

Cumulative Exposure to LDL Causes Heart Disease
Apr 09, 2026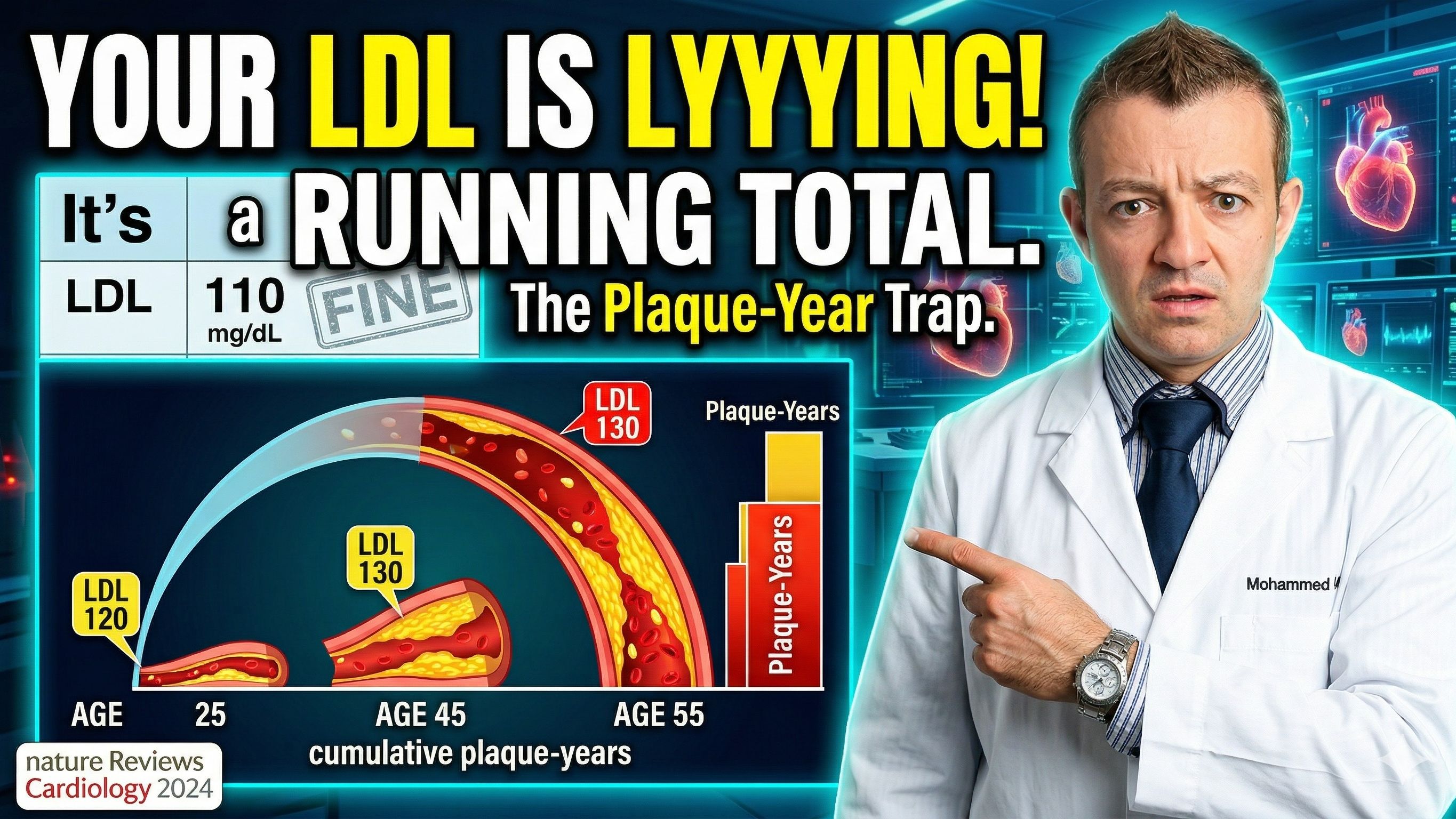
Your LDL Is Not a Snapshot. It Is a Running Total.
