

A Weight Loss Drug Just Cut Heart Attacks and Strokes by 20 Percent. And You Don't Need Diabetes to Benefit
Jul 15, 2026
Ozempic Cuts Heart Attacks and Strokes by 20 Percent In Non Diabetics
I have been a huge proponent of GLP1 medications since they first hit the market in 2005. I also run a cardiometabolic, obesity, and weight loss clinic and jumped on the modern GLP1 medications early in 2019.
People think that all of the cardiometabolic benefits of GLP1 medications comes from weight loss alone. This is not true. People at every level of obesity and at every BMI had improved cardiovascular benefit.
Most cardiologists spend their careers waiting for a drug to move the needle on cardiovascular outcomes in people with obesity. The SELECT trial just delivered that drug, and the results are impossible to ignore.
What the Research Shows
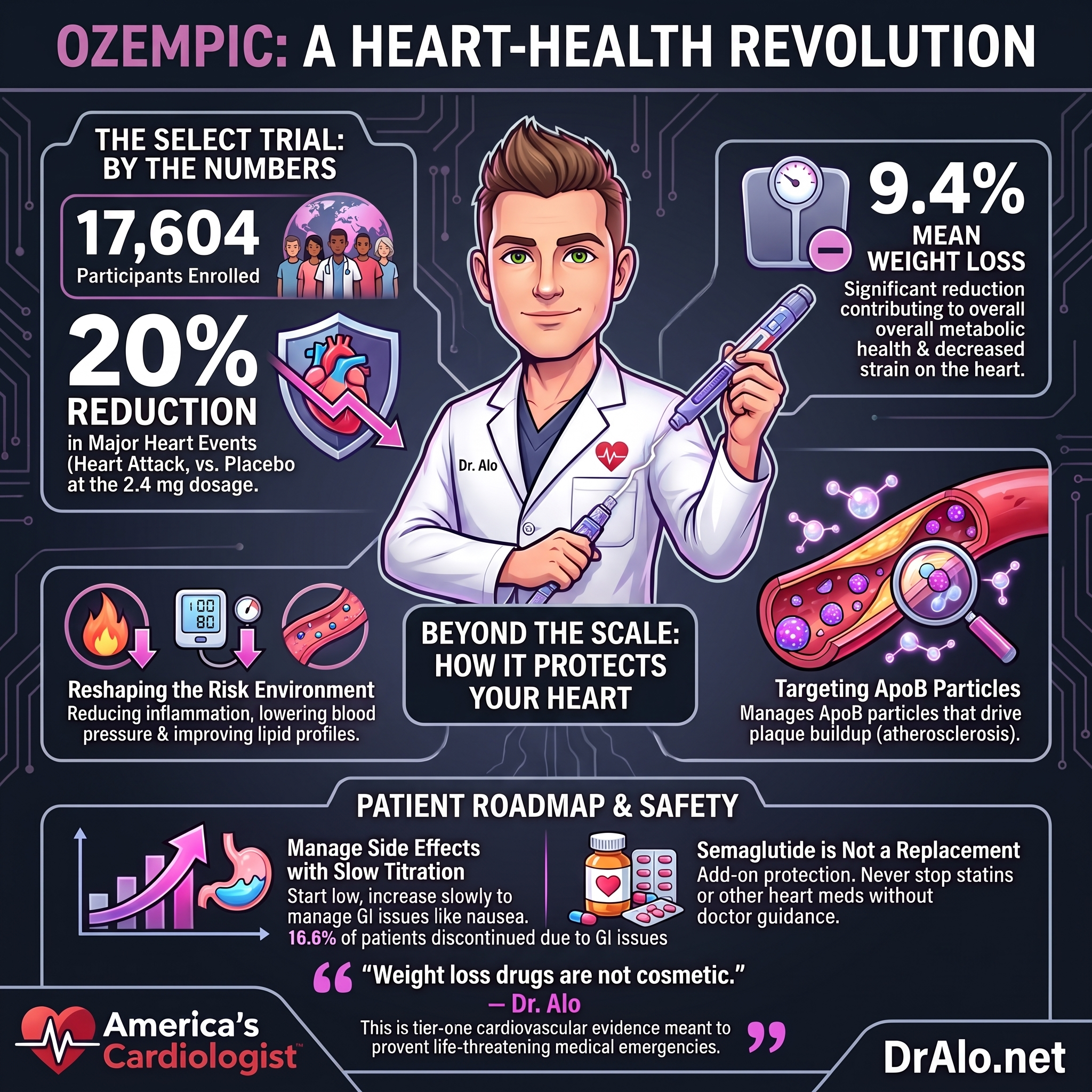
The SELECT trial enrolled 17,604 adults aged 45 and older. Every single participant had preexisting cardiovascular disease and a body mass index of 27 or greater. None of them had diabetes. That last part is critical, because until now, semaglutide's cardiovascular benefits had been studied primarily in diabetic populations.
Participants received either once-weekly subcutaneous semaglutide 2.4 mg (Wegovy) or a placebo. The researchers followed them for a mean of 39.8 months, just over three years. The primary outcome was a major adverse cardiovascular event, what we call MACE: death from cardiovascular causes, nonfatal heart attack, or nonfatal stroke.
