

Young And Metabolically Healthy Still Get Heart Disease With High LDL
Apr 11, 2026
The Cholesterol Time Bomb: Why Young, Healthy People Still Get Heart Disease
Can young, healthy, metabolically pristine individuals get heart disease if all they have is high LDL? I get asked this question a lot and it has been tested and studied extensively.
What if you have no insulin resistance, very low triglycerides, high HDL, low BMI, don't smoke, and are very lean and muscular, but have high LDL cholesterol? Can you still get heart diease?
We have a lot of studies and data on this exact question.
The Myth of Invincibility
For decades, we've operated under a comforting assumption: if you're young, don't smoke, maintain normal blood pressure and blood sugar, and exercise regularly, you're protected from heart disease. Your cholesterol might be a bit elevated, say, 130 or 140 mg/dL for LDL, but that's "normal," right? Certainly nothing to worry about in your 20s or 30s.
This assumption is wrong. And the evidence proving it wrong is both compelling and sobering.
Multiple large prospective studies now demonstrate that young, otherwise healthy individuals with elevated LDL cholesterol develop atherosclerotic cardiovascular disease independent of other risk factors. More striking still: even "normal" LDL cholesterol levels, the kind that wouldn't raise eyebrows in a routine physical, contribute to atherosclerosis development over time. The disease doesn't wait until middle age to begin. It starts silently, progressively, in young adulthood.
Young & Healthy With High LDL Summary Infographic:
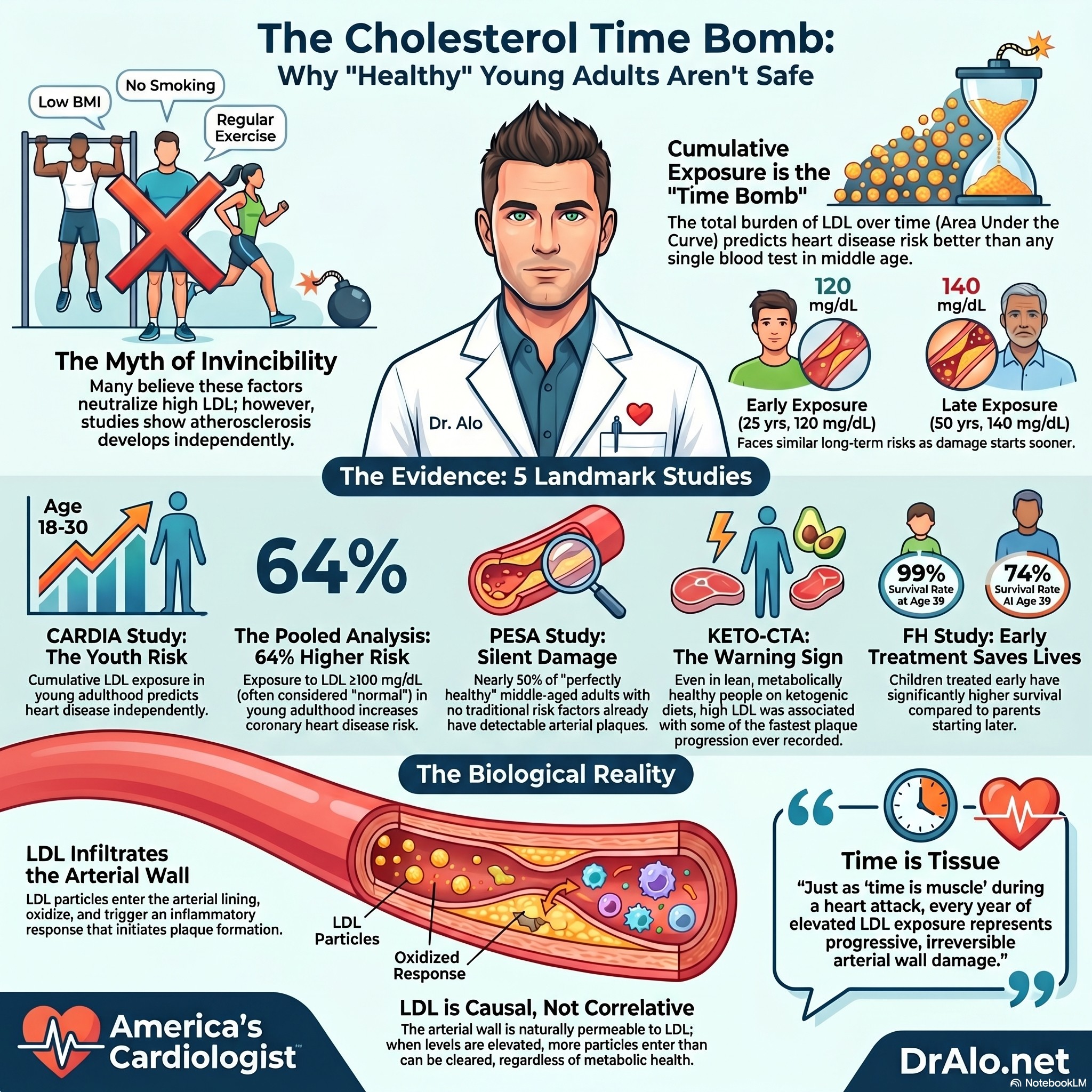
The CARDIA Study: Cumulative Exposure Matters More Than We Thought
The Coronary Artery Risk Development in Young Adults (CARDIA) study enrolled adults aged 18-30 years and followed them for a median of 16 years. The findings fundamentally changed how we understand cholesterol's role in cardiovascular disease.
Incident cardiovascular disease risk increased with cumulative LDL cholesterol exposure, calculated as the area under the LDL-C versus age curve from ages 18 to 40 years. This relationship persisted even after adjusting for other cardiovascular risk factors. In other words, the total burden of cholesterol exposure over time predicted heart disease risk independently of blood pressure, diabetes, smoking, or any other traditional risk factor.