Let me ask you something. If your LDL came back at 110 mg/dL today, would you be worried? Most doctors would shrug. That number is not flagged. You might get a recommendation to watch your diet and come back in a year.
But here is the question your doctor is probably not asking: how long has your LDL been at 110? Or 120? Or 130? How many years has that cholesterol been quietly loading up the walls of your arteries?
That is the question that actually predicts your heart attack risk. And a landmark 2024 review published in Nature Reviews Cardiology, authored by Ference, Braunwald, and Catapano, explains exactly why. The concept is called cumulative LDL exposure, and it may be the most important reframe in cardiovascular prevention in a generation.
Let me walk you through it.
The Old Mental Model Was Wrong
For decades, we have managed cholesterol through a snapshot. You come in for your annual physical, we draw a lipid panel, we look at the LDL number today, and we make a treatment decision based on that single data point.
The problem is that atherosclerosis, the plaque buildup that causes heart attacks and strokes, is not driven by your LDL level today. It is driven by the total number of LDL particles that have crossed into your artery walls over your entire lifetime.
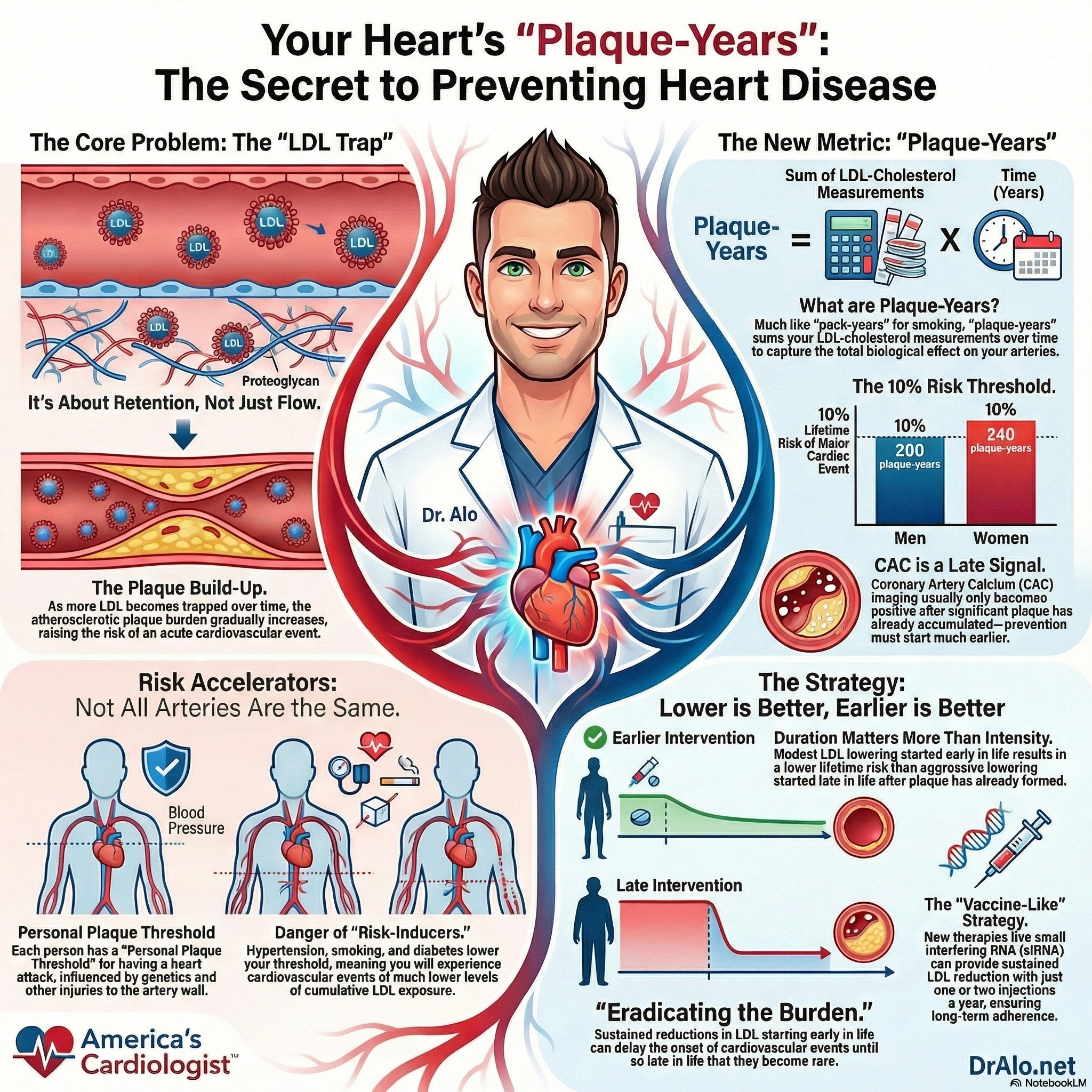
Think of it like smoking. We do not assess lung damage based on how many cigarettes you smoked this week. We use pack-years, the cumulative dose over time. The authors of this paper make exactly that analogy, proposing what they call plaque-years as the right unit of measurement for LDL exposure.
A person who has had an LDL of 140 mg/dL since age 25 has accumulated vastly more arterial damage by age 55 than someone who developed the same LDL at age 50. The same number. Completely different risk.
Infographic Summary:
How Atherosclerosis Actually Builds
Here is the biology, explained plainly.
LDL particles are small enough to cross the lining of your artery walls through a process called transcytosis. The vast majority get returned to circulation harmlessly. But a small proportion stick. They attach to proteoglycans in the artery wall and become trapped.
Once trapped, those particles trigger an inflammatory cascade. Macrophages arrive, engulf the cholesterol, and get stuck themselves. This is how plaques are born. Over years and decades, as more particles become trapped, the plaque slowly enlarges.
