

Statins In Primary And Secondary Prevention! What the Latest Data Shows!
Jul 17, 2026
Four Types of Prevention and the Power of Lowering LDL
The old model of preventing heart disease had two categories. Modern cardiology has four, and knowing where you fall could change the course of your life.
Cardiovascular disease remains the leading cause of death worldwide, claiming nearly 18 million lives every year. For decades, our approach to preventing it came in exactly two flavors: you either had not had an event yet, or you had. That was the whole map. Today the map is far more detailed, and that detail matters, because it tells us how early we can intervene and how much disease we can prevent before it ever starts.
Here is the single truth that drives everything below: the lower your achieved LDL-C, the greater the reduction in cardiovascular events. Statins are the most proven way to get there, and there is no serious doubt that lowering LDL-C results in fewer events, lower mortality, and better outcomes.
The Old Model: Primary and Secondary Prevention
In the classical literature, primary prevention meant reducing your risk of an event before you ever had one. In plain terms: preventing a heart attack, stroke, or peripheral artery disease before the first one ever happens.
Secondary prevention classically meant reducing your risk of the next event after you had already had one. You already have clinical atherosclerotic cardiovascular disease (ASCVD), so how do you prevent the second heart attack or stroke? Here the evidence is even stronger and the treatment targets are more aggressive. That was the entire paradigm for a long time, and it was all we had. Things have changed.
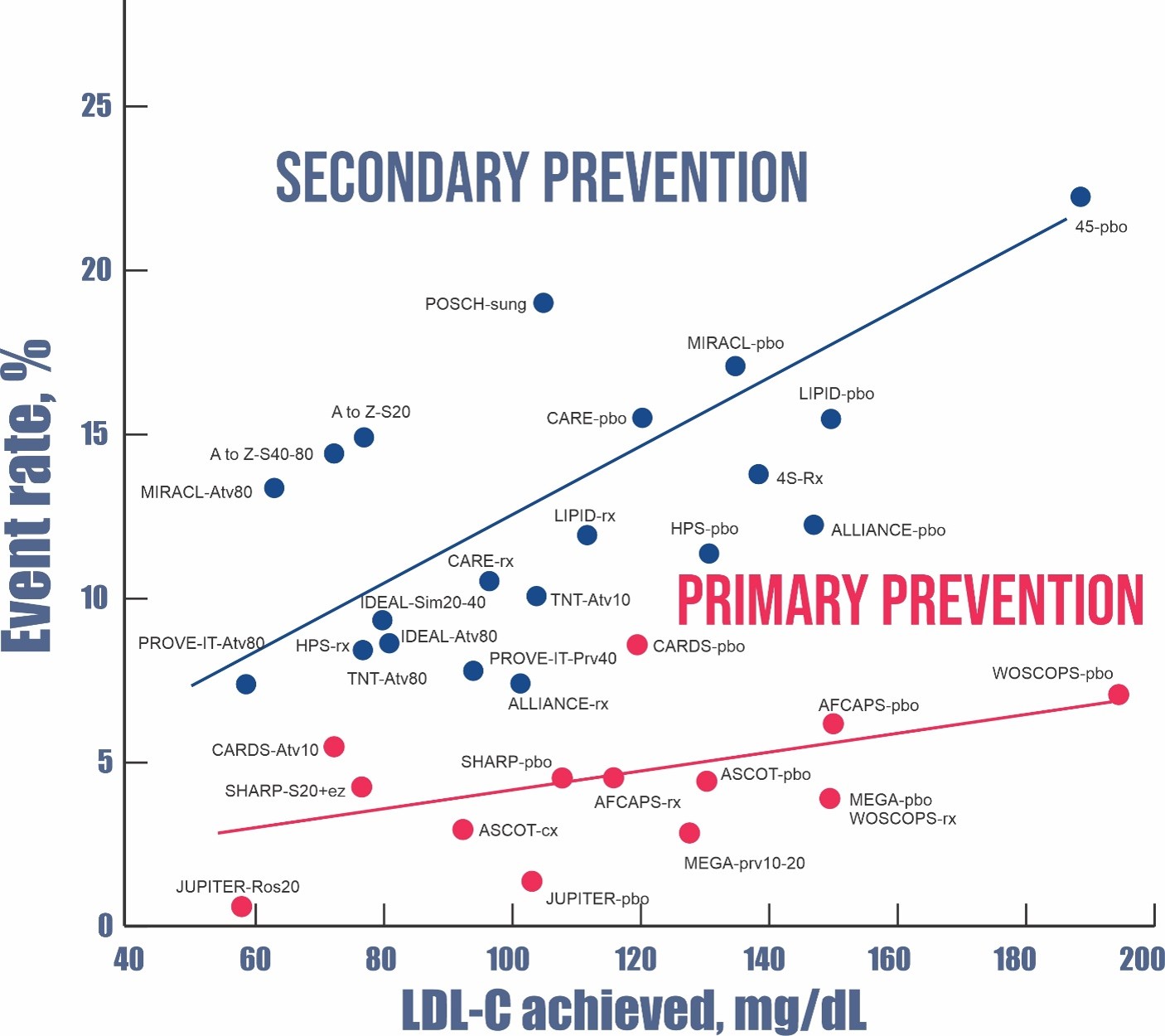
The below chart is a nice chart comparing reduction in cardiovascular disease (CVD) event rates in “classical” Primary versus Secondary Prevention.
The New Model: Four Types of Prevention
In today’s nomenclature, prevention is a spectrum that begins long before any symptoms and continues well after a first event. Here is how the modern framework breaks down:
- Primordial prevention. Preventing plaque from ever developing in the first place, long before any event and even before the risk factors take hold.
- Primary prevention. Reducing risk in people who are considered “at risk” but have not yet had an event.
- Secondary prevention. In the modern definition, this applies when imaging has demonstrated plaque, but an event has not yet occurred.
- Tertiary prevention. Treating after an initial event has already happened. This is what the classical model used to call secondary prevention.
- Quaternary prevention. Preventing a second, third, or subsequent event.
Why draw these lines so carefully? Because your chance of having another cardiovascular event is much higher once you have already had one. The categories are not academic. They tell us how aggressively to act and how much room there is to change your future.
