

GLP1 Medications: Life Changing Discovery That Improves All Medical Conditions!
May 02, 2026
GLP-1 Receptor Agonists: The Most Important Drug Class of Our Lifetime?
If you have been paying attention to cardiovascular medicine over the past decade, you have watched GLP-1 receptor agonists transform from diabetes drugs into one of the most powerful multi-system therapies in modern medicine. We are no longer talking about a class that simply lowers blood sugar. We are talking about drugs that reduce heart attacks, protect the kidneys, reverse liver disease, treat sleep apnea, and may even help with addiction. The evidence base has grown to the point where ignoring it would be a disservice to every patient who walks through a cardiologist's office.
I'm not only a cardiologist, I also practice obesity medicine. I've been using modern therapeutics to help people lose wight for two decades, longer before we had GLP1 medications. GLP1s definitely has made it easier. I have thousands of patient on these medications. In fact, I am the number one prescriber of every single GLP1 medication that is available. I speak from experience with these medications, but also from data and science, because I teach other physicians how to use these medications.
As the top prescriber, I am going to walk you through the entire evidence landscape for GLP-1 receptor agonists, domain by domain, so that whether you are a patient trying to understand your options or a clinician who wants the full picture, you will leave with clarity. Let's get into it.
What Are GLP-1 Receptor Agonists?
GLP-1 stands for glucagon-like peptide-1, a hormone that your gut naturally releases after you eat. It tells your pancreas to release insulin, signals your brain that you are full, slows gastric emptying, and suppresses the glucagon that raises blood sugar. GLP-1 receptor agonists are synthetic molecules that mimic and amplify these effects, with half-lives ranging from hours to a full week depending on the formulation.
The original agents, like exenatide and liraglutide, were pioneered for blood sugar control in type 2 diabetes. But as large cardiovascular outcome trials accumulated, it became clear these drugs were doing far more than managing glucose. Today, the FDA-approved indications for this class span seven distinct clinical areas, and the investigational signals keep expanding.
The key agents you will see discussed throughout this post include:
- Semaglutide (Ozempic/Wegovy/Rybelsus): Weekly subcutaneous or once-daily oral; the most extensively studied agent in CV outcomes
- Tirzepatide (Mounjaro/Zepbound): A dual GIP/GLP-1 receptor agonist with the most potent weight loss data to date
- Liraglutide (Victoza/Saxenda): Daily injection; historically important LEADER trial data
- Dulaglutide (Trulicity): Weekly injection; REWIND trial established CV benefit in primary prevention-like populations
- Exenatide (Byetta, Bydureon): Once a day injection.
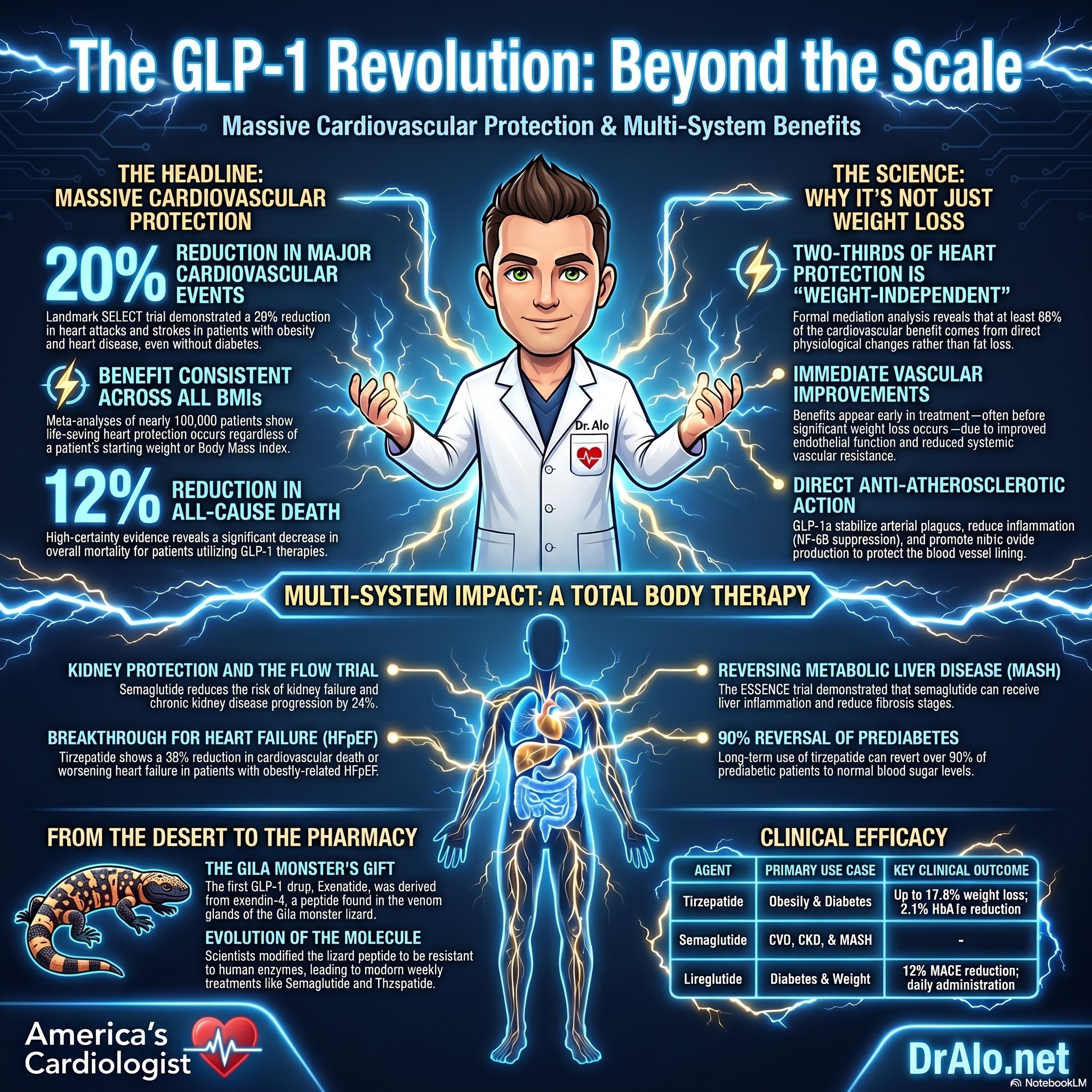
GLP1 Summary Infographic:
The Origin Story: From a Venomous Lizard in the Arizona Desert
