

Extreme Athletes And Increased Cardiovascular Risk
Apr 08, 2026
The Dark Side of Being Fit: What Happens to Your Heart When You Exercise Too Much for Too Long
A major 2026 joint consensus from the European Society of Cardiology and the American College of Cardiology reveals that dedicated older athletes face a paradox: the very training that protects their hearts may also leave marks on them. Here is what every serious exerciser over 35 needs to know.
Can you ever exercise too much? Can it be bad for you?
You train hard. You log your miles, hit your power targets, and track your VO2 max. You eat well, sleep well, and your resting heart rate is the envy of your sedentary colleagues. By any reasonable measure, you are a model of cardiovascular health.
And yet, a 2026 joint consensus statement from the European Association of Preventive Cardiology, the European Society of Cardiology, and the American College of Cardiology raises a question that should make every dedicated older athlete pause: what is all that training doing to your heart over decades?
The answer is nuanced, important, and not at all what most fitness-oriented patients expect to hear from their cardiologist.
The paper, titled Masters Athletes With Abnormal Cardiovascular Findings, was published in JACC in 2026 and co-authored by more than 30 international experts in sports cardiology. It is the most comprehensive guidance document ever assembled on the cardiovascular risks that are unique to older competitive athletes. I am going to walk you through it in detail, because what it says has direct clinical implications for anyone who has been training seriously for years.
First: Who Is an Extreme or "Masters" Athlete?
The consensus defines a Masters athlete as anyone 35 years of age or older who trains habitually, exceeds standard physical activity recommendations (more than 300 minutes per week), and participates in competition or structured performance goals. This is not a recreational walker or someone who does yoga twice a week. We are talking about the 55-year-old triathlete, the 62-year-old marathon runner, the 50-year-old cyclist who puts in 200 miles a week.
This population has grown dramatically over the past few decades, and with that growth has come a harder clinical question: are the hearts of highly trained older adults fundamentally different from those of their sedentary peers, and if so, how should they be managed when cardiac findings are discovered?
The answer, as this document makes clear, is yes, they are different, and the clinical management needs to reflect that difference.
The Paradox at the Center of This Document
Exercise reduces the risk of cardiovascular disease and all-cause mortality. That is settled science. Physically active people live longer and have fewer heart attacks than sedentary people. The dose-response relationship is real: more exercise generally means more benefit.
But the relationship is not infinitely linear. At very high training volumes over very long periods of time, something changes. The heart adapts structurally to decades of hemodynamic load, and some of those adaptations appear to cross from physiological into pathological territory in a subset of athletes. The document calls this the 'exercise paradox.'
The authors are careful to note that this does not mean exercise is bad. It means that Masters athletes are a clinically distinct population whose cardiac findings cannot simply be interpreted using the same frameworks we use for sedentary patients with heart disease. And it means that the assumption that exercise is always protective, in every domain, at every dose, is incomplete.
