

5000 Milligrams Cholesterol Years Danger Zone
Mar 16, 2026
Cholesterol-Years: How Lifetime Cholesterol Exposure Affects Your Heart
What Are Cholesterol-Years?
Just like doctors measure smoking exposure in "pack-years," researchers have discovered that your lifetime exposure to cholesterol can be measured in "cholesterol-years." This number is calculated by multiplying your LDL cholesterol level (the "bad" cholesterol) by the number of years you've been exposed to that level.
Smoking "pack years" is how many packs per day you smoke. For example, if you have smoked 2 packs per day for five years, you have 2x5, or "10 pack years" of smoking history.
A similar method applies using age and LDL cholesterol to calculate lifetime exposure.
For example, if your LDL cholesterol has been 125 mg/dL for 40 years, you have accumulated 5,000 cholesterol-years (125 × 40 = 5,000).
Why Do Cholesterol Years Matter?
Research has shown that when you reach 5,000 cholesterol-years of exposure, your risk of having a heart attack increases to about 1%. This is a critical threshold where plaque buildup in your arteries becomes significant enough to start causing problems.
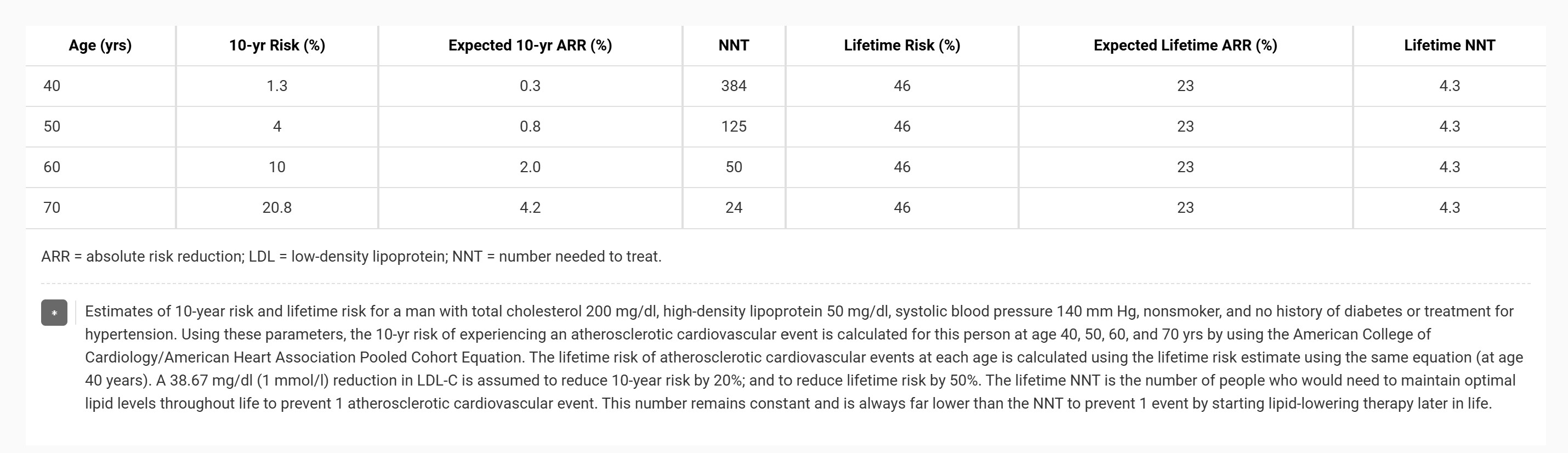
After crossing this threshold, your risk doubles with each additional decade of exposure. For someone with an LDL cholesterol of 125 mg/dL:
- At age 40 (5,000 cholesterol-years): 1% risk
- At age 50 (6,250 cholesterol-years): 2% risk
- At age 60 (7,500 cholesterol-years): 4% risk
- At age 70 (8,750 cholesterol-years): 8% risk
- At age 80 (10,000 cholesterol-years): 16% risk
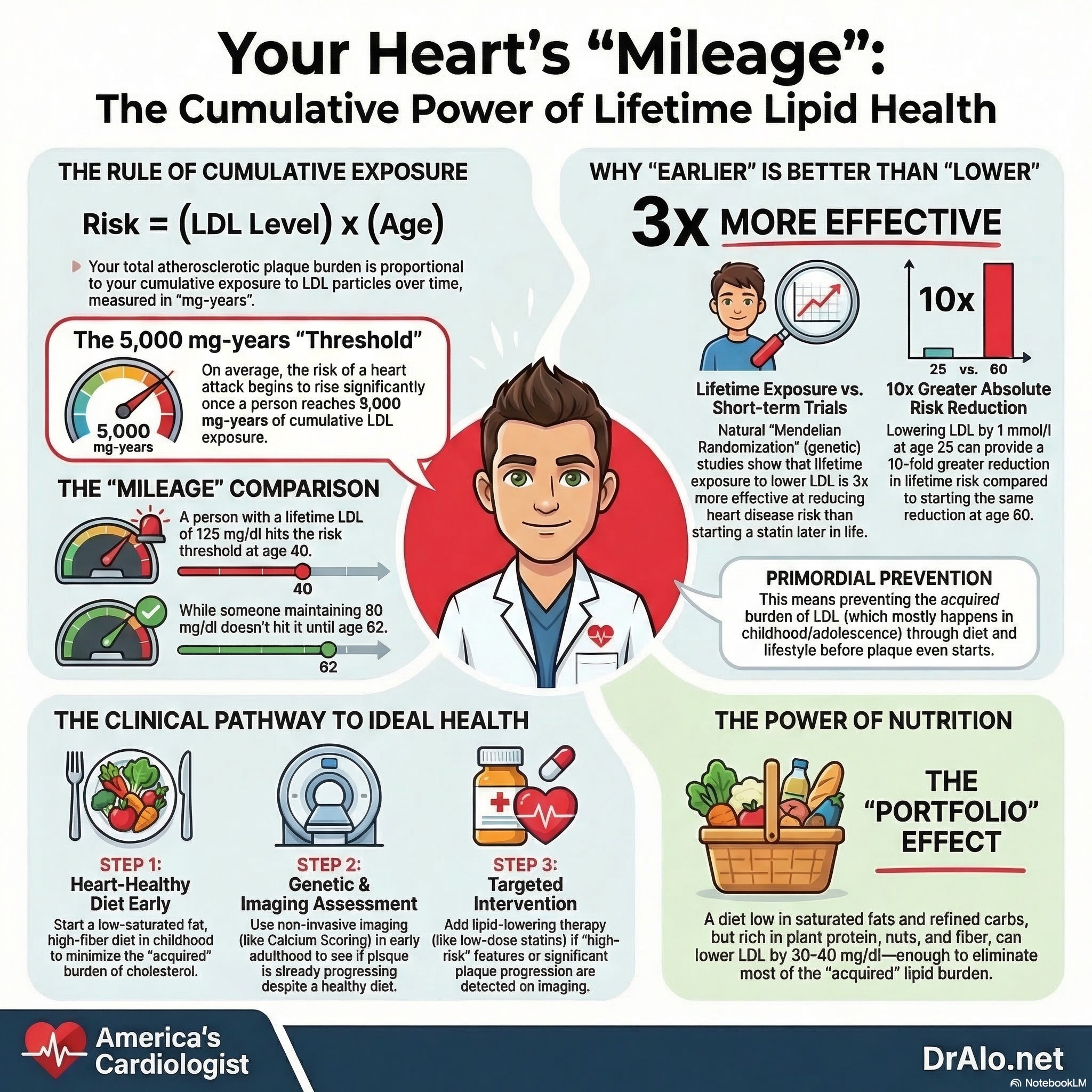
Cholesterol Milligram Years Infographic Summary:
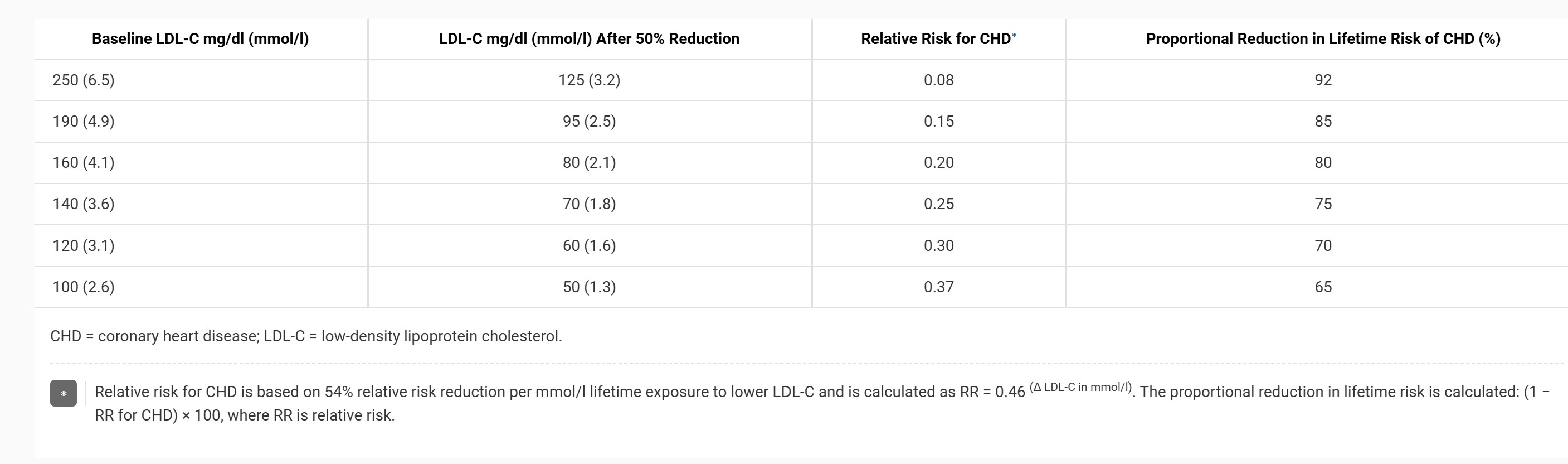
The Power of Lower Cholesterol
The good news is that maintaining lower cholesterol levels throughout your life can dramatically delay when you reach this critical threshold. If you keep your LDL cholesterol at 80 mg/dL instead of 125 mg/dL, you wouldn't reach the 5,000 cholesterol-years threshold until age 62 instead of age 40.