Before we get into the clinical data, I want to take a moment to tell you where these drugs actually came from, because the story is one of the most fascinating in all of pharmacology. It begins not in a laboratory, but in the Sonoran Desert, with one of the most unusual animals in North America: the Gila monster.
The Gila monster (Heloderma suspectum) is a venomous lizard native to the southwestern United States and northwestern Mexico, particularly Arizona, New Mexico, Nevada, and Utah. It is one of only two venomous lizards native to North America. What makes the Gila monster biologically peculiar, beyond its venom, is its eating behavior. It feeds infrequently, sometimes only three to four times a year, consuming large prey items and then essentially doing very little for extended periods. Despite eating so rarely, it maintains blood sugar regulation in a way that intrigued scientists.
In the 1980s, endocrinologist Dr. John Eng at the Veterans Affairs Medical Center in New York became interested in the biology of the Gila monster's venom. Working with specimens collected from the desert, he began analyzing the proteins present in the venom glands. What he discovered changed medicine forever.
Dr. Eng identified a peptide in the venom that bore a striking structural resemblance to a human gut hormone called GLP-1. This peptide, which he named exendin-4, was approximately 53% identical in amino acid sequence to human GLP-1, but with one critical difference: while human GLP-1 is degraded by an enzyme called DPP-4 within minutes of being released, exendin-4 was resistant to that breakdown. In the Gila monster, this likely evolved as a mechanism to sustain satiety signals after large, infrequent meals. The lizard essentially has a built-in long-acting GLP-1 system.
Dr. Eng received a patent for exendin-4 in 1996. The pharmaceutical company Amylin Pharmaceuticals licensed the compound and spent years developing it into a drug suitable for human use. The result, after nearly two decades of development, was exenatide (Byetta), which received FDA approval in April 2005 as the first GLP-1 receptor agonist approved for clinical use. From desert lizard venom to approved medication took roughly 20 years. These medications are not new, they have been around since 2005, with a robust safety record.
The journey from discovery to approval is worth dwelling on because it illustrates how counterintuitive pharmacological breakthroughs can be. Nobody sat down and said we should look for diabetes drugs in lizard venom. Dr. Eng was following basic scientific curiosity about an unusual biological system. The lesson is that nature has been running biochemical experiments for hundreds of millions of years, and sometimes what evolves in a desert reptile turns out to be exactly what humans need.
Exenatide itself was a twice-daily injection with a relatively short duration of action. But the Gila monster's biology had unlocked a new pharmacological door. Pharmaceutical chemists spent the following years designing synthetic analogs that were even more resistant to degradation, could be administered once weekly, and ultimately could be taken as a pill. Semaglutide, liraglutide, dulaglutide, and tirzepatide are all downstream descendants, pharmacologically speaking, of that lizard venom discovery in a Veterans Affairs laboratory in the 1980s.
