

LDL Causes Heart Disease. Here Is the Proof.
Apr 05, 2026
The Debate Is Over Causality Is Over! LDL Causes ASCVD!
In cardiology, there are questions that deserve nuance, and then there are questions where the science has become overwhelmingly clear. This is one of them: LDL is not just associated with atherosclerotic cardiovascular disease. LDL is a cause of it.
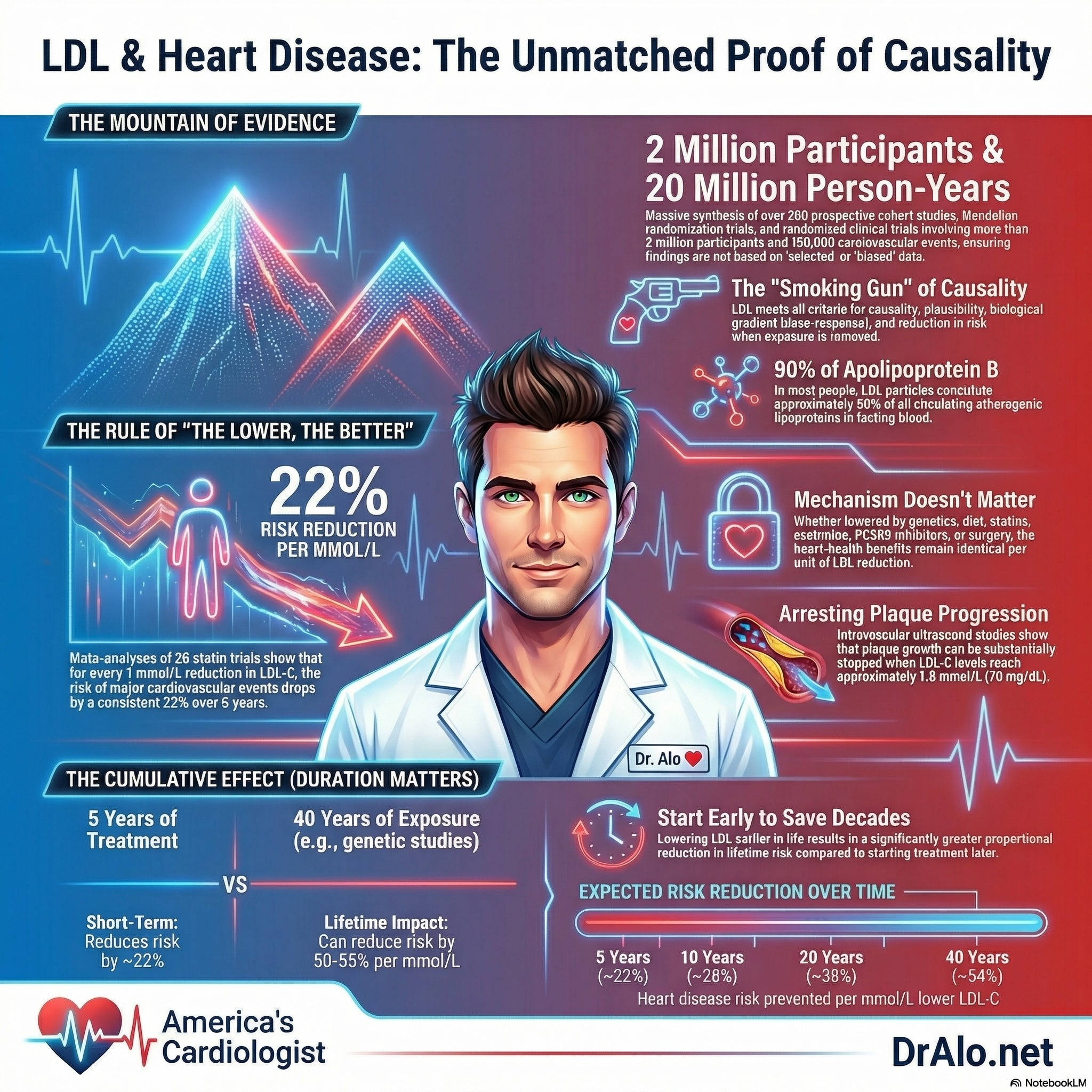
That is the central conclusion of a major European Atherosclerosis Society consensus statement that reviewed the full body of evidence across genetics, epidemiology, Mendelian randomization, and randomized clinical trials, more than 200 studies, over 2 million participants, more than 20 million person-years of follow-up, and over 150,000 cardiovascular events.