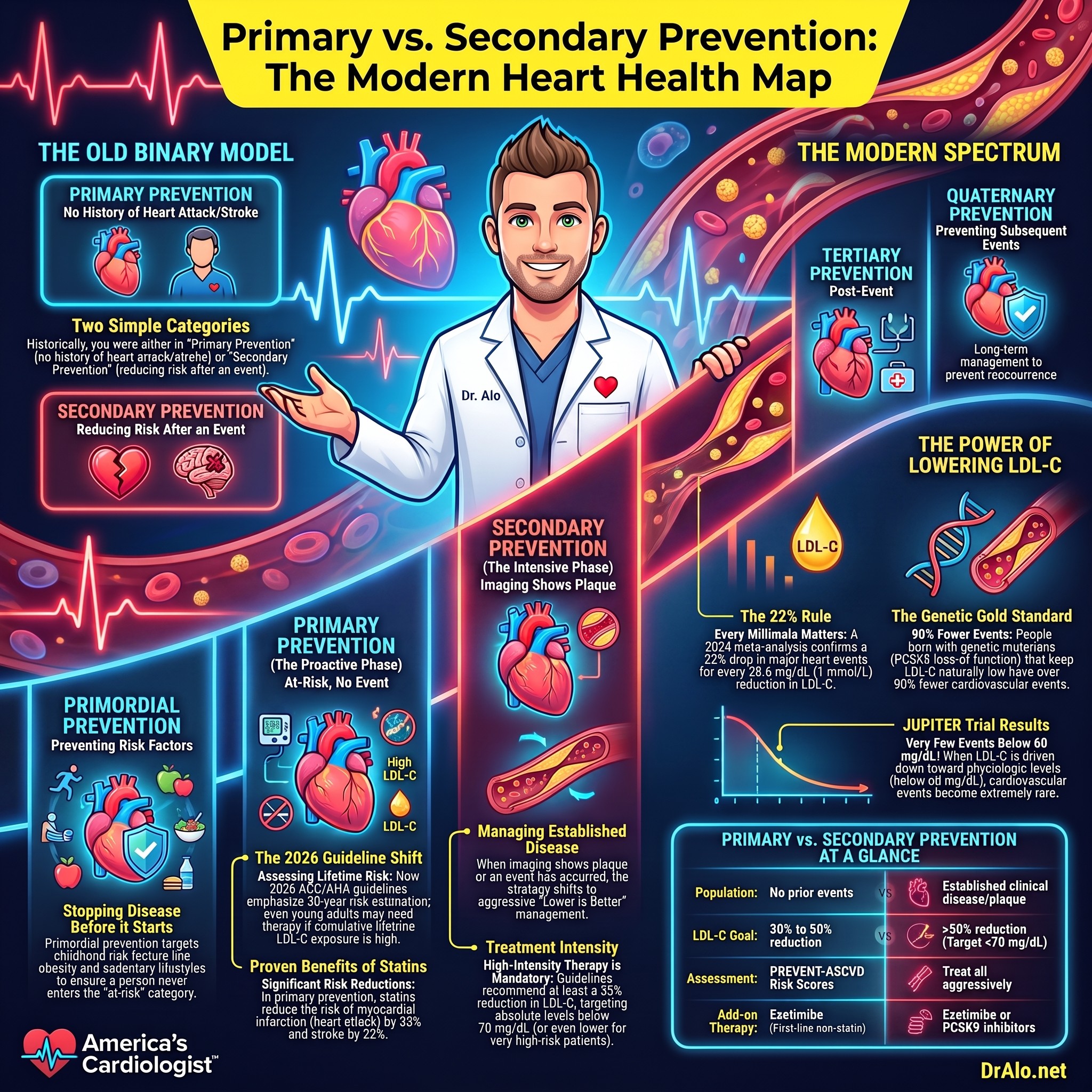
Infographic Summary:
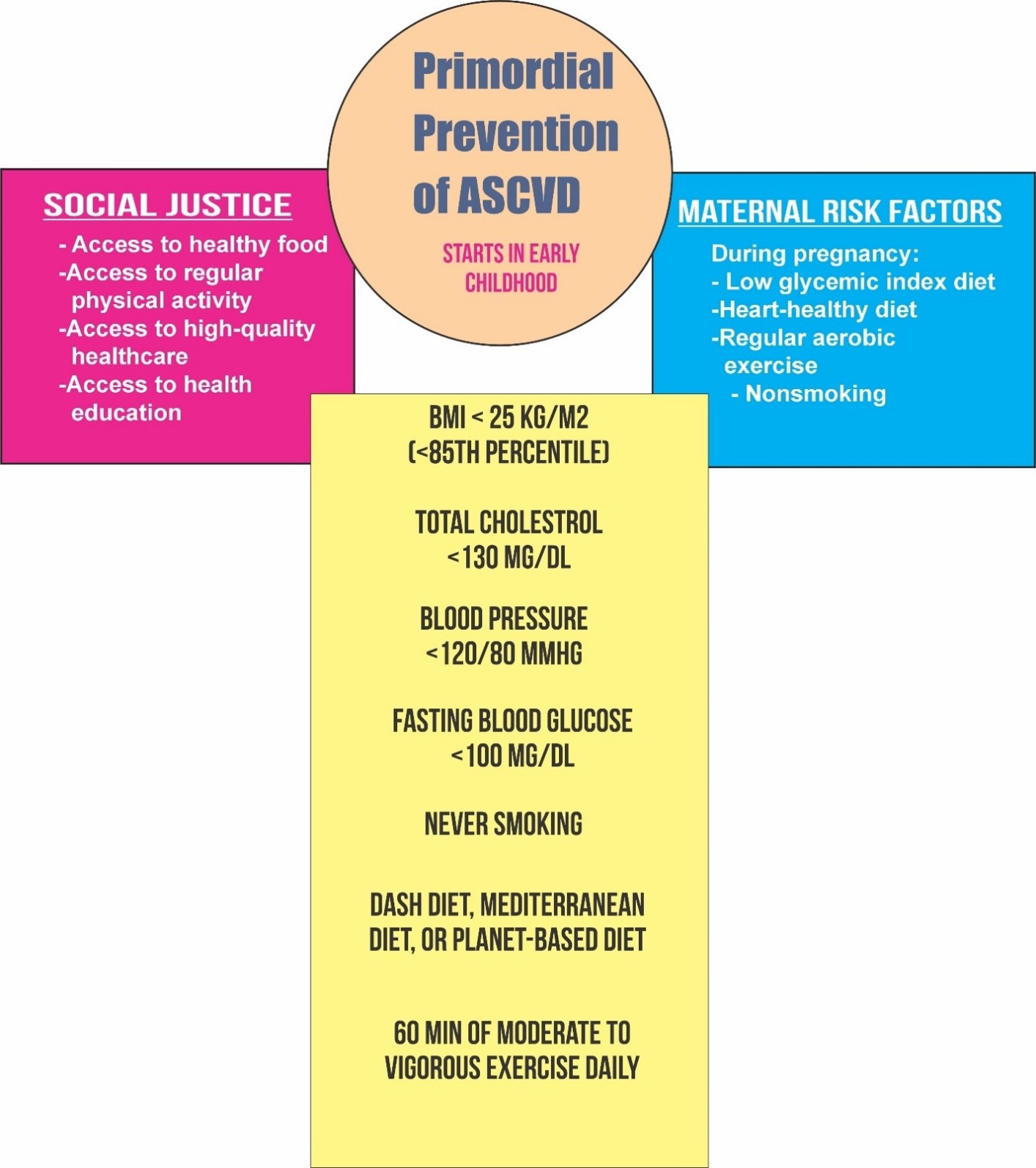
What Is Primordial Prevention?
Here is a question worth sitting with. What if we could prevent heart disease before primary prevention even becomes necessary? Primary and secondary prevention both work on people who are already at risk. What if we could take them out of the at-risk category altogether?
That is primordial prevention. It is the effort to eliminate the risk factors for heart disease so that a person is never at risk for ASCVD in the first place, and never needs primary prevention later in life.
So how do we attack it? We screen children for obesity, smoking, high blood pressure, cholesterol, activity levels, social determinants of health, food poverty, diabetes, and the many other risk factors, so that in the future they will not need primary prevention at all. Childhood obesity rates are at an all-time high. More children and teenagers are sedentary, eating a lipid-raising diet, and starting to vape or smoke than in previous generations. We need to attack this problem at its root.
To be clear, I am not saying we should put children on medications. I am saying we need to start thinking about this far sooner, and stop waiting until it is too late. Reducing LDL-C earlier in life, and more aggressively, lowers the need for primary and secondary prevention down the road.
What the Prevention Studies Show
When you line up every major trial ever done on classical primary versus secondary prevention, a clear pattern emerges. The secondary prevention group (what we now call tertiary) starts out with higher LDL-C and shows a more substantial, and frankly dramatic, drop in events as LDL-C is lowered. That steep decline makes sense: these are people who already have ASCVD and have already had an event, so they are far more prone to future ones. Lower their LDL-C and the payoff is large. The classical primary prevention group had never had a cardiac event, and yet they still saw a significant reduction in first-time events as their LDL-C came down.
One landmark sits at the far end of that data: the JUPITER trial, which used 20 mg of rosuvastatin (Crestor) in people with elevated hsCRP (inflammation) regardless of their cholesterol level. Rosuvastatin is the most potent statin we have, and this was the first time we could really drive LDL-C down toward physiologic levels. They did not even use the highest dose. Twenty milligrams is considered moderately intense, and it is still quite potent. JUPITER showed that with an LDL-C below 60 mg/dL, there were very few, if any, cardiovascular events. At its highest dose, rosuvastatin can lower LDL-C by 50 to 60% depending on the person.