There is also a broader scientific lesson here about the value of studying unusual biological systems. The Gila monster's long fasting periods and infrequent feeding made it an interesting research subject. Its venom, which most people would consider only a danger, turned out to contain a molecule that would eventually reduce heart attacks, protect kidneys, reverse liver disease, and help millions of people manage obesity. Science does not always follow a straight line from question to answer.
I share this story with patients not just because it is fascinating, but because it often shifts how they think about these medications. When someone hears that a drug was derived from a chemical found in lizard venom, the initial reaction can be skepticism. But when you understand the decades of rigorous science, thousands of patients enrolled in clinical trials, and the careful regulatory review that stood between that desert lizard and a prescription pad, it puts the safety and efficacy data in proper context.
Cardiovascular Benefits: The Most Robust Evidence Base
Let me start with what matters most to a cardiologist. The cardiovascular outcome data for this class is, at this point, one of the strongest evidence bases in preventive medicine.
A landmark 2025 meta-analysis published in the Journal of the American College of Cardiology pooled 21 randomized controlled trials covering 99,599 patients and found high-certainty evidence that GLP-1 receptor agonists produced:
- 12% reduction in all-cause death (IRR 0.88; number needed to treat = 121)
- 13% reduction in cardiovascular death (IRR 0.87; NNT = 170)
- 13% reduction in major adverse cardiovascular events (MACE) (IRR 0.87; NNT = 66)
- 15% reduction in myocardial infarction
- 15% reduction in heart failure hospitalization
- 9% reduction in acute kidney failure
These are not trivial numbers. A number needed to treat of 66 to prevent a MACE event is competitive with many of our most established cardiovascular therapies.
Four individual GLP-1 receptor agonists have now demonstrated MACE superiority in their dedicated cardiovascular outcome trials:
- Liraglutide: LEADER trial
- Semaglutide: SUSTAIN-6 and the landmark SELECT trial
- Dulaglutide: REWIND trial
- Albiglutide: HARMONY trial
The SELECT trial deserves special attention because it broke entirely new ground. SELECT enrolled patients without diabetes who had established cardiovascular disease and obesity, and semaglutide 2.4 mg reduced MACE by 20%. This fundamentally changed the way we think about this class. The cardiovascular benefit is not dependent on glucose lowering alone. Read that again:
20% reduction in all MACE across all BMI ranges!
Then came the SOUL trial, which demonstrated that oral semaglutide also reduces MACE by 14%, establishing that the route of administration does not blunt the cardiovascular protection.
Mechanistically, GLP-1 receptor agonists improve endothelial function, cause vasodilation, reduce systemic vascular resistance, lower blood pressure, reduce inflammation, and favorably affect lipid profiles. These are pleiotropic effects that go well beyond what you would predict from weight loss or glycemic improvement alone.
The ADA 2026 Standards of Care now recommend GLP-1 receptor agonists with demonstrated cardiovascular benefit for patients with type 2 diabetes and established ASCVD, multiple cardiovascular risk factors, or chronic kidney disease, and note that combination with SGLT2 inhibitors may provide additive benefit.
|
Trial |
Agent |
Population |
Key CV Finding |
|
LEADER |
Liraglutide |
T2D + high CV risk |
MACE reduced 13% |
|
SUSTAIN-6 |
Semaglutide SC |
T2D + high CV risk |
MACE reduced 26% |
|
SELECT |
Semaglutide 2.4 mg |
Obesity + CVD, no T2D |
MACE reduced 20% |
|
REWIND |
Dulaglutide |
T2D + CV risk |
MACE reduced 12% |
|
SOUL |
Oral semaglutide |
T2D + ASCVD/CKD |
MACE reduced 14% |
Table 1. Key GLP-1 Receptor Agonist Cardiovascular Outcome Trials
Why Do GLP-1 Medications Protect the Heart? It Is Not Just Weight Loss
This is where I want to go deeper, because I think it is one of the most clinically important and most misunderstood aspects of this entire drug class. When patients lose weight on a GLP-1 receptor agonist and their blood pressure improves and their cholesterol gets better, the easy assumption is that the cardiovascular protection is just a downstream consequence of the weight loss. The data tells a more complicated and frankly more impressive story.