The plaque stays silent for a long time. Early plaque does not obstruct blood flow. It does not cause symptoms. It does not show up on most standard tests. But it is growing, year by year, particle by particle.
Eventually, when a plaque becomes large enough and unstable enough, it ruptures. The body responds by forming a clot. If that clot occludes the artery, the result is a heart attack or ischemic stroke. That is the moment most people encounter the healthcare system for the first time, long after decades of silent accumulation.
The critical insight from this paper: the risk of that clot occluding the vessel is directly proportional to the size of the disrupted plaque. Which is directly proportional to cumulative LDL exposure. Which started accumulating the day you were born.
|
The Plaque-Year Framework Cumulative LDL exposure is calculated by summing your LDL level at each age over your lifetime, the area under the curve. This is expressed in plaque-years (mmol/L or mg/dL). Among men with average LDL levels, cardiovascular event risk reaches 1% after approximately 130 plaque-years and 10% after 200 plaque-years. Among women, thresholds are higher (150 and 240 plaque-years respectively), largely because estrogen reduces LDL transcytosis into the artery wall before menopause. The Tsimane people of South America, who maintain lifetime LDL levels of 75-90 mg/dL, accumulate only about 150 plaque-years total and have a lifetime cardiovascular event risk of approximately 1%. |
Lower Is Better. And Earlier Is Far Better.
The evidence on this is unambiguous, and it comes from multiple independent lines of research.
Mendelian randomization studies are effectively nature's clinical trials. People who are born with genetic variants that naturally lower their LDL levels experience the benefit of lower LDL across their entire lifetime, starting before birth. These studies show a twofold to threefold greater reduction in cardiovascular risk for the same magnitude of LDL reduction compared to drug trials that started treatment at age 65.
That difference is not a drug effect. It is a duration effect. Starting earlier compounds.
Statin and PCSK9 inhibitor trials show the same principle playing out in real time. Both drug classes reduced major cardiovascular events by 10% in year one and 20% by year two. After 5 years of treatment, the benefit reached a 22% risk reduction per mmol/L of LDL lowered. In 15-year observational studies, that same magnitude of LDL reduction produced a 33% risk reduction. In lifetime Mendelian randomization studies, 50 to 55% risk reduction.