Even more striking: the average age when heart attacks occur (around 8,000 cholesterol-years) would shift from age 64 to age 100 if you maintain an LDL of 80 mg/dL throughout your life.
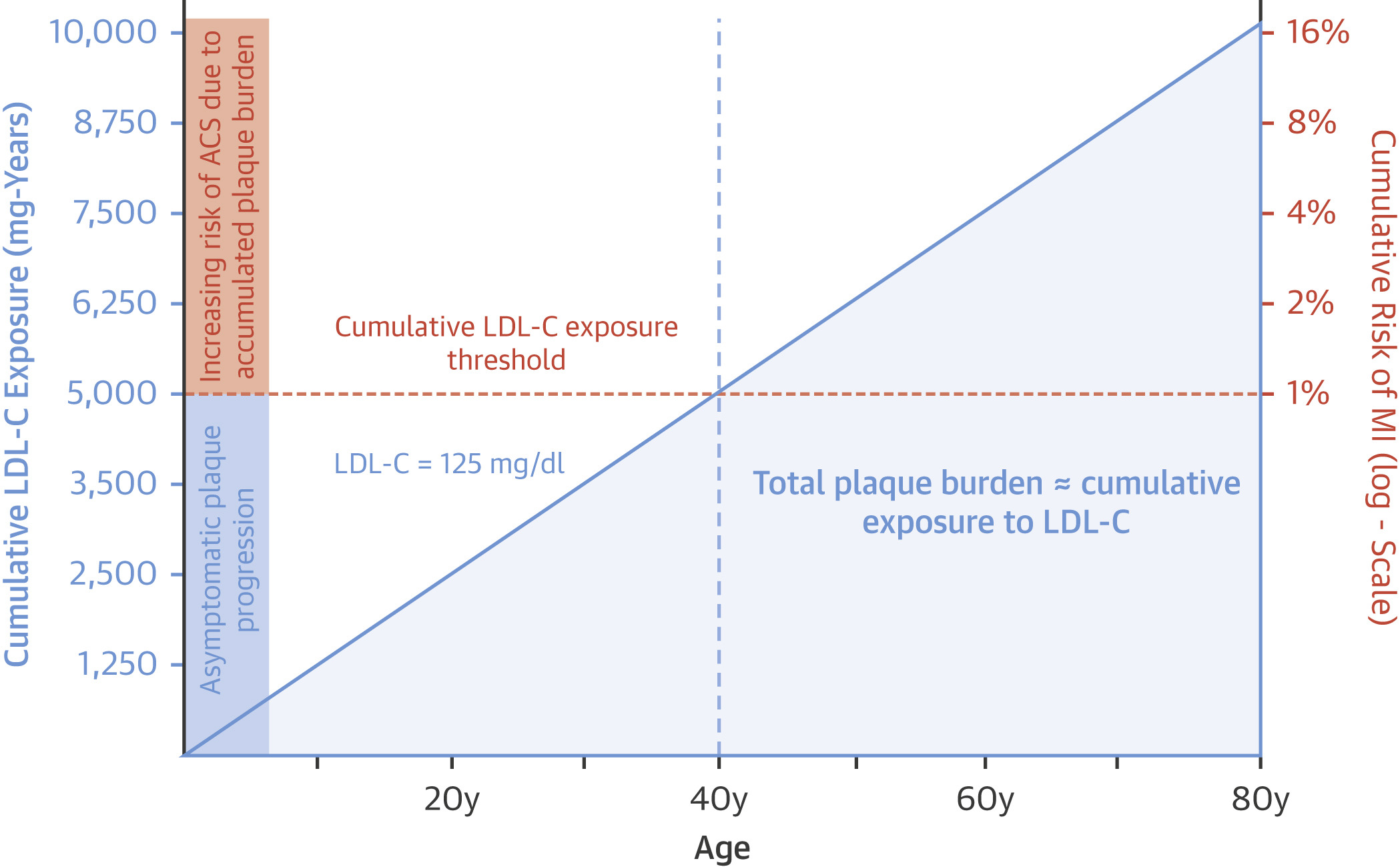
Figure 1. Effect of Cumulative Exposure to LDL on Plaque Burden and Risk of Cardiovascular Disease
The solid blue line represents constant exposure to plasma low-density lipoprotein cholesterol (LDL-C) of 125 mg/dl. Cumulative low-density lipoprotein cholesterol exposure is derived by multiplying age by plasma low-density lipoprotein cholesterol. The shaded area under the solid blue line represents the accumulating total plaque burden (which is directly proportional to both age and cumulative exposure to low-density lipoprotein cholesterol). The horizontal orange dashed line represents the cumulative low-density lipoprotein cholesterol (and therefore total plaque burden) needed to result in a measurable increase in the risk of myocardial infarction (MI). It is derived by multiplying age 40 years (age at which the cumulative incidence of myocardial infarction exceeds 1%) by 125 mg/dl (plasma low-density lipoprotein cholesterol level). Beyond this threshold, if the plasma low-density lipoprotein cholesterol level remains constant, then both cumulative low-density lipoprotein cholesterol exposure and total plaque burden increase linearly, but the risk of myocardial infarction rises log-linearly (and is shown on the right-hand side y-axis expressed on the log or “doubling scale”). ACS = acute coronary syndrome.