But here's the critical insight that should change clinical practice: the same cumulative LDL cholesterol exposure reached at a younger age resulted in greater risk increase. Two people might have identical total cholesterol exposure over 20 years, but the person who accumulated that exposure earlier—say, from age 20 to 40 rather than 40 to 60—faced higher cardiovascular risk.
This finding emphasizes the profound impact of early intervention. Every year of elevated LDL cholesterol in young adulthood compounds future risk. The 2026 ACC/AHA Dyslipidemia Guidelines now explicitly recognize this, noting that CARDIA demonstrated strong associations between atherogenic lipid levels in young adults that are approximately 20 mg/dL lower for LDL-C compared with those seen in middle-aged adults with cardiovascular disease. Translation: a 25-year-old with an LDL of 120 mg/dL faces similar long-term risk as a 50-year-old with an LDL of 140 mg/dL.
The Pooled Analysis: Even "Normal" Cholesterol Isn't Safe
A pooled analysis of 36,030 participants from six U.S. cohort studies with median 17-year follow-up examined young adults aged 18-39 years. The results were unambiguous: exposure to LDL cholesterol levels ≥100 mg/dL in young adulthood was associated with a 64% increased risk of coronary heart disease (adjusted hazard ratio 1.64, 95% CI 1.27-2.11) compared with LDL-C 100 mg/dL.
Read that again. An LDL of 100 mg/dL, considered perfectly normal by conventional standards, increased heart disease risk by nearly two-thirds when that exposure occurred in young adulthood. This association persisted even after adjusting for the most recent LDL cholesterol level during middle age, demonstrating that both current LDL level and cumulative LDL burden independently contribute to coronary heart disease risk.
The implication is profound: we cannot simply wait until middle age to address cholesterol. The damage accumulates silently over decades, and by the time traditional risk calculators suggest intervention, substantial atherosclerosis has already developed.
The PESA Study: Atherosclerosis in the "Perfectly Healthy"
Perhaps the most striking evidence comes from the Progression of Early Subclinical Atherosclerosis (PESA) study. Researchers examined 1,779 middle-aged participants (mean age 45 years) without any conventional cardiovascular risk factors. These weren't people with borderline abnormalities, they had no smoking history, untreated blood pressure 140/90 mmHg, fasting glucose 126 mg/dL, total cholesterol 240 mg/dL, and LDL cholesterol 160 mg/dL.