If you have ever been told your cholesterol is high, you have probably heard some version of the following: 'We need to lower your LDL.' But why? What is LDL really doing inside your arteries? And how confident are we that it is actually causing the problem, not just tagging along for the ride?
Infographic Summary:
Those are fair questions. And a landmark 2017 consensus statement published in the European Heart Journal by 30+ leading cardiologists and lipid scientists from across the world answers them with a level of rigor that I find genuinely impressive. The paper is titled 'Low-Density Lipoproteins Cause Atherosclerotic Cardiovascular Disease: Evidence from Genetic, Epidemiologic, and Clinical Studies.'
Notice the word cause. Not 'correlate with.' Not 'are associated with.' Cause. That is a very deliberate and carefully defended word in medicine.
I am going to walk you through this paper in depth because the evidence it lays out is exactly the scientific foundation behind much of what I do in clinical practice. Understanding it will help you understand why your cardiologist cares so deeply about your lipid panel, and why simply dismissing cholesterol as 'just a number' misses a critically important biological reality.
First: What Is LDL And Why Does It Matter?
LDL stands for low-density lipoprotein. It is not pure fat. It is a particle, a tiny protein-wrapped sphere that carries cholesterol through your bloodstream. Each LDL particle contains a single protein called apolipoprotein B (ApoB). Think of ApoB as the address label on a shipping container. The container is LDL. The cargo is cholesterol.
When doctors order a standard lipid panel, they typically measure LDL cholesterol (LDL-C), which reflects the total amount of cholesterol carried by all the LDL particles in your blood. Under most conditions, LDL-C is a reliable proxy for the actual number of LDL particles circulating in your body.
However, and this is important, in people with metabolic syndrome, diabetes, or high triglycerides, LDL-C can underestimate the true burden of LDL particles. In those cases, measuring ApoB directly gives you a more accurate picture of cardiovascular risk. This is exactly why I prioritize ApoB in my clinical practice. But for the purposes of this review, LDL-C is how most of the research is reported, and it is where we will focus.
At physiologically 'natural' LDL-C levels, such as what you see in newborns (typically 20 to 40 mg/dL), the risk of arterial retention of these particles is low. As LDL-C rises above that baseline, the probability that LDL particles will get trapped inside artery walls increases in a dose-dependent fashion. That is the starting point for everything that follows.
How Do We Prove Causation? The Bradford Hill Criteria
In medicine and science, proving that something causes a disease is harder than proving it is associated with it. An association can be a coincidence, a statistical artifact, or the result of a confounding variable. Causation requires a much higher bar.
The authors of this consensus statement used a modified version of the Bradford Hill criteria, a classic framework for establishing causality. These criteria include things like biological plausibility, dose-response relationships, consistency across studies, and reduction in risk when the exposure is removed.
What makes this paper so powerful is that the authors did not cherry-pick a few favorable studies. They synthesized the totality of evidence from over 200 studies involving more than 2 million participants, with over 20 million person-years of follow-up and more than 150,000 cardiovascular events. That is an enormous body of evidence.
LDL satisfied every single criterion for causality. Let me walk through the key lines of evidence.
Evidence #1: Genetics, The Natural Experiment
One of the most compelling ways to establish causation in medicine is to find a naturally occurring genetic variation that affects a single biological pathway and then observe the downstream consequences. This is sometimes called a natural experiment.
The authors point to familial hypercholesterolemia (FH), a genetic condition caused by mutations that impair LDL receptor function. The LDL receptor is responsible for clearing LDL particles from the bloodstream. When that receptor does not work well, LDL-C builds up in the blood from birth.
People with heterozygous FH (one mutated copy) typically have LDL-C levels in the range of 190 to 400 mg/dL and develop premature heart disease at a rate dramatically higher than the general population. People with homozygous FH (two mutated copies) may have LDL-C levels exceeding 500 mg/dL from childhood and can suffer heart attacks in their teens or twenties if untreated.