Extreme Athletes and Cardiovascular Disease Risk Infographic Summary:
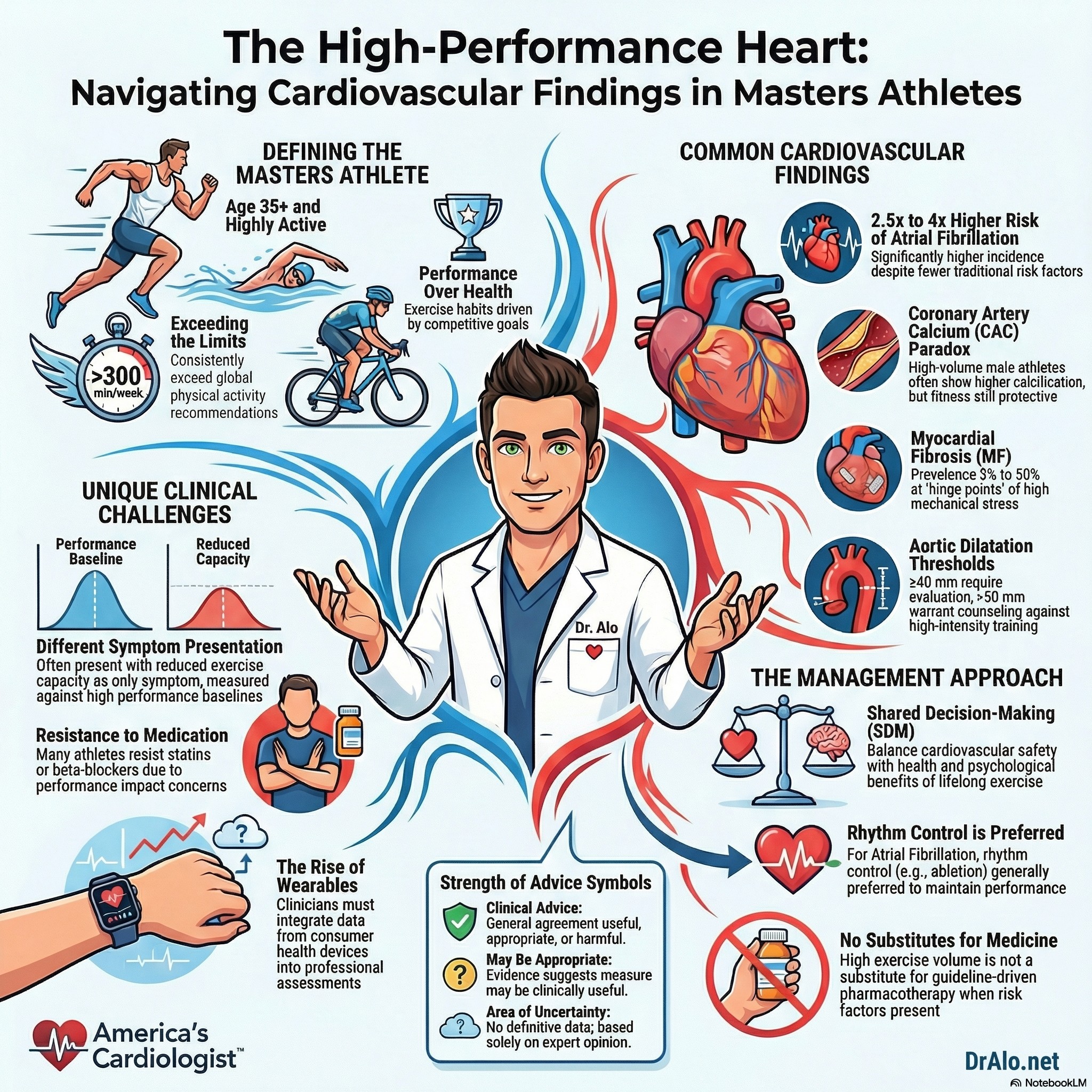
The Seven Cardiac Findings in Masters Athletes
The consensus document covers seven specific cardiovascular abnormalities that are more prevalent in Masters athletes than in sedentary controls. Here is a plain-language breakdown of each:
- Atrial Fibrillation: The Most Common Problem
Atrial fibrillation (AF) is the abnormal heart rhythm in which the upper chambers of the heart quiver chaotically instead of contracting effectively. It is the most common arrhythmia in the general population and becomes more prevalent with age.
In Masters athletes, the risk is dramatically higher. Among competitive Nordic skiers, the prevalence of AF is approximately twice that of comparable non-athletes. Across multiple studies, the adjusted hazard ratio for AF in Masters athletes ranges from 2.5 to 4.0 compared to sedentary peers. And unlike many other conditions where women have lower risk than men, this elevated AF risk exists in both sexes, though absolute rates remain lower in women.
Why does this happen? Several mechanisms are at play. Decades of sustained cardiovascular training stretch and remodel the atria. Vagal tone is chronically elevated in endurance athletes, slowing electrical conduction. There may also be low-grade inflammatory changes that promote atrial fibrosis over time. The result is an atrium that is electrically unstable.