At a Glance: The LDL-Event Relationship
- 22% fewer major cardiovascular events for every 38.6 mg/dL (1 mmol/L) reduction in LDL-C, per a July 2024 meta-analysis
- Hazard ratio 0.78 per 1 mmol/L reduction, across data from 1996 to 2023
- Below 60 mg/dL LDL-C in JUPITER, very few cardiovascular events occurred
- 50 to 60% LDL-C reduction achievable with high-dose rosuvastatin alone
- 80 to 90% LDL-C reduction possible by stacking non-statin medications on top
That July 2024 meta-analysis, published in the journal Atherosclerosis, pooled all the data from 1996 to 2023 and found an overall hazard ratio of 0.78 per 1 mmol/L reduction in LDL-C. In other words, for every 38.6 mg/dL you lower LDL-C, you cut major cardiovascular endpoints by about 22%. The authors also asked whether the benefit held up over time. They found that in primary prevention, every 5 years brought additional lowering of major adverse cardiovascular events (MACE), while in secondary prevention the relative effect stayed stable. In their words: “Based on available RCT data with limited follow-up duration, the relative treatment effects of LDL-C reduction are stable over time in secondary prevention, but may attenuate with higher age in primary prevention.”
And we are no longer limited to statins. By stacking a few non-statin medications, we can now reach an 80 to 90% reduction in LDL-C, which has produced remarkable reductions in ASCVD. The lower the achieved LDL-C, the more significant the reduction in event rates.
Statins in Primary Prevention
So who should actually start a statin before they have ever had an event? The decision is guided by cardiovascular risk assessment, and two major sets of recommendations shape current practice.
The 2026 ACC/AHA Dyslipidemia Guideline is the most up-to-date guidance. It recommends statin therapy for adults aged 30 to 79 years with LDL cholesterol between 70 and 189 mg/dL, with treatment intensity guided by 10-year ASCVD risk calculated using the newer PREVENT-ASCVD risk equations. For individuals at high risk (a 10-year risk of 10% or greater), high-intensity statin therapy targeting an LDL-C below 70 mg/dL is recommended. A major update in this guideline is its emphasis on 30-year risk estimation and cumulative lifetime LDL-C exposure. Even younger adults with less than 3% 10-year risk may now be considered for lipid-lowering therapy if their 30-year risk is 10% or greater, or their LDL-C is 160 mg/dL or higher. This is a paradigm shift toward earlier, more proactive intervention, and it echoes exactly what primordial prevention is about.
The U.S. Preventive Services Task Force (USPSTF) 2022 recommendation takes a slightly more conservative approach. It recommends statins for adults aged 40 to 75 with at least one CVD risk factor (dyslipidemia, diabetes, hypertension, or smoking) and a 10-year CVD risk of 10% or greater (a Grade B recommendation). For those with a risk of 7.5% to less than 10%, selective use is recommended (Grade C). Notably, the USPSTF found insufficient evidence to make a recommendation for adults 76 years and older.
Special Populations Who Warrant a Statin Regardless of Risk Score
- Severe hypercholesterolemia (LDL-C 190 mg/dL or higher). These patients face markedly elevated lifetime risk and should receive high-intensity statin therapy.
- Adults with diabetes. Diabetes is a significant independent risk factor for ASCVD, and statin therapy is recommended for most diabetic adults.
What the Evidence Shows
A comprehensive systematic review conducted for the USPSTF, encompassing 22 randomized controlled trials and over 90,000 participants, found that statins in primary prevention significantly reduced:
- All-cause mortality (relative risk 0.92)
- Myocardial infarction (relative risk 0.67)
- Stroke (relative risk 0.78)
- Composite cardiovascular outcomes (relative risk 0.72)
Just as importantly, these benefits came without significant increases in serious adverse events, muscle pain (myalgias), or cancer, which addresses some of the most common concerns patients raise about statins.
Statins in Secondary Prevention
For patients with established ASCVD, the evidence is overwhelming and the approach is more straightforward: treat aggressively. This is the “lower is better” paradigm in its purest form.
The 2026 ACC/AHA guideline recommends high-intensity statin therapy for all patients with clinical ASCVD aged 75 or younger, targeting at least a 50% reduction in LDL-C and an absolute LDL-C goal below 70 mg/dL. A notable change in the 2026 update is that ezetimibe is no longer required before adding a PCSK9 inhibitor. Either agent may be added based on how much additional LDL-C lowering is needed and on patient preference.