By any conventional assessment, these individuals were at low risk. Yet subclinical atherosclerosis, detectable plaques in the carotid, aortic, iliofemoral, or coronary arteries—was present in 49.7% of them. Nearly half of "perfectly healthy" middle-aged adults already had atherosclerosis.
The researchers then examined a subgroup with optimal risk factors: blood pressure 120/80 mmHg, fasting glucose 100 mg/dL, HbA1c 5.7%, and total cholesterol 200 mg/dL. Even in this ultra-low-risk group, over one-third had subclinical atherosclerosis.
What predicted atherosclerosis in these otherwise healthy individuals? Age, male sex, and LDL cholesterol. Even when all other risk factors were at optimal levels, LDL cholesterol remained independently associated with both atherosclerosis presence and extent.
The dose-response relationship was linear and striking. Among risk factor-free individuals, atherosclerosis prevalence ranged from 11% in those with LDL cholesterol 60-70 mg/dL to 64% in those with 150-160 mg/dL (p0.001). This pattern persisted across all vascular territories examined, carotid, aortic, iliofemoral, and coronary arteries.
These findings demolish the notion that "normal" cholesterol levels are safe. LDL cholesterol, even at levels currently considered normal, drives atherosclerosis development in the absence of any other risk factors.
KETO-CTA Trial: Fastest Plaque Progression Ever Recorded
Even the controversial KETO-CTA observational study can be read as a warning, not a reassurance. In a narrowly selected group of 100 lean, metabolically healthy people on long-term ketogenic diets with very high LDL-C and ApoB, the published 1-year analysis reported a median increase in noncalcified plaque volume of 18.9 mm³. Other analysts evaluating the raw data noted a 35-45 mm³ increase in soft plaque.
In my analysis (and many others) of the same dataset, we have found that plaque growth occurred in the vast majority of participants, that some individuals who began with a coronary calcium score of 0 progressed to clearly positive calcium scores, and that the magnitude of plaque progression appeared strikingly high relative to comparator cohorts. In other words, this was not evidence that youth, leanness, high HDL, or low triglycerides somehow neutralize atherosclerosis risk; it was a reminder that young and apparently healthy people can still accumulate coronary plaque rapidly when exposure to atherogenic lipoproteins is extreme. Because the 2025 longitudinal KETO-CTA paper was later retracted over methodological problems affecting data reliability, it should be presented as controversial and hypothesis-generating rather than definitive proof.
As of note, this study was designed by proponents of a keto diet and lifestyle who designed the study to specifically show no change in plaque. Yet, it showed some of the fastest plaque accumulation ever recorded.
Even when the study design was biased toward showing that high LDL cholesterol did not matter, it showed that it mattered a lot. And that LDL was the only thing that mattered.
No Heart Disease With An LDL < 60 mg/dL
If you have been reading my blog and publications for a while, you will have run across the 60mg rule. Studies have shown that very little heart disease occurs with an LDL Cholesterol below 60 mg/dL.
This also fits the broader “LDL ~60 mg/dL” story.
Multiterritory imaging data suggest that subclinical atherosclerosis is rare to nearly absent when LDL-C is below about 60 mg/dL, then rises in a clear dose-dependent fashion above that range; in the PESA framework discussed here, atherosclerosis prevalence climbed from roughly 11% at LDL-C 60–70 mg/dL to 64% at 150–160 mg/dL.
This matters because it reframes the debate entirely: the question is not whether a young, lean, metabolically healthy person can temporarily “tolerate” an LDL of 200 or 300, but why anyone would assume those levels are benign when the broader imaging, cumulative-exposure, and outcomes literature points in the opposite direction and suggests that the biologically safer zone is far lower, closer to 60 mg/dL than to the conventional “normal” range.