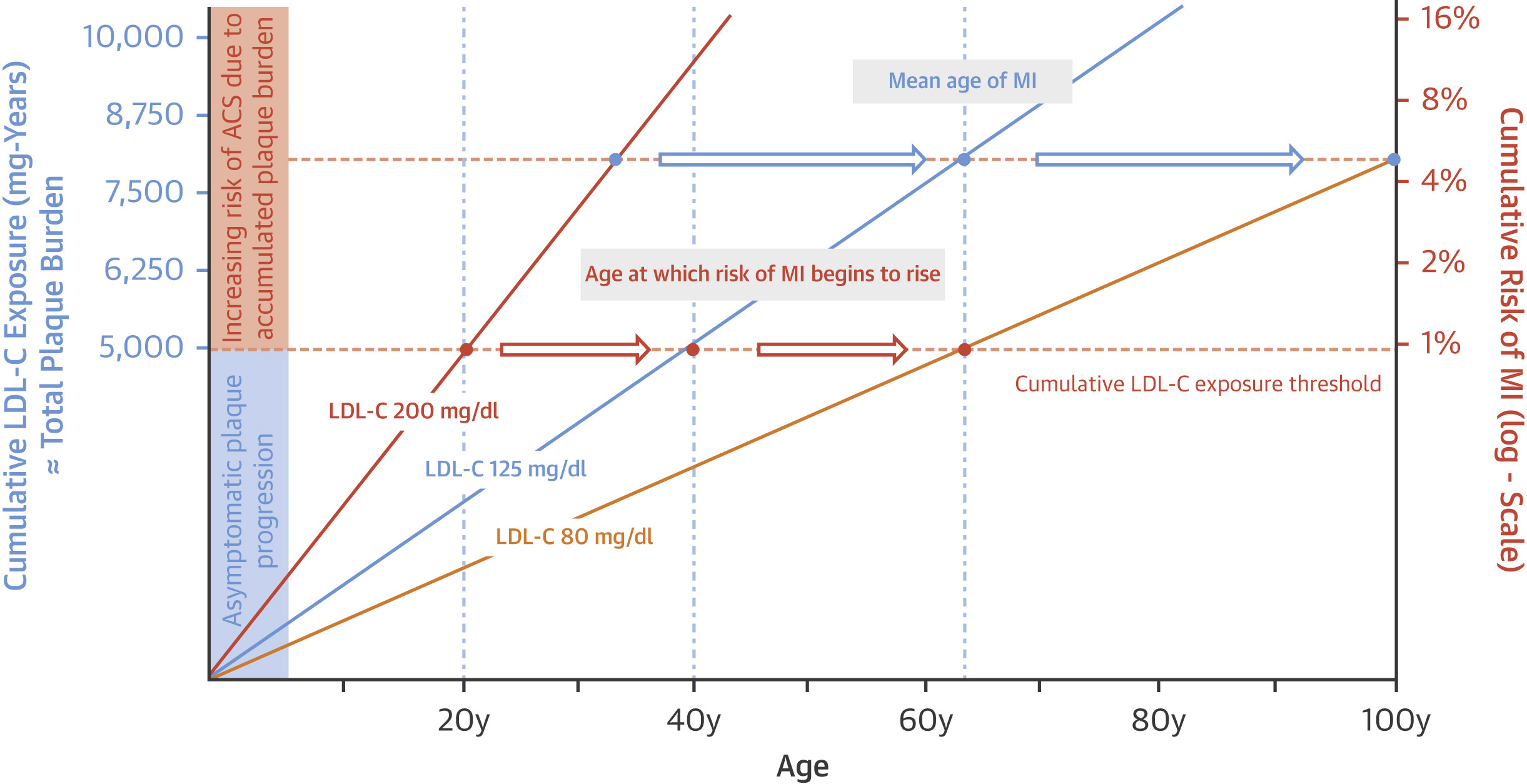
Figure 2. Cumulative Effect of LDL on Risk of Atherosclerotic Cardiovascular Disease
The solid orange line represents a low-density lipoprotein cholesterol (LDL-C) level of 200 mg/dl throughout life. The solid blue line represents a low-density lipoprotein cholesterol level of 125 mg/dl throughout life. The yellow line represents a low-density lipoprotein cholesterol level of 80 mg/dl throughout life. Cumulative low-density lipoprotein cholesterol exposure is derived by multiplying age by plasma low-density lipoprotein cholesterol. Cumulative risk of myocardial infarction (MI) is measured on the log (“doubling”) scale. The orange dots represent the age at which persons with lifetime exposure to 200 mg/dl, 125 mg/dl, and 80 mg/dl, respectively, exceeds the 5,000 mg-years threshold of cumulative exposure to low-density lipoprotein cholesterol beyond which the cumulative lifetime risk of myocardial infarction exceeds 1%. The blue dots represent the average age that persons with lifetime exposure to 200 mg/dl, 125 mg/dl, and 80 mg/dl, respectively, experience a myocardial infarction (or approximately 8,000 mg-years of cumulative low-density lipoprotein cholesterol exposure). The figure shows that lower cumulative exposure to low-density lipoprotein cholesterol can slow plaque progression and delay the onset of myocardial infarction and other acute coronary syndromes (ACS). Abbreviations as in Figure 1.