Not every secondary prevention patient carries the same risk. Those classified as very high-risk ASCVD, defined by multiple major cardiovascular events, or one major event plus high-risk conditions such as diabetes, age over 65, current smoking, hypertension, or LDL-C above 100 mg/dL on maximally tolerated therapy, warrant intensification with non-statin agents. And reassuringly, current evidence supports the long-term safety of achieved LDL-C levels as low as 30 mg/dL, with no signal that we need to back off at very low levels.
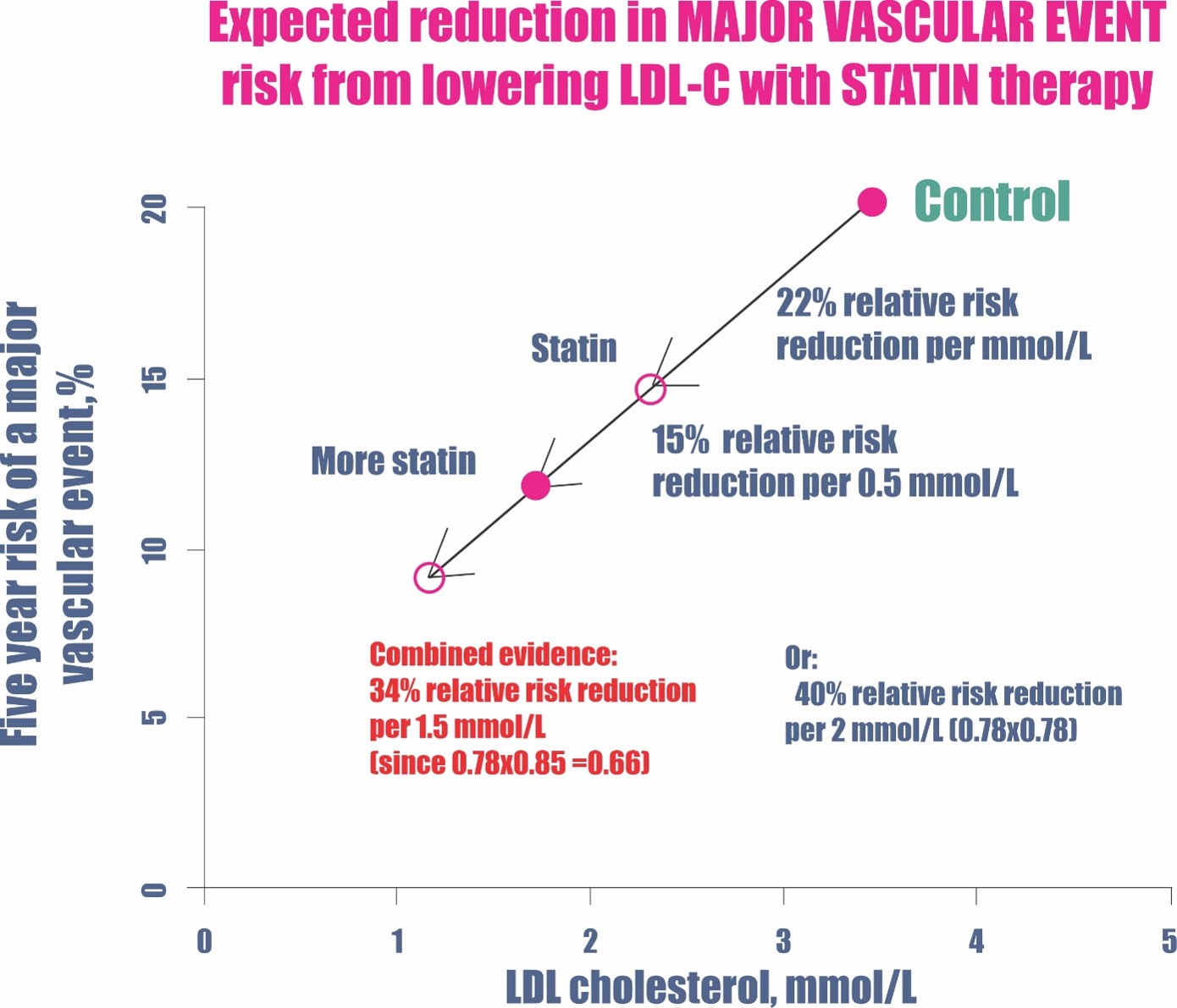
The Cholesterol Treatment Trialists’ (CTT) Collaboration meta-analysis of high- versus low-intensity statin regimens in secondary prevention showed an additional 15% reduction in major vascular events with more intensive therapy. The proportional benefit works out to roughly a 19% relative risk reduction per 1 mmol/L (39 mg/dL) reduction in LDL cholesterol, a relationship that holds consistently across subgroups. The VA/DoD Clinical Practice Guideline adds a pragmatic layer, using moderate-dose statins as the foundation and offering high-dose therapy through shared decision-making, preferentially to higher-risk patients such as those with recent acute coronary syndrome, recurrent events, or multivessel disease combined with diabetes or smoking.