The Genetic Evidence: Lifelong Exposure Matters Most
Mendelian randomization studies, which use genetic variants as natural experiments, provide perhaps the most compelling evidence for LDL cholesterol's causal role in atherosclerosis. These studies examine people born with genetic variants that result in slightly lower LDL cholesterol throughout their entire lives.
The results are remarkable: genetically mediated lower LDL cholesterol beginning early in life is associated with up to 3-fold greater reduction in coronary heart disease risk compared with shorter-term LDL cholesterol lowering started later in life through medication.
A European Atherosclerosis Society consensus statement reviewed genetic studies, prospective cohort studies, Mendelian randomization studies, and randomized trials including over 2 million participants with more than 20 million person-years of follow-up. The evidence demonstrates a consistent dose-dependent log-linear association between LDL cholesterol exposure and cardiovascular disease risk, with the effect increasing with duration of exposure.
This isn't about having extremely low cholesterol. It's about the cumulative burden over decades. A person with an LDL of 70 mg/dL from birth to age 60 faces dramatically lower cardiovascular risk than someone with an LDL of 130 mg/dL over the same period, even though 130 mg/dL is considered "normal."
The Familial Hypercholesterolemia Study: Early Treatment Changes Everything
A 20-year follow-up study of children with familial hypercholesterolemia provides the most direct evidence that early intervention saves lives. Children who started statins in adolescence (mean age 14 years) showed 99% cardiovascular disease-free survival at age 39 years. Their parents, who had the same genetic condition but didn't have statins available until adulthood, showed only 74% cardiovascular disease-free survival at the same age.
The hazard ratio was 11.8 (95% CI 3.0-107.0), meaning the parents faced nearly 12 times the cardiovascular risk of their children, despite having identical genetic predisposition. The only difference was when treatment started.
This study, while conducted in a high-risk population, illustrates a fundamental principle: duration of LDL cholesterol exposure determines cardiovascular risk more powerfully than the absolute level at any single time point.
What This Means for Clinical Practice
These findings force us to reconsider how we approach cardiovascular prevention in young adults. The traditional model—wait until middle age, calculate 10-year risk, then decide whether to treat—misses the critical window when atherosclerosis begins.
The evidence suggests several key principles:
Cumulative exposure matters more than single measurements. A 30-year-old with an LDL of 130 mg/dL isn't at low risk simply because their 10-year cardiovascular risk is low. They're accumulating atherosclerotic burden that will manifest decades later.
"Normal" cholesterol levels aren't necessarily safe. The PESA study demonstrated atherosclerosis development even in people with LDL cholesterol levels we traditionally consider acceptable. The relationship between LDL and atherosclerosis is continuous, without a clear threshold below which risk disappears.
Earlier intervention has disproportionate benefit. The same reduction in cumulative LDL exposure achieved earlier in life provides greater cardiovascular protection than the same reduction achieved later. This argues for aggressive lifestyle modification, and potentially pharmacotherapy, in young adults with elevated LDL cholesterol.
The absence of other risk factors doesn't confer protection. Young adults who don't smoke, maintain normal blood pressure and blood sugar, and exercise regularly can still develop significant atherosclerosis if their LDL cholesterol is elevated. Cholesterol drives atherosclerosis independently.
The Biological Mechanism: Why LDL Alone Is Sufficient
How can LDL cholesterol cause atherosclerosis in the absence of other risk factors? The mechanism is well-established: LDL particles infiltrate the arterial wall, become oxidized, trigger inflammatory responses, and initiate plaque formation. This process doesn't require diabetes, hypertension, or smoking to occur, those factors accelerate it, but LDL alone is sufficient.
The arterial wall is permeable to LDL particles. When LDL cholesterol levels are elevated, even modestly, more particles enter the arterial wall than can be cleared. Over years and decades, this imbalance leads to lipid accumulation, foam cell formation, and progressive plaque development.
The PESA study's finding that LDL cholesterol was the strongest modifiable factor associated with atherosclerosis in otherwise healthy individuals confirms what decades of basic science research has shown: LDL cholesterol is not just a risk factor for atherosclerosis. It is a causal factor.