An invited review in the New England Journal of Medicine stated it plainly: the positive cardiac and renal effects of GLP-1 receptor agonists are more than just improvement in ambient glucose concentrations, pointing to pleiotropic vascular actions as key contributors to the MACE reductions observed across LEADER, SUSTAIN-6, SELECT, and the other landmark trials. GLP-1 improves microvascular blood flow by increasing endothelial function, causing vasodilation, and reducing systemic vascular resistance. Blood pressure reductions occur through both direct mechanisms and indirect effects on sympathetic nervous system output, not weight loss alone.
What the SELECT Trial Mediation Analysis Revealed
The most definitive clinical evidence that cardiovascular protection is not driven by weight loss comes from a prespecified analysis of the SELECT trial, which enrolled 17,604 patients with obesity and established cardiovascular disease but no diabetes. The analysis found that early in-trial weight loss was not related to subsequent cardiovascular benefit after the first 20 weeks. Patients who lost 5% or more of body weight had essentially the same cardiovascular outcomes as patients who lost less than 5%.
A formal mediation analysis in SELECT estimated that waist circumference reduction accounted for no more than 33% of the MACE effect. The investigators concluded directly: the cardioprotective effects of semaglutide extend beyond its impact on adiposity. In plain language, at least two-thirds of the cardiovascular protection is coming from something other than fat loss.
A separate prespecified SELECT analysis confirmed that semaglutide reduced cardiovascular events irrespective of baseline HbA1c or change in HbA1c, including in normoglycemic patients and in patients who showed no glycemic improvement whatsoever. The drug protects the heart in people without diabetes, and in people whose blood sugar does not move. That rules out both weight and glucose as the primary explanation.
The Benefit Appears Before Significant Weight Loss Even Occurs
Another compelling piece of evidence is the timing of the cardiovascular benefit. In SELECT, the separation in cardiovascular event curves between semaglutide and placebo emerged early, before patients had accumulated the kind of weight loss that could plausibly explain the protection through metabolic pathways. This temporal pattern strongly suggests that rapid physiological changes, not gradual fat mass reduction, are driving at least the early component of cardiovascular risk reduction.
This has important practical implications. A patient who is not achieving dramatic weight loss on a GLP-1 receptor agonist should not be told that the drug is not working from a cardiovascular standpoint. The heart benefit and the weight loss benefit appear to operate on different timescales and through different mechanisms.
Direct Anti-Atherosclerotic and Anti-Inflammatory Effects
A landmark 2026 study published in the European Heart Journal provided some of the most direct mechanistic evidence to date. In normoglycemic, non-obese rabbits, liraglutide significantly inhibited atherosclerosis progression, with meaningful reductions in percent atheroma volume, plaque macrophage content, cathepsin activity, and systemic CRP. There was no hyperglycemia and no obesity in these animals. The drug was acting directly on the arterial wall.
In a parallel clinical cohort of 47,324 patients, GLP-1 receptor agonist use was associated with lower inflammatory biomarkers and fewer MACE events, with the benefits persisting in subgroups stratified by BMI or HbA1c. Mediation analysis confirmed that reduction in inflammatory biomarkers was a contributing pathway to cardiovascular protection. The laboratory data and the clinical data pointed in the same direction.
The proposed direct vascular mechanisms, supported by preclinical and clinical data, include the following:
- Endothelial protection: GLP-1 receptor agonists promote nitric oxide production, vasodilation, and angiogenesis while inhibiting oxidative stress in vascular endothelial cells
- Plaque stabilization: Reduced matrix metalloproteinase activity prevents fibrous cap degradation; decreased smooth muscle cell proliferation reduces neointimal formation
- Anti-inflammatory signaling: Suppression of NF-kB, reduced macrophage infiltration into plaques, and decreased secretion of IL-6, TNF-alpha, and MCP-1 from monocytes and foam cells
- Atherogenic lipid reduction: Improvements in LDL cholesterol, VLDL, triglycerides, and chylomicron remnants beyond what weight loss alone would predict
- Blood pressure reduction: Through direct vasodilation and natriuresis, independent of weight change
- Epicardial and perivascular fat reduction: This fat depot exerts direct paracrine inflammatory effects on the vascular endothelium and myocardium; shrinking it has local cardiovascular consequences that extend beyond systemic BMI reduction
|
Mechanism |
Cardiovascular Effect |
Weight-Independent? |
|
Endothelial nitric oxide production |
Vasodilation, reduced vascular resistance |
Yes |
|
NF-kB suppression |
Reduced plaque inflammation |
Yes |
|
MMP inhibition |
Plaque stabilization, reduced rupture risk |
Yes |
|
Natriuresis and vasodilation |
Blood pressure reduction |
Yes |
|
Epicardial fat reduction |
Reduced paracrine inflammation on myocardium |
Partly |
|
Atherogenic lipid reduction |
Lower LDL, VLDL, triglycerides |
Partly |
|
Weight and fat mass loss |
Metabolic risk factor improvement |
No |
Table 2. Cardiovascular Protective Mechanisms of GLP-1 Receptor Agonists and Their Independence from Weight Loss.