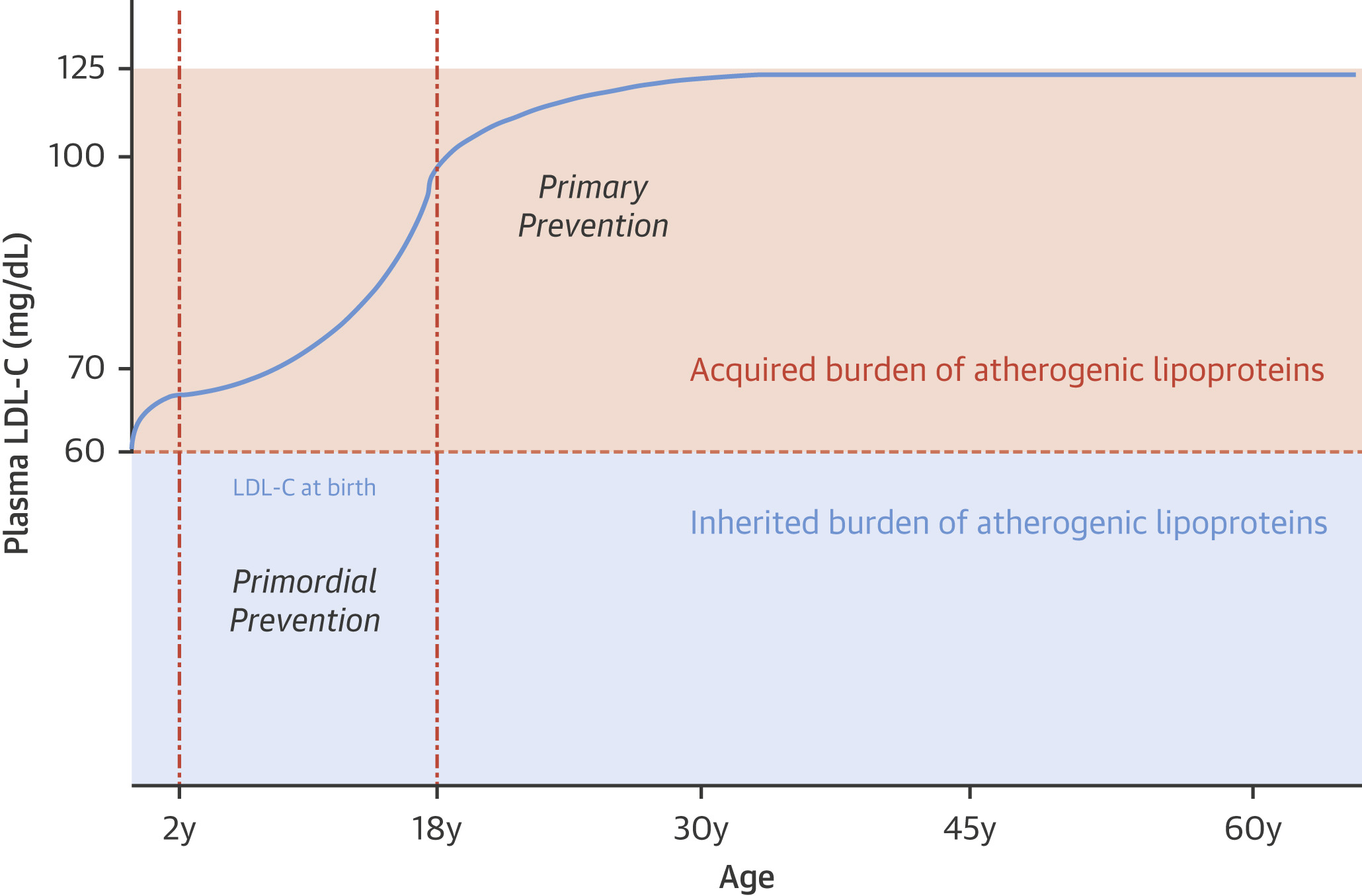
Figure 3. Life Course Trajectory of LDL and Implications for Primordial Prevention
The blue line represents mean low-density lipoprotein cholesterol (LDL-C) level at each age. The blue shaded area represents the inherited burden of low-density lipoprotein cholesterol and is equal to the low-density lipoprotein cholesterol level at birth. The orange shaded area represents the acquired burden of low-density lipoprotein cholesterol that is equal to the low-density lipoprotein cholesterol level at each age minus the low-density lipoprotein cholesterol level at birth.