Rethinking Prevention: The Case for Earlier, More Aggressive Intervention
The evidence presented here challenges conventional approaches to cardiovascular prevention. If atherosclerosis begins in young adulthood, if cumulative LDL exposure determines long-term risk, and if early intervention provides disproportionate benefit, then our current practice of deferring treatment until middle age may be fundamentally flawed.
This doesn't necessarily mean prescribing statins to every 25-year-old with an LDL of 120 mg/dL. But it does mean taking elevated cholesterol in young adults seriously. It means emphasizing intensive lifestyle modification, diet, exercise, weight management, as first-line therapy. It means recognizing that a "normal" cholesterol level in a young adult may still warrant intervention if it's persistently elevated.
And for young adults with significantly elevated LDL cholesterol, particularly those with genetic predisposition or family history of premature cardiovascular disease—it may mean considering pharmacotherapy much earlier than current guidelines suggest.
Conclusion: Time Is Tissue
In acute myocardial infarction, we say "time is muscle", every minute of delayed treatment means more heart muscle dies. In atherosclerosis prevention, we might say "time is tissue"—every year of elevated LDL cholesterol exposure means more arterial wall damage.
The studies reviewed here demonstrate unequivocally that young, otherwise healthy individuals develop atherosclerotic cardiovascular disease when exposed to elevated LDL cholesterol. The disease doesn't wait for middle age. It doesn't require multiple risk factors. It begins silently in young adulthood and progresses relentlessly over decades.
The good news is that this understanding creates opportunities for intervention. If we identify and address elevated LDL cholesterol early, through lifestyle modification and, when necessary, pharmacotherapy, we can prevent atherosclerosis before it becomes clinically significant. The familial hypercholesterolemia study proves this: early treatment can reduce cardiovascular risk by more than 90%.
The question is whether we'll act on this evidence. Will we continue to defer cholesterol management until middle age, when substantial atherosclerosis has already developed? Or will we embrace a new paradigm that recognizes cumulative LDL exposure as the primary driver of cardiovascular disease and intervenes accordingly?
For young adults with elevated cholesterol, the answer may determine whether they reach age 60 with clean arteries or coronary stents.
Back To The Future:
I'll as you again...
What if you have no insulin resistance, very low triglycerides, high HDL, low BMI, don't smoke, and are very lean and muscular, but have high LDL cholesterol? Can you still get heart diease?
The answer is a resounding YES!
It's just not as fast as someone who isn't as healthy.
References:
- Primary Prevention of Subclinical Atherosclerosis in Young Adults: JACC Review Topic of the Week. Devesa A, Ibanez B, Malick WA, et al. Journal of the American College of Cardiology. 2023;82(22):2152-2162. doi:10.1016/j.jacc.2023.09.817.
- Managing Atherosclerotic Cardiovascular Risk in Young Adults: JACC State-of-the-Art Review. Stone NJ, Smith SC, Orringer CE, et al. Journal of the American College of Cardiology. 2022;79(8):819-836. doi:10.1016/j.jacc.2021.12.016.
- 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Writing Committee Members, Blumenthal RS, Morris PB, et al. Circulation. 2026;. doi:10.1161/CIR.0000000000001423.
- Association Between Cumulative Low-Density Lipoprotein Cholesterol Exposure During Young Adulthood and Middle Age and Risk of Cardiovascular Events. Zhang Y, Pletcher MJ, Vittinghoff E, et al. JAMA Cardiology. 2021;6(12):1406-1413. doi:10.1001/jamacardio.2021.3508.
- Screening for Lipid Disorders in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. US Preventive Services Task Force, Barry MJ, Nicholson WK, et al. JAMA. 2023;330(3):253-260. doi:10.1001/jama.2023.11330.
- Normal LDL-Cholesterol Levels Are Associated With Subclinical Atherosclerosis in the Absence of Risk Factors. Fernández-Friera L, Fuster V, López-Melgar B, et al. Journal of the American College of Cardiology. 2017;70(24):2979-2991. doi:10.1016/j.jacc.2017.10.024.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