Does BMI Change the Cardiovascular Benefit?
The large 2025 JACC meta-analysis of 99,599 patients found consistent MACE reduction regardless of whether patients had diabetes, obesity, CKD, or heart failure. Interestingly, a subgroup interaction suggested that non-diabetic and obese patients may derive greater MI benefit than their diabetic or non-obese counterparts. This is the opposite of what you would predict if glucose lowering were the primary mechanism.
A real-world propensity-matched study of patients with type 2 diabetes added important nuance. Cardiovascular benefits including heart failure hospitalization and MACE were more pronounced in patients with BMI of 25 or above, while renal benefits were consistent across all BMI categories. This suggests that different organ-protective mechanisms may have different relationships to adiposity. The kidneys benefit through mechanisms that are largely body-weight-independent, while some cardiovascular benefit in leaner patients may be attenuated.
The Clinical Bottom Line: Do Not Stop the Drug Because Weight Loss Is Modest
When a patient returns at six months having lost only eight pounds, the instinct for both patient and physician is to question whether the medication is working. But if that patient has established cardiovascular disease, the clinical trials tell us clearly that meaningful cardiovascular protection is likely still occurring through vascular, anti-inflammatory, and hemodynamic mechanisms that are not reflected on the scale.
Weight loss is a valuable outcome and worth optimizing. But it is not the only outcome, and in patients with established atherosclerotic disease or heart failure, it may not even be the primary mechanism of benefit. The SELECT mediation analysis tells us that at least two-thirds of the MACE protection comes from something other than adiposity reduction. Evaluate the drug in the context of all its effects. Do not judge it solely by the number on a scale.
Heart Failure: A Breakthrough for HFpEF
Heart failure with preserved ejection fraction (HFpEF) has historically been one of the most frustrating conditions in cardiology. We had very few treatments that moved the needle. GLP-1 receptor agonists have changed that, particularly for patients with obesity.
The STEP-HFpEF trials evaluated semaglutide 2.4 mg in patients with obesity-related HFpEF. The results were striking. Semaglutide improved Kansas City Cardiomyopathy Questionnaire (KCCQ) scores by 7 to 8 points more than placebo, produced 13% weight loss, improved six-minute walk distance by approximately 20 meters, and reduced C-reactive protein (a marker of inflammation) by about 40%.
The SUMMIT trial took this further with tirzepatide, showing a 38% reduction in the composite of cardiovascular death or worsening heart failure (HR 0.62) in patients with HFpEF and obesity, along with a clinically meaningful 6.9-point improvement in KCCQ scores.
A pooled analysis across SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM confirmed that semaglutide consistently reduces the composite of cardiovascular death or worsening heart failure events in this population. The ADA now formally recommends GLP-1 or GIP/GLP-1 receptor agonists for reduction of heart failure events and symptoms in patients with HFpEF and obesity.
The working hypothesis is that these agents reduce the inflammatory, hemodynamic, and metabolic drivers that underpin HFpEF. Weight loss unloads the heart. Reduced inflammation improves myocardial compliance. Lower blood pressure reduces afterload. Together, these translate into real clinical benefit for patients.
Kidney Protection: The FLOW Trial Changes Practice
Chronic kidney disease (CKD) and cardiovascular disease are deeply intertwined. Patients with CKD are at dramatically elevated risk of MACE, and progressive kidney disease leads to dialysis, which carries its own enormous cardiovascular burden. Protecting the kidneys is therefore a cardiovascular imperative.
The FLOW trial was the first dedicated kidney outcomes trial for a GLP-1 receptor agonist. Semaglutide 1 mg weekly reduced the composite primary kidney outcome (defined as a 50% or greater eGFR decline, end-stage kidney disease, or kidney or cardiovascular death) by 24% (HR 0.76). This is practice-changing data.
A meta-analysis of 10 trials totaling 71,351 patients extended these findings, showing GLP-1 receptor agonists reduced the composite kidney outcome by 17% across trials. In patients with baseline eGFR below 60 mL/min per 1.73m2, a relevant and high-risk group, there were dose-dependent reductions in eGFR decline of 22 to 28%.
The mechanisms of kidney protection appear to go beyond glucose lowering. GLP-1 receptor agonists reduce albuminuria, improve endothelial function in the glomerulus, lower blood pressure, and reduce renin-angiotensin system activation. Semaglutide (Ozempic) now carries a formal FDA-approved indication for reducing the risk of sustained eGFR decline, end-stage kidney disease, and cardiovascular death in adults with type 2 diabetes and chronic kidney disease.