Primary and Secondary Prevention at a Glance
| Feature | Primary Prevention | Secondary Prevention |
|---|---|---|
| Population | No prior ASCVD events | Established clinical ASCVD |
| Statin intensity | Moderate to high (risk-based) | High-intensity preferred |
| LDL-C goal | At least 30 to 50% reduction (risk-based); below 70 mg/dL if high risk | At least 50% reduction and below 70 mg/dL |
| Risk assessment | PREVENT-ASCVD (10-year and 30-year) | Not applicable: treat all |
| Add-on therapy | Ezetimibe as first-line non-statin | Ezetimibe or PCSK9 inhibitor |
| Evidence for age over 75 | Insufficient | Continuation reasonable |
Safety: Addressing Common Concerns
Statins are among the most extensively studied medications in history, and their safety profile is well established. In primary prevention trials, statins were not significantly associated with increased serious adverse events, myalgias, or cancer.
The one real safety consideration is a modest increase in new-onset diabetes with high-intensity therapy, a relative risk of about 1.25. But that risk is generally outweighed by the cardiovascular benefit in anyone whose 10-year ASCVD risk exceeds roughly 3%. For most patients, the net clinical benefit of statin therapy is strongly favorable.
What About Genetics? Mendelian Randomization
Some people are dealt their cards at birth. There are genetic mutations that confer either protection or harm, and these people cannot change their genes. This is the basis of Mendelian randomization: at birth, you were effectively randomized into carrying a mutation or not. It gives us some of the cleanest data in all of cardiology, because no medication is involved. The differences in outcome come purely from lifelong differences in LDL-C.
Consider the two extremes:
| Genetic mutation | Effect on LDL-C and risk |
|---|---|
| LDLR mutation (dysfunctional LDL receptor) | Very high LDL-C, higher event rates |
| PCSK9 loss-of-function mutation | About 40 mg/dL lower LDL-C, 90% or more fewer events |
At one end are people with an LDLR mutation that leaves the LDL receptor dysfunctional. Their bodies cannot clear LDL particles from circulation well, so their LDL-C runs very high. There are six common types of LDLR mutations, plus many rare ones.
At the other end are people born with a PCSK9 loss-of-function (LOF) mutation. The PCSK9 gene normally regulates how long LDL receptors survive. When PCSK9 is barely produced, the LDL receptor is not degraded and lives longer, clearing more LDL from the blood. These individuals have LDL-C that is roughly 40 mg/dL lower than baseline, and they enjoy an event rate reduction of 90% or more compared to people without such low cholesterol. Every level of risk in between these two extremes is represented by other mutations.
Here is a detail that often gets missed. These are otherwise healthy people. Many do not have diabetes or inflammation, and the share who are diabetic (about 9.1%) simply mirrors the general population. In other words, neither diabetes nor inflammation is necessary for atherosclerosis to develop. LDL-C is doing the driving.