The reverse is also true. Rare loss-of-function mutations in PCSK9, a gene that normally degrades LDL receptors, lead to lower lifetime LDL-C levels and substantially lower rates of coronary artery disease. People with these mutations essentially walk around with the equivalent of a biological PCSK9 inhibitor built in, and their arteries show it.
Within affected families, siblings who inherit an FH mutation develop markedly elevated LDL-C and a correspondingly higher lifetime risk of cardiovascular disease compared to their unaffected siblings, who carry essentially the same diet, environment, and lifestyle. The only major difference is the gene. That is powerful evidence of causation.
Evidence #2: Mendelian Randomization, A Genetic Randomized Trial
Observational studies have limitations. Confounding variables (like diet, exercise, stress, or socioeconomic status) can muddy the waters. Randomized clinical trials overcome this, but they are expensive, short-term, and cannot ethically randomize people to high cholesterol. So how do you get unbiased causal evidence from large populations?
The answer is Mendelian randomization. At conception, genes are shuffled randomly. If you inherit a genetic variant associated with lower LDL-C, that is essentially like being randomly assigned to the 'lower LDL' group for your entire life. And importantly, this assignment happened before you were born, so it cannot be influenced by confounders like your diet or exercise habits.
Researchers have identified variants in over 50 genes that are associated with lower LDL-C. When they study people who carry these variants versus those who do not, they find a continuous, dose-dependent, log-linear relationship between lifetime LDL-C exposure and the risk of coronary heart disease.
Here is what makes this particularly compelling: when they looked at genetic variants that mimic the mechanisms of statins (the HMGCR gene), ezetimibe (the NPC1L1 gene), and PCSK9 inhibitors (the PCSK9 gene), they found that each variant reduced cardiovascular risk by essentially the same amount per unit reduction in LDL-C, regardless of the mechanism. Zero heterogeneity between them. This finding would be statistically implausible if the benefit were coming from anything other than the LDL reduction itself.
Meta-analyses of Mendelian randomization studies involving over 300,000 participants and 80,000 CHD cases confirm this. The evidence is clean, unconfounded, and consistent.
Evidence #3: Prospective Epidemiologic Studies
The authors also looked at large-scale observational cohort studies, the kind where researchers follow thousands or millions of people over many years and track who develops heart disease.
The Emerging Risk Factors Collaboration analyzed data from 302,430 people across 68 prospective studies, tracking nearly 9,800 cardiovascular events over 2.79 million person-years. The result: a log-linear, dose-dependent association between LDL-C and the risk of heart attack or coronary death
The Prospective Studies Collaboration was even larger, pooling individual data from 892,337 participants across 61 cohort studies and tracking over 33,000 ischemic heart disease deaths over nearly 12 million person-years. Again: the higher the cholesterol, the higher the risk, in a smooth, graded, consistent relationship.
These are not small, easily dismissed studies. They represent some of the largest and most rigorous epidemiologic work ever conducted in cardiovascular medicine. And they tell the same story.
Evidence #4: Randomized Clinical Trials, The Gold Standard
If genetics and epidemiology build the case, randomized controlled trials seal it.
The Cholesterol Treatment Trialists Collaboration performed a meta-analysis of 26 statin trials involving nearly 170,000 individuals. The result: for every 1 mmol/L reduction in LDL-C (roughly 39 mg/dL), there was a 22% proportional reduction in major cardiovascular events over 5 years. The benefit was consistent across every subgroup analyzed, regardless of baseline LDL-C, age, sex, or whether the person already had heart disease.
Crucially, the benefit was not just from statins. Ezetimibe, which lowers LDL by blocking intestinal cholesterol absorption (a completely different mechanism from statins), produced the exact same proportional risk reduction per unit of LDL-C lowered in the IMPROVE-IT trial and the SHARP trial. The PCSK9 inhibitor evolocumab, tested in the FOURIER trial, lowered LDL-C by about 53 mg/dL and reduced cardiovascular events by 20% over a median of 2.2 years, again consistent with the dose-response relationship predicted by the genetic and epidemiologic data.