When you combine GLP-1 receptor agonists with SGLT2 inhibitors in patients with diabetic kidney disease, you are stacking two complementary mechanisms. The guidelines now support exactly that approach.
Blood Sugar Control: Among the Most Potent Agents We Have
GLP-1 receptor agonists were originally developed for glycemic control, and they remain among the most effective agents available for that purpose, particularly the newer long-acting formulations.
A network meta-analysis of 76 randomized controlled trials covering 39,246 patients found that tirzepatide produced the largest HbA1c reduction at negative 2.10% versus placebo, followed by semaglutide. These are not marginal improvements. In the SURPASS-2 trial, tirzepatide 15 mg was superior to semaglutide 1 mg for HbA1c reduction, with up to 46% of patients achieving near-normoglycemia (HbA1c below 5.7%).
What makes GLP-1 receptor agonists particularly appealing from a glycemic standpoint is their mechanism. They stimulate insulin secretion in a glucose-dependent fashion, meaning the insulin response is tied to actual glucose levels. This dramatically reduces the risk of hypoglycemia that plagues older sulfonylureas and insulin regimens.
Longer-acting formulations (semaglutide, dulaglutide, tirzepatide) provide greater and more sustained glucose lowering than shorter-acting agents like exenatide twice daily. The combination of potent HbA1c reduction, minimal hypoglycemia risk, and cardiovascular benefit makes these agents the preferred glucose-lowering option for most patients with type 2 diabetes.
Weight Loss: Approaching Bariatric Surgery Territory
The weight loss data for this class is genuinely remarkable. For decades, pharmacotherapy for obesity was a disappointment, offering 5 to 8% weight reduction at best. GLP-1 receptor agonists shattered that ceiling.
Here is where the key agents stand based on the best available randomized trial data:
- Tirzepatide 15 mg: Up to 17.8% weight loss at 72 weeks in non-diabetic patients; over 50% of patients achieved 20 to 25% weight reduction thresholds at 176 weeks
- Semaglutide 2.4 mg: Up to 13.9% weight loss at 68 weeks
- Liraglutide 3.0 mg: Approximately 5.8% weight loss at 26 weeks
- Retatrutide (investigational triple agonist): Up to 22.1% weight loss at 48 weeks
A meta-analysis of 47 randomized controlled trials confirmed a mean weight reduction of 4.57 kg, BMI reduction of 2.07 kg/m2, and waist circumference reduction of 4.55 cm versus placebo across all GLP-1 receptor agonists. Critically, the weight loss is predominantly from fat mass with relative preservation of lean tissue, which is exactly what you want metabolically.
From a cardiovascular perspective, meaningful weight loss at this scale produces benefits across virtually every risk factor. Blood pressure falls, triglycerides improve, HDL rises, inflammation markers decrease, and the inflammatory adipose tissue that drives atherosclerosis shrinks. These are not small effects. This is why I tell patients that treating obesity is treating cardiovascular disease.
In my practice, when we combine GLP1 medications with older generic pills, we can get even great weight loss. We are beating gastric bypass and bariatric surgery. We have patients losing hundreds of pounds. We are seeing 45-60% of total body weight lost!
|
Agent |
Dose |
Weight Loss |
Trial Duration |
|
Tirzepatide |
15 mg weekly |
Up to 17.8% |
72 weeks |
|
Semaglutide |
2.4 mg weekly |
Up to 13.9% |
68 weeks |
|
Liraglutide |
3.0 mg daily |
~5.8% |
26 weeks |
|
Retatrutide* |
12 mg weekly |
Up to 22.1% |
48 weeks |
Table 2. Weight Loss Outcomes by GLP-1/Incretin Agent. *Retatrutide is investigational and not yet FDA-approved.
Combination Weight Loss Therapy
We can combine these with older meds like:
- Phentermine
- Diethylproprion
- Naltrexone
- Topiramate
- Metformin
- Buproiprion
- SGLT2i (not generic yet)
Obstructive Sleep Apnea: A New FDA-Approved Indication
This one surprises many patients. Tirzepatide (Zepbound) is now FDA-approved for moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity. This is a significant development because OSA is extraordinarily common, underdiagnosed, and carries real cardiovascular risk through mechanisms including intermittent hypoxia, sympathetic nervous system activation, and systemic inflammation.
