle-sparing" supplements specifically targeting GLP-1 users, apply significant skepticism. The data does not support a crisis that requires a proprietary solution.
- Monitor muscle function, not just weight. Grip strength, walking speed, and functional performance are clinically more meaningful than absolute LBM numbers from a DXA scan. Ask your clinician about these measures if you are on long-term therapy.
Dr. Alo's Clinical Bottom Line
GLP-1 medicines cause a mild reduction in absolute muscle mass as part of the overall weight loss process. This is not disproportionate. It is not pathological. Fat and liver mass are lost far more rapidly than skeletal muscle. Muscle strength is preserved. Running performance improves. Body composition gets better. The tools we use to measure lean mass in clinical trials (DXA) likely overestimate the muscle component of LBM loss because they cannot distinguish liver and muscle substrate changes from actual contractile protein loss. The muscle wasting panic around GLP-1 medications has outrun the evidence. This study brings the conversation back to the data.
References
- Langer HT, Gilmore NK, Hayden CMT, et al. Weight loss with GLP-1 medicines does not result in a disproportionate loss of muscle mass or function in obese mice and humans. Cell Reports Medicine. 2026;7:102665.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384:989-1002.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387:205-216.
- Coskun T, Wu Q, Schloot NC, et al. Effects of retatrutide on body composition in people with type 2 diabetes. Lancet Diabetes Endocrinol. 2025;13:674-684.
- Tinsley GM, Heymsfield SB. Fundamental Body Composition Principles Provide Context for Fat-Free and Skeletal Muscle Loss With GLP-1 RA Treatments. J Endocr Soc. 2024;8:bvae164.
- Prado CM, Phillips SM, Gonzalez MC, Heymsfield SB. Muscle matters: the effects of medically induced weight loss on skeletal muscle. Lancet Diabetes Endocrinol. 2024;12:785-787.
- Sattar N, Neeland IJ, Leinhard OD, et al. Tirzepatide and muscle composition changes in people with type 2 diabetes (SURPASS-3 MRI). Lancet Diabetes Endocrinol. 2025;13:482-493.
- Bliddal H, Bays H, Czernichow S, et al. Once-Weekly Semaglutide in Persons with Obesity and Knee Osteoarthritis. N Engl J Med. 2024;391:1573-1583.
- Ditzenberger GL, Lake JE, Kitch DW, et al. Effects of Semaglutide on Muscle Structure and Function in the SLIM LIVER Study. Clin Infect Dis. 2025;80:389-396.
- Nunn E, Jaiswal N, Gavin M, et al. Antibody blockade of activin type II receptors preserves skeletal muscle mass and enhances fat loss during GLP-1 receptor agonism. Mol Metab. 2024;80:101880.
- Garvey WT, Bluher M, Contreras CKO, et al. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2025;393:635-647.
- Look M, Dunn JP, Kushner RF, et al. Body composition changes during weight reduction with tirzepatide in the SURMOUNT-1 study. Diabetes Obes Metab. 2025;27:2720-2729.
- Anyiam O, Phillips B, Quinn K, et al. Metabolic effects of very-low calorie diet, semaglutide, or combination in individuals with type 2 diabetes mellitus. Clin Nutr. 2024;43:1907-1913.
Want to go deeper on GLP-1 medications and heart health?
Join the Heart 2 Heart VIP Community at dralo.net/community
America's Cardiologist | dralo.net
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