The longer the duration of lower LDL, the bigger the benefit. Every additional year of lower LDL matters.
|
What Happens When You Lower LDL Earlier vs. Later 25% lower LDL throughout adulthood (LDL approximately 97-104 mg/dL): reduces cumulative lifetime LDL exposure by 50 plaque-years, delays cardiovascular events by roughly 12.5 years, cuts lifetime ASCVD risk by more than half. 50% lower LDL throughout adulthood (LDL approximately 60-70 mg/dL): reduces cumulative exposure by 100 plaque-years, delays events by approximately 25 years, resulting in very low lifetime risk. More aggressive LDL lowering starting at age 55 does not match the benefit of modest LDL lowering starting at age 40. Duration beats intensity when it comes to lifetime risk reduction. |
Your Personal Plaque Threshold
One of the most important concepts in this paper is that the LDL threshold at which cardiovascular events begin to occur is not the same for everyone.
If your only cardiovascular risk factor is elevated LDL, and you have well-controlled blood pressure, no diabetes, and you do not smoke, your arteries can tolerate a higher accumulated plaque burden before a plaque rupture causes an occlusive clot. Your threshold is higher.
But add hypertension, and that threshold drops significantly. Elevated blood pressure increases LDL transcytosis into the artery wall, promotes smooth muscle cell proliferation, increases proteoglycan synthesis that traps more particles, and raises shear stress across existing plaques, making them more likely to rupture.
Add type 2 diabetes, and the threshold drops further. Chronic dysglycemia injures the artery wall and causes adverse remodeling, narrowing the coronary arteries so that even a small plaque creates significant obstruction. A thrombus in a narrowed artery is far more likely to occlude blood flow.
Smoking similarly injures the arterial wall, lowering the threshold at which plaque becomes dangerous.
The practical implication: two people with identical LDL levels and identical cumulative exposure can have completely different cardiovascular risk profiles depending on these co-exposures. This is why a 50-year-old with controlled LDL, optimal blood pressure, no diabetes, and no smoking history can carry a much lower risk than a 50-year-old with the same LDL but uncontrolled hypertension and prediabetes.
The authors frame this as your personal plaque threshold, the point at which your accumulated plaque burden, modified by other arterial wall stressors, tips from subclinical to dangerous.
But as you have seen from my other articles on here, the vast majority of people start to build plaque at an LDL cholesterol of 60 mg/dL and higher. The higher it is, the faster you build plaque. The more risk factors you have, the faster you build plaque.
CAC Scoring: Useful, But Not a Starting Gun
Many of my patients ask about coronary artery calcium scoring as a way to decide whether they need to start a statin. This paper provides an important reframe on that question.
CAC becomes non-zero at a median age of 53 years in men, at approximately 150 plaque-years of cumulative LDL exposure. At that point, the cumulative lifetime risk of major coronary events is already 2.5%. CAC scores reach 100 after roughly 210 plaque-years, at which point lifetime risk has already exceeded 10%.
Coronary calcification is a late marker. By the time calcium appears on a CT scan, decades of plaque accumulation have already occurred. The authors are explicit: lowering LDL to slow atherosclerosis progression must begin well before the CAC score becomes non-zero.
This does not mean CAC scoring is useless. It remains valuable for confirming the expected plaque burden at a given cumulative exposure level, or for recalibrating individual risk when CAC and LDL exposure are discordant. But using a CAC score of zero to justify deferring treatment in a 45-year-old with chronically elevated LDL misses the point entirely.