The result was a 20 percent relative risk reduction. A primary cardiovascular event occurred in 6.5 percent of the semaglutide group compared to 8.0 percent in the placebo group. The hazard ratio was 0.80, with a 95 percent confidence interval of 0.72 to 0.90, and a P value less than 0.001. In medicine, that is a definitive result.
Infographic Summary:
Why This Matters for Your Heart
Here is what I want every patient with obesity and heart disease to understand. We have long known that excess body weight drives inflammation, raises triglycerides, increases blood pressure, and contributes to a pattern of metabolic dysfunction that accelerates atherosclerosis, the buildup of plaque in your arteries. That plaque is what ruptures and causes heart attacks.
For decades, we told patients to lose weight and hoped lifestyle changes would stick. They rarely did. Now we have a pharmacological tool that produces real, sustained weight loss and directly reduces the risk of heart attack and stroke in people who are at the highest risk.
The mean weight loss in the semaglutide group was 9.4 percent of body weight. That is significant. But here is the part that every researcher in this field is now wrestling with: the cardiovascular benefit in SELECT appeared to go beyond what weight loss alone explains. The cardiometabolic effects of semaglutide, including reductions in inflammation, improvements in blood pressure, and favorable changes in lipid profiles, all likely contribute. The drug does not just shrink the waistline. It reshapes the cardiovascular risk environment.
From an ApoB perspective, this matters. ApoB is the protein that carries atherogenic particles through your bloodstream. Triglyceride-rich lipoproteins, LDL particles, and VLDL all carry ApoB. Obesity drives up ApoB-containing particle count. Any intervention that reduces cardiovascular events in a high-risk obese population is almost certainly working in part through the lipid and inflammatory pathways that ApoB tracks so precisely.
The Evidence
Here is exactly what the SELECT trial found:
✅ 17,604 participants enrolled, all with established cardiovascular disease, BMI of 27 or greater, and no diabetes
✅ Primary MACE event rate: 6.5 percent in the semaglutide group versus 8.0 percent in the placebo group
✅ Hazard ratio of 0.80 means a 20 percent relative reduction in the risk of heart attack, stroke, or cardiovascular death
✅ 95 percent confidence interval: 0.72 to 0.90, meaning the true effect falls within that range with high certainty
✅ P value less than 0.001, which is statistically decisive
✅ Mean follow-up: 39.8 months
✅ Mean weight loss with semaglutide: 9.4 percent of body weight
✅ Serious adverse events leading to discontinuation: 16.6 percent in the semaglutide group versus 8.2 percent in the placebo group
That last number is a bit concerning. The discontinuation rate for serious adverse events was nearly double in the semaglutide group. Gastrointestinal side effects are the most common driver of stopping this medication. Nausea, vomiting, and diarrhea are real. They are manageable for many patients, but not all.
As someone who has managed thousands of patients on Ozempic and other GLP1s, we can usually adjust the meds and doses to avoid side effects. In 20 years of practice, I can say there were only 2 patients that truly couldn't tolerate any GLP1 meds.
What You Can Do
If you have cardiovascular disease and your BMI is 27 or greater, have a direct conversation with your cardiologist about semaglutide. Bring this trial to the appointment if you need to.
Ask your doctor to check your ApoB, fasting insulin, triglycerides, and blood pressure together. Get the full metabolic picture before and after starting any GLP-1 therapy.
Do not stop statins or other proven cardiovascular medications. Semaglutide adds to your protection. It does not replace the foundation.
Expect the first four to eight weeks to be the hardest. Dose titration matters. Starting at the full 2.4 mg immediately is not how the drug works. Slow titration reduces side effects.
Track your weight monthly. A 9 percent reduction in a 250-pound person is 22.5 pounds. That is a meaningful, measurable goal.
Talk to your doctor about whether you need continuous glucose monitoring even without a diabetes diagnosis. Semaglutide changes how your body handles blood sugar, and tracking that response is useful data.
Statistical Summary
- 17,604: Number of adults enrolled in the SELECT trial, all with cardiovascular disease and obesity but no diabetes
- 20%: Relative reduction in major cardiovascular events with semaglutide 2.4 mg compared to placebo
- 6.5% vs 8.0%: Actual event rates in the semaglutide group versus the placebo group over roughly 3.3 years
- 9.4%: Mean body weight lost by participants taking semaglutide during the trial
- 0.80: The hazard ratio, the single number that tells you how much lower your cardiovascular risk becomes on this drug
- 16.6%: Percentage of semaglutide patients who stopped the drug due to serious adverse events, compared to 8.2 percent on placebo
Bottom Line
The myth I need to bury today is this one: weight loss drugs are cosmetic. They are not. The SELECT trial proves that semaglutide prevents heart attacks and strokes in people who are overweight or obese and already living with cardiovascular disease. This is tier-one cardiovascular evidence.
A 20 percent reduction in MACE over 39.8 months is the kind of outcome that changes clinical guidelines. The drug is not without risk. The discontinuation rate from adverse events is real and your cardiologist needs to manage that with you carefully.
But if you have heart disease and obesity, this conversation can no longer wait.
My challenge to you is direct: when did you last have a serious, data-driven discussion with your cardiologist about your metabolic risk, not just your cholesterol number? If the answer is never, that appointment is overdue.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