The clinical approach to AF in Masters athletes differs importantly from the general population. Rate control strategies, which use beta-blockers, calcium channel blockers, or digoxin to slow the heart rate, are often poorly tolerated in athletes because they impair exercise capacity and in some cases are prohibited in competition. Rhythm control is the preferred strategy, meaning the goal is to restore and maintain normal sinus rhythm rather than simply letting the rate run fast.
Pulmonary vein isolation (PVI), the catheter ablation procedure used to treat AF, is now considered a reasonable first-line option in Masters athletes with symptomatic AF, not just a last resort. Prior concerns that ablation would be less effective in athletes have not been borne out in the data. Success rates are comparable to non-athletes.
Anticoagulation decisions follow the standard CHA2DS2-VA scoring system, the same tool used in the general population. There is no evidence to support athlete-specific anticoagulation thresholds, and those who meet criteria for anticoagulation should receive it, with the caveat that athletes in collision sports need individualized counseling about bleeding risk.
- Bradyarrhythmias: When the Heart Slows Too Much
A slow resting heart rate is considered a sign of fitness. Most trained athletes have resting heart rates well below 60 beats per minute. Some Masters athletes have rates below 40 bpm at rest and may show first-degree or type-1 second-degree AV block on their ECG. Under normal circumstances, these findings in a trained athlete require no intervention.
The concern arises when symptoms appear: dizziness, presyncope, fatigue, or unexplained drops in exercise performance. These symptoms, if linked to true chronotropic incompetence (the inability to raise heart rate appropriately during exercise), need investigation. The workup should include ambulatory monitoring, exercise testing, and a careful assessment of the chronotropic response to maximal effort.
More concerning, emerging data from large cohorts of competitive cross-country skiers show a dose-response relationship between lifetime competition volume and the risk of developing sinus node disease or third-degree AV block. Long-term incidence of clinically significant bradycardia and the need for pacemaker implantation were 19% and 17% more frequent in competitive skiers compared to the general population. This is not something that resolves when training stops.
- Ventricular Arrhythmias: Not Always Benign
Premature ventricular contractions (PVCs) are common in endurance athletes. Studies report them in up to 7% of ultra-marathon finishers immediately post-race and in 34% of middle-aged and older athletes undergoing pre-participation stress testing.
In younger athletes, isolated PVCs with typical morphology (originating from the right or left ventricular outflow tract or fascicles) and no associated structural disease are usually benign. In Masters athletes, the picture is more complicated. PVCs are more likely to have higher-risk features in older athletes compared to younger ones, and the existing guidelines for athletes were developed almost exclusively from data on young competitors.
High-risk PVC features that warrant further evaluation include: atypical morphology (not from the outflow tract or fascicles), polymorphic or repetitive PVCs, coupling intervals below 360 milliseconds, PVC burden above 10% on 24-hour Holter monitoring, PVCs that increase with exercise rather than suppress, and PVCs that coincide with sudden onset exercise intolerance. When these features are present, a full cardiac workup including cardiac MRI is appropriate.
- Coronary Atherosclerosis: The Counterintuitive Finding
This is probably the finding that surprises patients most. Regular exercise improves lipid levels, blood pressure, inflammation, and glucose tolerance. It should, in theory, protect against coronary artery disease. And at the population level, it does.
But at the individual level, for highly trained male endurance athletes, something paradoxical occurs: coronary artery calcium (CAC) scores tend to be higher in male Masters athletes compared to less active peers of similar age and risk factor profile. Multiple studies, including the Radboud study, the Merghani study, and the Master@Heart trial, have confirmed this pattern in men, though the finding does not appear to apply to women.
Does this mean exercise is causing heart disease? Not necessarily. One theory is that exercise-associated coronary calcification produces a more stable plaque phenotype, characterized by calcified rather than lipid-rich soft plaques, similar to what statins do. The exercise may accelerate plaque calcification without necessarily causing rupture-prone lesions. But the Master@Heart study found similar calcified plaque prevalence between lifelong athletes and active controls, complicating that interpretation.