Even old therapies like bile acid sequestrants and ileal bypass surgery showed the same pattern: lower LDL-C, fewer events, with risk reduction proportional to the magnitude of LDL-C lowering.
The implication is clear: it does not matter how you lower LDL-C. What matters is that you lower it, and by how much. The LDL particle is the problem. The mechanism is just the tool.
The Dose-Response Relationship: Lower Is Better
One of the most clinically important findings in this paper is the dose-response relationship between LDL-C and cardiovascular risk. This is not just a yes-or-no relationship. It is continuous, log-linear, and cumulative.
Intravascular ultrasound studies (which physically measure plaque inside coronary arteries) show that plaque progression can be substantially arrested when LDL-C is brought below approximately 70 mg/dL. At even lower levels, such as those achieved with high-intensity statins plus PCSK9 inhibitors, some studies show actual plaque regression, meaning the plaques shrink.
The GLAGOV trial tested this directly with evolocumab added to a statin and found plaque regression that appeared proportional to the achieved LDL-C level, even at levels as low as 36.6 mg/dL.
The authors also point out something deeply important: the cumulative burden of LDL exposure over a lifetime matters just as much as the current level. Mendelian randomization studies suggest that lifelong exposure to lower LDL-C, starting from birth, can be associated with up to three times the proportional risk reduction per unit of LDL-C compared to starting statin therapy in middle age after plaque has already developed.
This is the scientific basis for the 'lower LDL-C earlier' philosophy that guides modern preventive cardiology. The cardiovascular damage from LDL accumulates over decades. Getting ahead of it matters.
What About the LDL Skeptics?
Yes, they exist. Some physicians, journalists, and wellness influencers have argued that LDL is not really causal, that cholesterol is not the enemy, or that the entire statin-industrial complex has manufactured a problem that does not exist.
This paper addresses that skepticism directly. The authors note that most publications questioning LDL causality tend to cite individual studies or small, highly selected groups of studies without any quantitative synthesis of the overall evidence. That is selection bias masquerading as critical thinking.
When you look at the totality of evidence, from genetics to Mendelian randomization to epidemiology to randomized trials, all converging on the same log-linear, dose-dependent, cumulative relationship, the causal case is, in my view, settled science. The debate belongs in the academic margins, not in the clinic.
One notable exception the authors acknowledge is the CETP inhibitor class, where evacetrapib lowered LDL-C but did not reduce events. The authors speculate this may be due to a small increase in blood pressure, dysfunctional HDL effects, or a discordance between the LDL-C reduction and the actual LDL particle number reduction. This is an important caveat, one that reinforces the point that LDL particle number (and by extension, ApoB) is the true driver of risk, not cholesterol mass alone.
The Bottom Line: What This Means for Your Health
Here is what I want you to take away from this paper:
- LDL causes atherosclerosis. This is not a hypothesis. It is supported by the most robust, multi-layered evidence base in all of cardiovascular medicine.
- The relationship is dose-dependent and cumulative. The higher your LDL-C over your lifetime, the more plaque you develop. Every decade of elevated LDL-C adds to the burden.
- Lower LDL-C is better, regardless of mechanism. Statins, ezetimibe, PCSK9 inhibitors, diet, exercise: all roads lead to the same destination. The LDL particle is the problem.
- Starting earlier matters. Lifetime exposure to lower LDL-C, especially in high-risk individuals and those with familial hypercholesterolemia, produces far greater risk reduction than starting therapy after plaque has already accumulated.
- ApoB may be a more reliable target than LDL-C alone, especially in people with metabolic syndrome, diabetes, or high triglycerides, where LDL-C can underestimate true particle burden.
This is not about fear. It is about information. If your LDL-C is elevated, that represents a real, quantifiable, modifiable lifetime cardiovascular risk. The tools to address it have never been better, and the evidence supporting their use has never been stronger.
Talk to your cardiologist. Know your numbers. Know your ApoB. And take the evidence seriously, because it is, in every meaningful sense of the word, unequivocal.
Reference
Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. doi:10.1093/eurheartj/ehx144
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