In two phase 3 trials, tirzepatide reduced the apnea-hypopnea index (AHI) by 20 to 24 events per hour more than placebo. Approximately 50% of patients achieved AHI reductions to levels where positive airway pressure therapy would no longer be required. A meta-analysis of 5 randomized controlled trials found that incretin-based therapies reduced AHI by 14.45 events per hour. In non-diabetic patients specifically, GLP-1 receptor agonists reduced AHI by 16.6 events per hour versus placebo.
The driving mechanism is likely weight loss, given that obesity is the primary modifiable risk factor for OSA. However, there may be additional direct effects on upper airway muscle tone and fat distribution in the pharyngeal region. Either way, treating obesity with this class of medication produces clinically meaningful improvements in sleep apnea, which then feeds back into better cardiovascular outcomes.
MASH (Metabolic Liver Disease): FDA Accelerated Approval in 2025
Metabolic dysfunction-associated steatohepatitis (MASH) is a condition where excess fat in the liver leads to inflammation and progressive fibrosis. Left untreated, it progresses to cirrhosis and liver cancer. MASH is directly tied to obesity, insulin resistance, and the same metabolic milieu that drives cardiovascular disease.
In August 2025, semaglutide (Wegovy) received FDA accelerated approval for MASH with F2 to F3 fibrosis based on the results of the ESSENCE trial. This was a phase 3 trial of 800 patients that demonstrated:
- MASH resolution without worsening fibrosis: 9% with semaglutide versus 34.3% with placebo (p<0.001)
- At least one stage of fibrosis reduction: 8% versus 22.4% (p<0.001)
- Combined MASH resolution plus fibrosis improvement: 7% versus 16.1%
- Mean weight loss: 10.5% versus 2.0%
- ALT improvement: 52% reduction versus 8% reduction
These are striking results in a disease where effective pharmacotherapy has historically been nonexistent. The AASLD now recommends identifying MASH candidates using non-invasive tests such as vibration-controlled transient elastography, MR elastography, or enhanced liver fibrosis score rather than liver biopsy, which lowers the barrier to diagnosis and treatment.
Diabetes Prevention: Near-Complete Reversal in Prediabetes
The SURMOUNT-1 extension trial followed patients with prediabetes and obesity on tirzepatide for 176 weeks. The results should reshape how we approach prediabetes management. Over 90% of tirzepatide-treated patients reverted to normoglycemia, compared with under 60% with placebo. And critically, this benefit persisted 17 weeks after drug discontinuation.
This is not just blood sugar improvement. This is disease modification. Preventing the progression from prediabetes to type 2 diabetes avoids years of glycemic damage to the vasculature, kidneys, and nerves before the diagnosis is even made. From a preventive cardiology standpoint, the earlier we intervene on metabolic disease, the better the long-term outcomes.
Emerging Areas: Addiction, Neurodegeneration, and More
The signals emerging from observational data and early trials are worth discussing, with appropriate scientific humility, because they point to a drug class that may have effects on the brain and reward system that were entirely unanticipated when these drugs were first developed.
Addiction and Substance Use: Preclinical data consistently show GLP-1 receptor agonists reduce drug intake and reward behavior across alcohol, nicotine, and opioid models. Pharmacoepidemiological studies show reduced alcohol use disorder incidence, fewer alcohol-related hospitalizations, and a striking 42 to 68% reduction in opioid overdose risk with GLP-1 receptor agonists. Multiple randomized trials are ongoing. Early data with exenatide showed a 70% increase in smoking abstinence. These are not cherry-picked findings; they represent a reproducible pattern across multiple substances and multiple study designs.
Neurodegeneration: A meta-analysis found reduced all-cause dementia incidence with GLP-1 receptor agonists. Three trials of short-acting GLP-1 receptor agonists showed slowed motor decline in Parkinson's disease, though the dedicated EVOKE trial of semaglutide for early Alzheimer's disease did not demonstrate significant benefit. The field is actively investigating whether longer-acting agents will show different results. The science here is preliminary but biologically plausible.
I want to be clear that these emerging signals are exactly that: signals. They require confirmation in well-powered randomized trials before they change clinical practice. But they suggest we are only beginning to understand the full scope of what GLP-1 receptor agonists can do.
Safety Profile: What You Actually Need to Know
No drug class with this breadth of benefit is without side effects, and intellectual honesty requires addressing them directly.
The most common adverse effects are gastrointestinal: nausea, vomiting, diarrhea, and constipation. The large 2025 meta-analysis quantified this as approximately 63% higher gastrointestinal adverse event rates compared with placebo, and gallbladder disorders were about 26% higher. These are real considerations and account for most treatment discontinuations.