What is clinically clear is this: exercise does not cancel out the prognostic significance of a high CAC score. Data from the Cooper Center Longitudinal Study in over 21,000 men show that high exercise volume reduces all-cause mortality in men with a CAC below 100, but that among men with a CAC of 100 or above, the event rate was similar regardless of how much they exercised. In other words, once calcified plaque burden crosses a threshold, fitness does not erase the risk.
The clinical guidance is clear: Masters athletes with elevated CAC scores should receive guideline-directed management of cardiovascular risk factors, including lipid-lowering therapy, just as the general population would. A CAC above 300 Agatston units has been shown in registry data to carry a cardiovascular event risk equivalent to that of someone with prior MI, stroke, or peripheral artery disease. That warrants aggressive treatment, regardless of fitness level.
Statins are the primary treatment tool here. And this brings up a critically important point: Masters athletes often resist pharmacotherapy. The belief that training at high volumes negates the need for medication is deeply embedded in fitness culture and is clinically wrong. No amount of exercise substitutes for guideline-directed pharmacotherapy when risk factors are present.
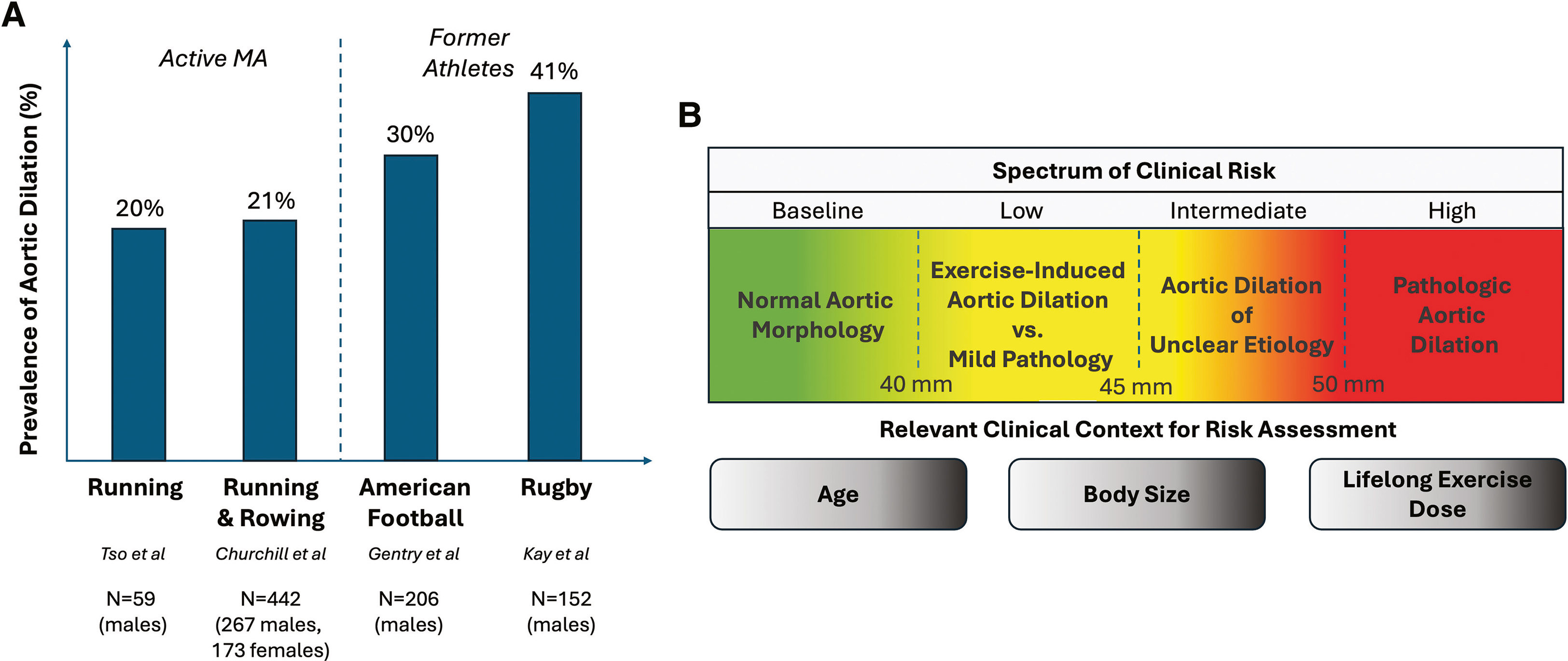
- Aortic Dilatation: A Growing Aorta
The aorta is the largest blood vessel in the body, carrying blood away from the heart. In athletes, sustained pressure and volume loads may stretch the aorta over time. Studies have found aortic diameters approximately 3 mm larger in athletes compared to controls on average.