In the above graphic, it's very important to note that below 60 mg/dL of LDL cholesterol, you do not see heart disease. This has been shown over time in multiple studies and cohorts. This is why we use 55 mg/dL as a cutoff for many targets and treatment guidelines.
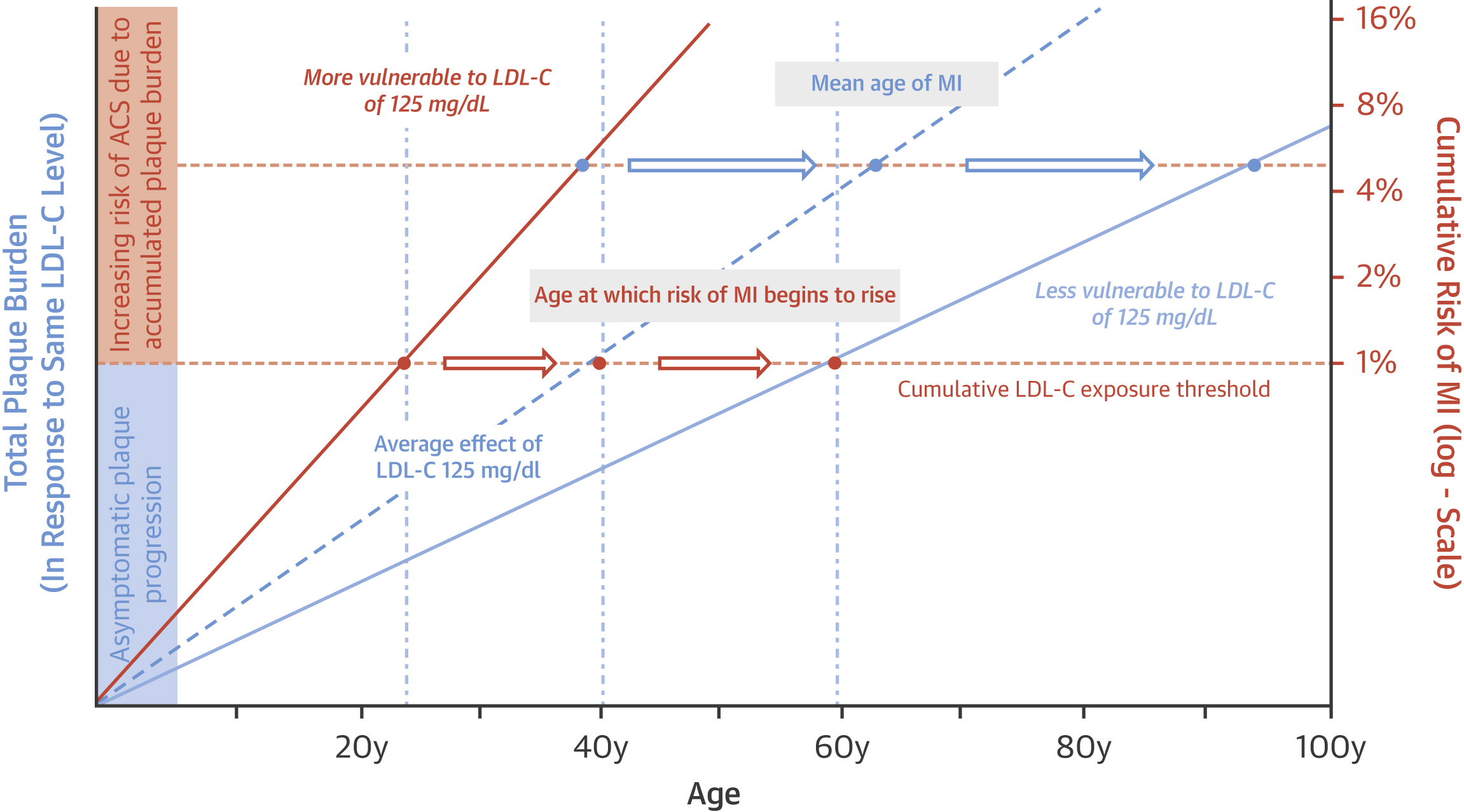
Figure 4. Differential Vulnerability to Retaining LDL and Other Apo B–Containing Lipoproteins
The dashed blue line represents the average rate of total plaque burden accumulation in response to a plasma low-density lipoprotein cholesterol (LDL-C) level of 125 mg/dl. The solid orange line (top) represents the rate of plaque burden increase for people with a low-density lipoprotein cholesterol level of 125 mg/dl who retain low-density lipoprotein particles in the artery wall more avidly. The solid light blue line (bottom) represents the rate of plaque burden increase for people with a low-density lipoprotein cholesterol level of 125 mg/dl who retain low-density lipoprotein particles in the artery wall less avidly. Cumulative risk of myocardial infarction (MI) is measured on the log (“doubling”) scale. Figure shows that people who are more vulnerable to retaining low-density lipoprotein particles have more rapid plaque progression and experience cardiovascular events at an earlier age in response to exposure to the same level of circulating low-density lipoprotein particles (as estimated by plasma low-density lipoprotein cholesterol) than people who are less vulnerable to retaining low-density lipoprotein particles. ACS = acute coronary syndrome; Apo B = apolipoprotein B.