What the data does not show is an increased risk of pancreatitis, pancreatic cancer, or severe hypoglycemia in large meta-analyses. This is important because those concerns dominated early discussions about this class and deterred use unnecessarily. The fear was louder than the evidence supported.
Monitoring considerations include:
- Acute kidney injury risk from dehydration in the setting of nausea and vomiting, particularly on initiation
- A class boxed warning for thyroid C-cell tumors based on rodent data; these drugs should not be used in patients with a personal or family history of medullary thyroid carcinoma or MEN2
- Rare cases of retinopathy progression in patients with pre-existing severe diabetic retinopathy, likely related to rapid glycemic improvement
- Potential drug interactions related to delayed gastric emptying, which can affect absorption of other oral medications
The practical approach is dose titration. Starting at the lowest dose and increasing slowly over months, rather than rushing to the target dose, dramatically reduces gastrointestinal side effects and improves long-term tolerability.
FDA-Approved Indications at a Glance
|
Indication |
Agent(s) |
Key Trial(s) |
Year |
|
Type 2 diabetes glycemic control |
Semaglutide, tirzepatide, dulaglutide, others |
SUSTAIN, SURPASS, REWIND |
Multiple |
|
CV risk reduction (T2D + CVD) |
Semaglutide, dulaglutide, liraglutide |
LEADER, REWIND, SOUL |
2016-2024 |
|
CV risk reduction (obesity + CVD, no T2D) |
Semaglutide (Wegovy) |
SELECT |
2024 |
|
Chronic weight management |
Semaglutide (Wegovy), tirzepatide (Zepbound) |
STEP, SURMOUNT |
2021-2023 |
|
CKD progression (T2D + CKD) |
Semaglutide (Ozempic) |
FLOW |
2024 |
|
Obstructive sleep apnea |
Tirzepatide (Zepbound) |
SURMOUNT-OSA |
2024 |
|
MASH (F2-F3 fibrosis) |
Semaglutide (Wegovy) |
ESSENCE |
2025 |
Table 3. FDA-Approved Indications for GLP-1 and GIP/GLP-1 Receptor Agonists as of 2026.
GLP1 Medication Bottom Line
GLP-1 receptor agonists are not a trend or a celebrity weight loss shortcut. They represent a genuine scientific breakthrough that has produced seven FDA-approved indications across cardiovascular disease, heart failure, chronic kidney disease, type 2 diabetes, obesity, obstructive sleep apnea, and now MASH. The cardiovascular outcome data alone, covering nearly 100,000 patients in randomized trials, places this class among the most impactful drug discoveries in modern preventive medicine.
A 2025 meta-analysis in JACC encompassing 99,599 patients demonstrated reductions in all-cause death, cardiovascular death, MACE, myocardial infarction, and heart failure hospitalization with high-certainty evidence. The SELECT trial established benefit in non-diabetic patients with obesity and CVD. The FLOW trial established kidney protection. STEP-HFpEF and SUMMIT established meaningful benefit in HFpEF. The ESSENCE trial produced a MASH indication. The SURMOUNT extension showed 90% reversion of prediabetes to normoglycemia.
What I want patients and clinicians to take away from this is that if you or your patient has obesity, established cardiovascular disease, type 2 diabetes, CKD, HFpEF, MASH, or sleep apnea, this drug class should be a serious part of the treatment conversation. The evidence is there. The indications are there. The mechanism is there.
The question is no longer whether GLP-1 receptor agonists work. The question is which patient gets which agent, at what dose, and in what combination. That is where the clinical nuance lives, and it is a conversation worth having with your physician.
References
Galli M, Benenati S, Laudani C, et al. Cardiovascular Effects and Tolerability of GLP-1 Receptor Agonists: A Systematic Review and Meta-Analysis of 99,599 Patients. Journal of the American College of Cardiology. 2025.
Rosen CJ, Ingelfinger JR. GLP-1 Receptor Agonists. New England Journal of Medicine. 2026.
American Diabetes Association Professional Practice Committee. 10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes 2026. Diabetes Care. 2026.
Nauck MA, Tuttle KR, Tschop MH, Bluher M. Glucagon-Like Receptor Agonists and Next-Generation Incretin-Based Medications: Metabolic, Cardiovascular, and Renal Benefits. Lancet. 2026.
Sanyal AJ, Newsome PN, Kliers I, et al. Phase 3 Trial of Semaglutide in Metabolic Dysfunction-Associated Steatohepatitis. New England Journal of Medicine. 2025.
Jastreboff AM, le Roux CW, Stefanski A, et al. Tirzepatide for Obesity Treatment and Diabetes Prevention. New England Journal of Medicine. 2025.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