In young athletes, aortic dilatation is rare, seen in only 1 to 2% of competitive athletes. In Masters athletes, the numbers are strikingly higher: mild aortic dilatation (40 to 45 mm) was present in roughly 20% of Masters runners and rowers in one series, and prevalences up to 41% have been reported in former elite strength athletes, including American football and rugby players.
The clinical management is stratified by aortic size. Athletes with aortic diameters of 40 to 44 mm without a heritable genetic cause are generally considered low risk and can continue training with appropriate surveillance. Those with dimensions of 45 to 50 mm are at intermediate risk and need individualized evaluation. Those meeting or exceeding established surgical thresholds of 50 mm should avoid high-intensity training and be evaluated for surgical intervention.
Genetic testing is appropriate for athletes with confirmed enlargement above 45 mm, to evaluate for heritable connective tissue disorders such as Marfan syndrome or Loeys-Dietz syndrome that carry independent aortic risk.
- Myocardial Fibrosis: Scar Tissue in the Heart
Cardiac MRI can detect late gadolinium enhancement (LGE), a marker of myocardial fibrosis or scarring. Myocardial fibrosis can result from prior ischemia, inflammation, or chronic hemodynamic overload. In Masters athletes, studies using cardiac MRI have found LGE in anywhere from 3% to 50% of subjects, with wide variation depending on the study design, athlete population, and imaging protocol.
The clinical significance of LGE in athletes depends heavily on its pattern. Isolated LGE at the right ventricular insertion points, sometimes called the hinge points, is extremely common in athletes and appears to be benign. No additional workup is required for this finding in an asymptomatic athlete. In contrast, non-ischemic LGE in a stria pattern in the left ventricle, or LGE associated with complex ventricular arrhythmias, is a different matter entirely and warrants thorough risk stratification including exercise testing and extended ambulatory monitoring.
Myocardial fibrosis may create an electrical substrate for dangerous ventricular arrhythmias, which is why the pattern and extent of LGE matter so much. Asymptomatic athletes with isolated RV insertion point LGE need no intervention. Athletes with extensive, non-ischemic LGE and ventricular arrhythmias may need to temporarily restrict competition, undergo electrophysiology study, and potentially receive antiarrhythmic therapy or an implantable cardioverter-defibrillator.
- Exercise-Induced Arrhythmogenic Cardiomyopathy: A Rare but Serious Phenotype
This is the most controversial and least well-defined entity in the document. Some Masters athletes with decades of high-intensity endurance training, particularly cycling, triathlon, and rowing, develop a pattern of disproportionate right ventricular (RV) dilation, impaired RV function, and ventricular arrhythmias of RV origin that cannot be explained by any other cause. This has been labeled exercise-induced arrhythmogenic cardiomyopathy, or ExI-ACM.
The condition was initially confused with genetic arrhythmogenic right ventricular cardiomyopathy (ARVC), but ExI-ACM cases typically do not carry the pathogenic desmosomal gene variants found in ARVC. The hypothesis is that the right ventricle, which handles pressure and volume loads disproportionately during sustained high-intensity exercise, may develop maladaptive remodeling over years or decades in susceptible individuals.
The prognosis data are sobering but must be interpreted carefully. An early case series from three tertiary sports cardiology centers found that of 46 high-level endurance athletes with complex ventricular arrhythmias, 18 had major arrhythmic events including 9 sudden cardiac deaths over a median of just 2 years. However, this series almost certainly selected the most severe phenotypes from referral centers, and the true population-level incidence of ExI-ACM is unknown and likely very low.