This is one of many reasons why I do not recommend using calcium scores. You are detecting plaque after it's too late. Often, decades too late. Why wait, when we can now prevent heart disease?
|
Why Current Guidelines Fall Short Most major guidelines recommend LDL-lowering therapy only when 10-year cardiovascular event risk exceeds a threshold (typically 7.5%-10%). This approach ignores how atherosclerosis actually develops. It encourages waiting until plaque has already accumulated enough to generate high short-term risk before intervening. The World Heart Federation 2022 Cholesterol Roadmap explicitly rejects this paradigm and instead recommends focusing on cumulative LDL reduction starting early in life. The biology supports lifetime risk as the correct frame, not 10-year risk. A 45-year-old with chronically elevated LDL and a 10-year risk of 6% may have a lifetime risk of 35% or more. |
The Vaccine Analogy and Where Treatment Is Heading
This paper introduces a concept that I find genuinely exciting as a preventive cardiologist: the possibility of a vaccine-like strategy for heart disease.
Inclisiran is a small interfering RNA (siRNA) that lowers LDL by silencing PCSK9 production in the liver. It produces a 36% time-averaged reduction in LDL with a single injection twice per year. Unlike daily pills, it essentially ensures adherence because the drug keeps working whether or not the patient remembers to take anything each day.
The vision described in this paper is administering such a therapy annually from middle adulthood onward, maintaining persistently low LDL levels over decades, accumulating fewer plaque-years, and pushing the age at which cardiovascular events would occur so far into the future that, for many people, ASCVD becomes a rare late-life event rather than the leading cause of death at 60.
This is not science fiction. The biology is established. The therapies exist. The question is whether the medical system adopts a lifetime prevention framework rather than a crisis-intervention framework.
What This Means for You Right Now
You do not need to wait for the healthcare system to adopt new guidelines to benefit from this framework. Here is how to apply it today:
- Do not treat your LDL as a single number. Ask your doctor how long your LDL has been elevated and what your estimated cumulative exposure looks like given your age and LDL trajectory.
- Earlier treatment compounds more than later, more aggressive treatment. If you are in your 30s or 40s with an LDL of 130-140 mg/dL, the evidence strongly supports discussing statin therapy now, even if your 10-year risk is below guideline thresholds.
- Control your other arterial wall stressors. Blood pressure, blood sugar, and smoking do not just add to your cardiovascular risk independently. They lower the threshold at which your accumulated plaque becomes dangerous. Optimal control of all three is as important as LDL lowering.
- ApoB is a better reflection of the number of atherogenic particles in your circulation than LDL-C alone. Ask your doctor to measure it. The cumulative exposure framework is ultimately about particle count, not cholesterol content, and ApoB captures that directly.
- Zero LDL treatment is not the goal. Very low LDL achieved with appropriate therapy is safe and protective. The evidence from FOURIER, ODYSSEY, and multiple long-term statin trials has consistently failed to identify a floor below which further LDL reduction becomes harmful.
- A CAC score of zero is not a green light to ignore LDL. It reflects plaque that has not yet calcified, not absence of plaque. Early plaque accumulation has already begun in most adults by the time calcium would appear on imaging.
LDL Exposure Bottom Line
Every year that your LDL is elevated is a year of plaque accumulation that you cannot reverse. The particles that became trapped in your artery wall at age 38 do not disappear when you start a statin at age 55. They are already there, forming the substrate for the plaque that could rupture at age 65.
The most powerful thing you can do for your long-term cardiovascular health is to start lowering LDL earlier and sustain that reduction for longer. Not because any single number today is catastrophic. But because atherosclerosis is a lifetime disease, and the window for meaningful prevention opens decades before symptoms appear.
Lower is better. And earlier is far better. The evidence has never been clearer.
If you want to understand your own cumulative LDL burden and personal plaque threshold in detail, this is exactly the kind of comprehensive cardiovascular risk conversation I have with members inside my Heart 2 Heart VIP Community. You can also register for my free longevity webinar at dralo.net/webinar.
Reference:
Ference BA, Braunwald E, Catapano AL. The LDL cumulative exposure hypothesis: evidence and practical applications. Nat Rev Cardiol. 2024. https://doi.org/10.1038/s41569-024-01039-5
https://www.nature.com/articles/s41569-024-01039-5
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