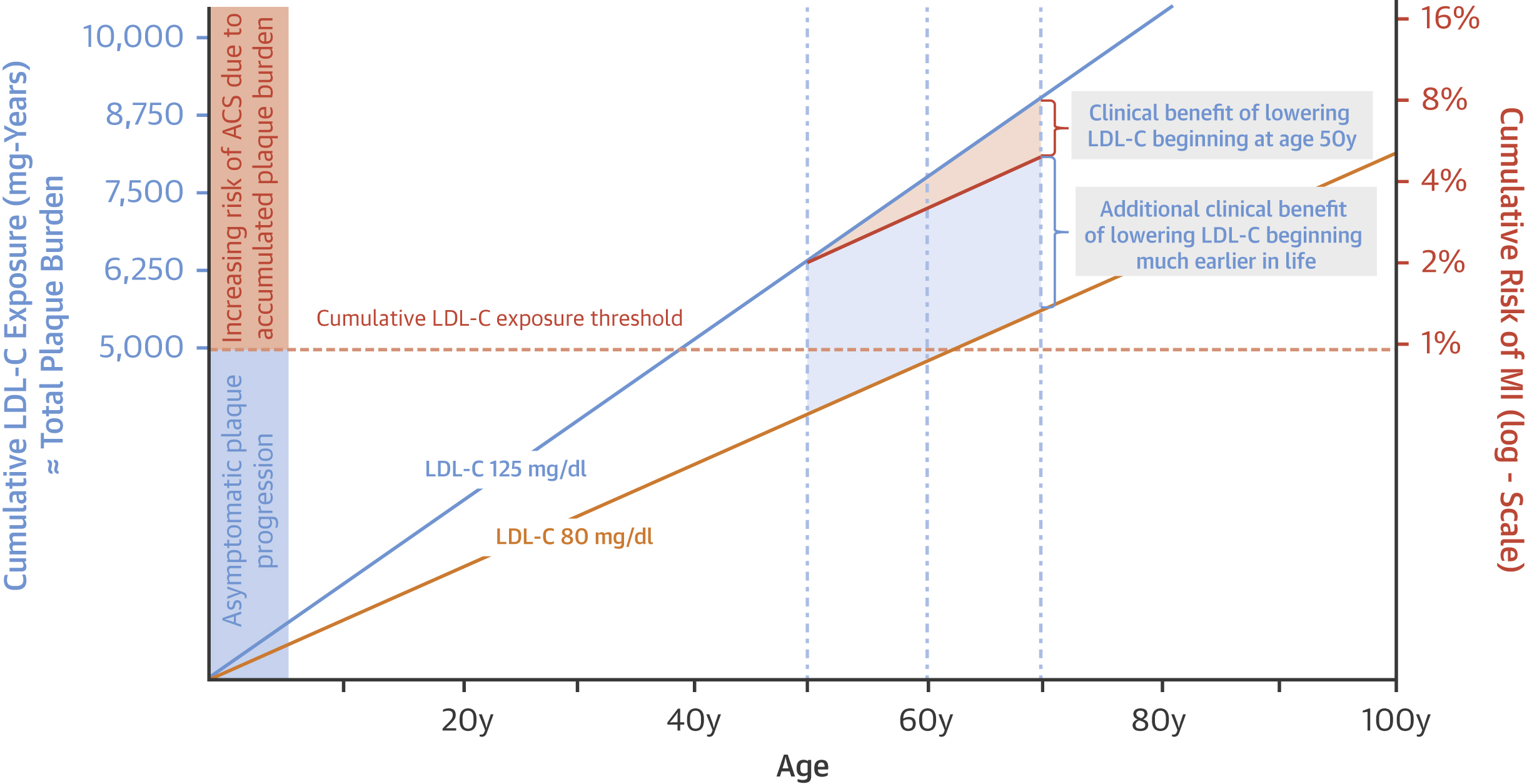
Figure 5. Effect of Primary and Primordial Prevention on Progression of Atherosclerosis and Risk of Acute Cardiovascular Events
The solid blue line is a low-density lipoprotein cholesterol (LDL-C) level of 120 mg/dl. The yellow line is a low-density lipoprotein cholesterol level of 80 mg/dl. The solid orange line represents lowering low-density lipoprotein cholesterol by 40 mg/dl (approximately 1 mmol/l) from 120 to 80 mg/dl beginning at age 50 years and extending to age 70 years. Cumulative low-density lipoprotein cholesterol exposure is derived by multiplying age by plasma low-density lipoprotein cholesterol. Cumulative risk of myocardial infarction (MI) is measured on the log (“doubling”) scale. The orange shaded area represents a 25% relative risk reduction in myocardial infarction (MI) as a result of lowering low-density lipoprotein cholesterol by 40 mg/dl from 120 to 80 mg/dl from age 50 to 70 years. During this period of treatment, however, the “residual” risk of myocardial infarction remains high because of the high accumulated total plaque burden (as estimated by the cumulative exposure to low-density lipoprotein cholesterol). The blue shaded area represents the additional clinical benefit that could be achieved by maintaining low-density lipoprotein cholesterol at 80 mg/dl throughout life (which essentially eliminates the “residual” risk of myocardial infarction). ACS = acute coronary syndrome.