ExI-ACM is a diagnosis of exclusion. Before reaching this conclusion, genetic ARVC, dilated cardiomyopathy, sarcoidosis, and other structural heart diseases must be ruled out. When the diagnosis is suspected, the recommended first step is prescribed detraining, which has been associated with partial reversal of structural changes and reduction in arrhythmia burden in observational studies.
Quick Reference: The Seven Findings at a Glance
|
Finding |
What It Means |
Key Takeaway |
|
Atrial Fibrillation |
2-4x higher risk in Masters athletes |
Rhythm control preferred; ablation is a first-line option |
|
Coronary Calcification |
Higher in male endurance athletes |
Exercise does not cancel out CACS above 100; statins apply |
|
Aortic Dilatation |
20 to 41% in some athlete groups |
Risk stratified by size; below 44 mm generally low risk |
|
Myocardial Fibrosis |
3 to 50% prevalence by CMR (study-dependent) |
Context and LGE pattern determine clinical significance |
|
ExI-ACM |
Rare, debated, RV-predominant cardiomyopathy |
Diagnosis of exclusion; detraining is first step |
Four Clinical Challenges Unique to Masters Athletes
The consensus document identifies four challenges that make managing this population fundamentally different from managing sedentary patients with the same diagnoses. As a cardiologist, I encounter all four of these regularly.
Challenge 1: A Different Symptom Presentation
Masters athletes do not always present with chest pain or classic angina. Their chief complaint is often a subtle decline in exercise performance or endurance, something they notice because they track their metrics obsessively and because their baseline is so far above the general population that impairment shows up early. A drop in power output, worsening race times, or unexpected fatigue at training intensities that used to feel comfortable should be taken seriously as potential cardiac symptoms in this population, not attributed to aging, overtraining, or stress without proper evaluation.
Challenge 2: Resistance to Medication
I see this constantly. Athletes who exercise six or seven days a week, maintain healthy weights, and eat reasonably well often genuinely believe that their lifestyle makes medication unnecessary. When I recommend a statin for a 58-year-old cyclist with a CAC score of 180, or an antihypertensive for a 52-year-old runner with consistently elevated blood pressure, the initial resistance can be significant. The misconception is understandable but dangerous. Exercise and pharmacotherapy are not competing strategies. They are complementary ones. This document is unambiguous on that point.
Challenge 3: Wearable Device Data
Masters athletes increasingly show up to clinic visits with months of ECG data from their Apple Watch, Garmin, or Polar monitor. They have heart rate variability trends, training load curves, and occasionally rhythm strips showing pauses or irregular beats recorded during training. The guidance here is practical: clinicians need to develop familiarity with these devices and integrate the data into clinical assessment, rather than dismissing it. A 48-hour monitoring study may show much less than what a dedicated athlete's wearable captured over 90 days of training.
Challenge 4: Shared Decision-Making Is Not Optional
Almost all of the clinical guidance in this document explicitly emphasizes shared decision-making, abbreviated SDM throughout the paper. This is not a soft concept or a box-checking exercise. For a 60-year-old with aortic dimensions of 46 mm and a goal of completing an Ironman, the conversation about risk and benefit is genuinely complex and deeply personal. The cardiologist's job is to present what is known, what is not known, and what the risk-benefit tradeoffs are, then reach a decision together with the athlete. Blanket exercise restriction without that conversation is not appropriate in most cases, and neither is ignoring an abnormal finding because the patient does not want to hear about it.
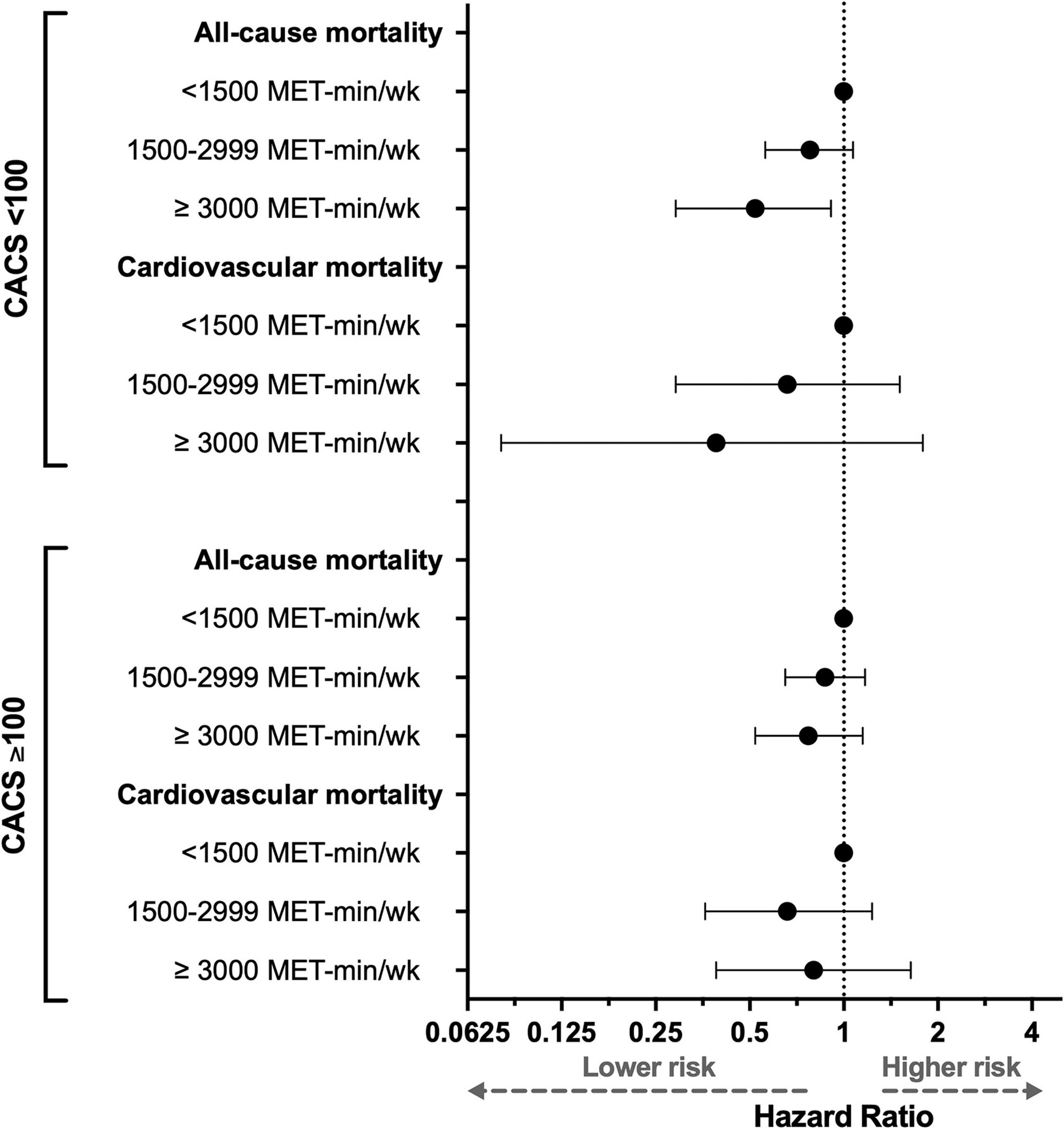
The figure above shows that the more MET-min/week, the more improved reduction in all-cause mortality and cardiovascular mortality for those who have a calcium score under 100. However, if your calcium score is over 100, while you still have improved risk reduction, it is not as much as it is for those with lower calcium score. This makes sense because those with more calcium have more established heart disease risk, and it will not improve as much by more exercise. It will improve, but not as much as it dose for those with lower scores. Those with higher CAC usually have higher LDL cholesterol and a higher plaque burden.