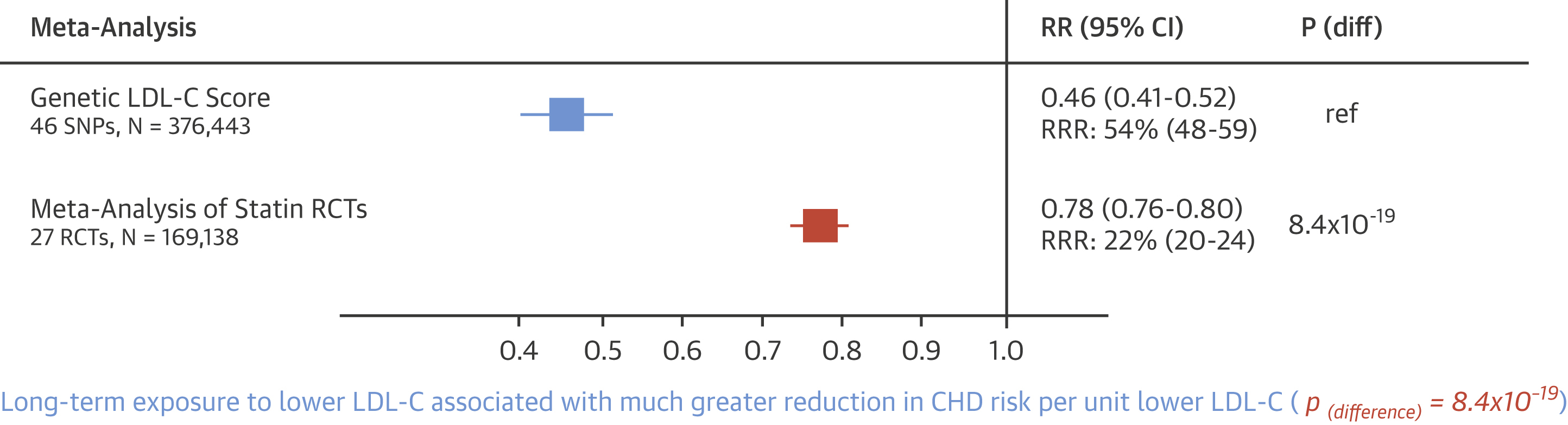
Figure 6. Comparison of Proportional Risk Reduction in Cardiovascular Events per mmol/l Lower LDL by Duration of Exposure to Lower LDL
The blue box is the odds ratio for coronary heart disease (CHD), defined as CHD death or nonfatal myocardial infarction, per 38.67 mg/dl (1 mmol/l) lower lifetime exposure to lower low-density lipoprotein cholesterol (LDL-C) as estimated from a meta-analysis of Mendelian randomization studies using a genetic low-density lipoprotein cholesterol score consisting of 46 genetic variants associated with low-density lipoprotein cholesterol at a p value threshold of ≤5.0 × 10-8 (and with at least an 80% concordant effect on apolipoprotein B levels). The orange box is the relative risk (RR) for major coronary events per 38.67 mg/dl (1 mmol/l) lower low-density lipoprotein cholesterol derived from the Cholesterol Treatment Trialists meta-analysis of statin trials. The lines across the boxes represent 95% confidence intervals (CI). P (diff) = p(difference); RCT = randomized controlled trial; ref = reference; RRR = relative risk reduction.
What This Means for You
This research shows that cholesterol exposure adds up over time, like interest on a loan. The earlier you start managing your cholesterol, the more you can reduce your lifetime risk of heart disease. Even small reductions in cholesterol levels, when maintained over many years, can make a big difference in preventing heart attacks.
Talk to your doctor about your cholesterol levels and whether lifestyle changes or medications might help you reduce your cumulative cholesterol exposure and protect your heart health for the long term.
References:
https://www.jacc.org/doi/pdf/10.1016/j.jacc.2018.06.046
https://jamanetwork.com/journals/jamacardiology/fullarticle/2784038
https://www.sciencedirect.com/science/article/abs/pii/S1933287423003562
https://www.sciencedirect.com/science/article/pii/S073510972036232X
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