What This Means for You Specifically
If you are a Masters athlete who trains hard and competes regularly, here is what I want you to take away from this document:
- Exercise is still protective overall. Nothing in this document negates the overwhelming evidence that regular physical activity reduces cardiovascular mortality. Masters athletes have lower overall cardiac death rates than sedentary peers. The goal is not to stop training.
- High exercise volume does not confer immunity from traditional risk factors. If you have hypertension, dyslipidemia, a family history of premature heart disease, or a high CAC score, those risks apply to you. Training does not override them. Treat the risk factors.
- A high CAC score changes the calculus. Once your coronary artery calcium score exceeds 100 Agatston units, exercise no longer attenuates your cardiovascular event risk in the way it does at lower scores. If you are a male endurance athlete over 45 and have never had a CAC score, that conversation is worth having with your cardiologist, particularly if you have any traditional risk factors.
- AF in athletes often requires rhythm control and may benefit from ablation. If you develop atrial fibrillation, do not accept a rate-control strategy as your only option without understanding why rhythm control was not recommended first. For most athletes, maintaining sinus rhythm matters for performance and quality of life.
- Statins do not impair athletic performance meaningfully. The concern that statins will tank your training is not supported by the evidence for most athletes. Statin-associated muscle symptoms occur but are manageable, and the cardiovascular protection they provide in high-risk athletes is the same as in any other patient.
- Sudden drops in exercise capacity are not aging. If your performance falls off sharply over weeks rather than gradually over years, that is not a normal aging phenomenon. Get evaluated.
- Performance-enhancing drugs worsen all of these risks. The document specifically flags this. Anabolic steroids, growth hormone, EPO, and related substances are known to accelerate coronary disease, promote cardiac remodeling, and increase arrhythmia risk. If this applies to you, your cardiologist needs to know.
What the Science Still Does Not Know
One of the most honest aspects of this consensus document is its willingness to list what remains uncertain. There are no randomized controlled trials in Masters athletes for any of the conditions it covers. Guidelines were not written for this population and have to be extrapolated from sedentary patients. The evidence base is almost entirely observational, often from small single-center studies.
Key unanswered questions include: Does prescribed detraining reduce AF recurrence rates? Does PCSK9 inhibitor therapy modify plaque risk in high-volume exercisers differently than in the general population? Does aortic dilatation progress faster in athletes who continue training? What predicts who will develop ExI-ACM versus who will simply have a large but otherwise healthy athlete's heart? How do these risks differ by race and ethnicity, where essentially no data currently exist?
These gaps matter clinically, and the authors are clear that longitudinal registries and dedicated trials in athlete populations are urgently needed. Until then, management relies on expert consensus, individual clinical judgment, and the kind of shared decision-making that this document advocates throughout.
My Bottom Line as a Cardiologist
The question I get asked most often by dedicated older athletes is: 'Is it okay for me to keep training at this level?' The honest answer is that for most of you, yes. The cardiovascular benefits of lifelong training are real, large, and durable. But the answer is not automatically yes for every athlete in every clinical situation, and this consensus document is the most authoritative framework we have for navigating those exceptions.
What I want you to do is this: see a cardiologist who understands athletes, not just someone who will tell you to slow down or someone who will dismiss your findings because you seem healthy. Get a comprehensive cardiovascular risk factor assessment. Know your blood pressure, your lipids, your ApoB, and if indicated, your coronary artery calcium score. If you have symptoms such as reduced exercise capacity, palpitations, or unexplained fatigue, do not train through them. Get evaluated.
The goal is not to stop exercising. The goal is to keep exercising safely for the rest of your life. That requires knowing what your heart is actually doing, not assuming it is fine because you can still finish a century ride.
Reference
Eijsvogels TMH, Kim JH, Aengevaeren VL, et al. Masters Athletes With Abnormal Cardiovascular Findings: A Clinical Consensus Statement of the European Association of Preventive Cardiology of the ESC and the American College of Cardiology. J Am Coll Cardiol. 2026. doi:10.1016/j.jacc.2026.03.025 https://www.jacc.org/doi/10.1016/j.jacc.2026.03.025
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