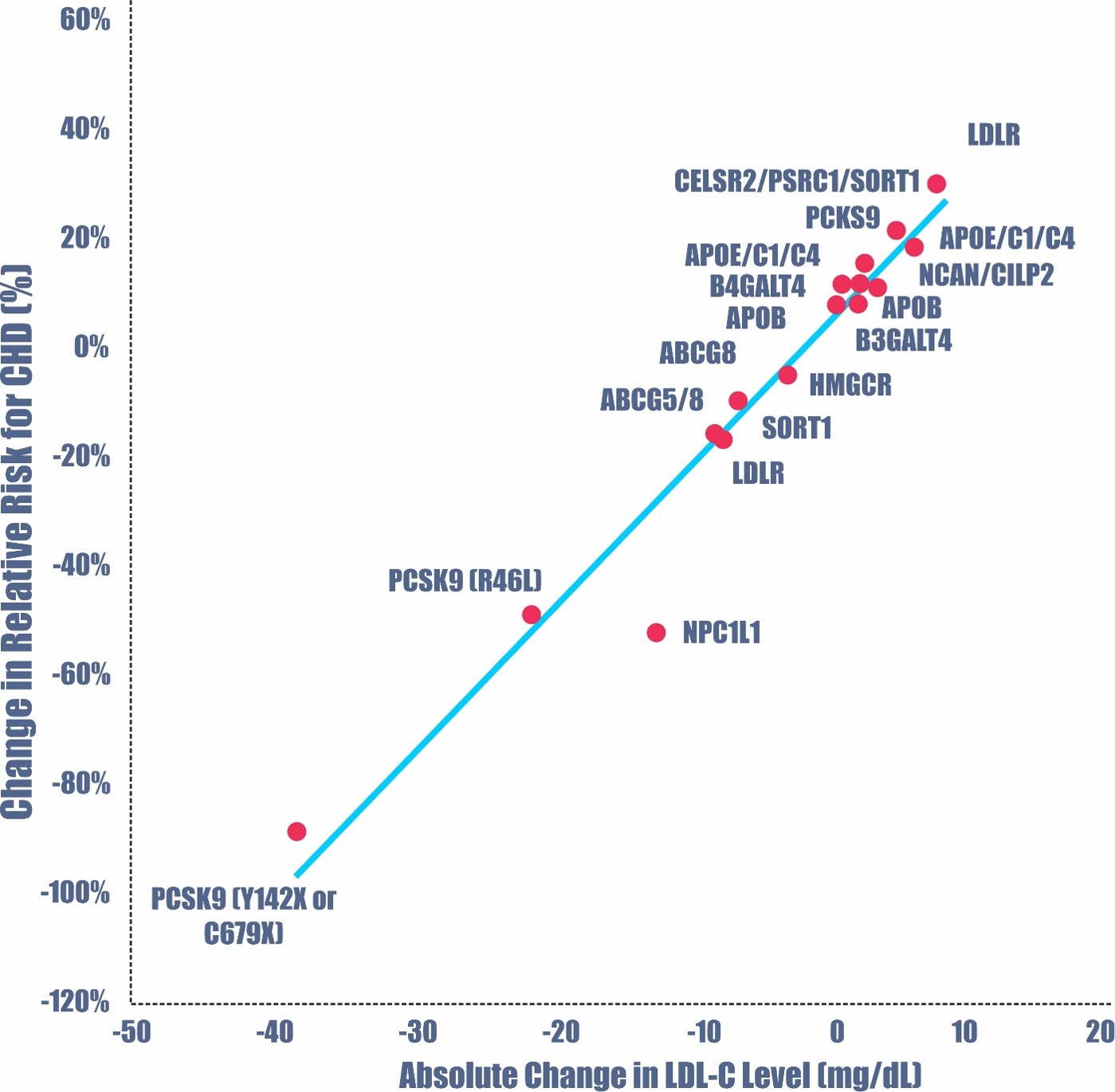
The above chart is a graphical representation of absolute change in LDL-C level versus relative changes in cardiovascular disease event rates based on genetic mutations. You’ll notice that some mutations increase LDL-C above normal, while others lower it.
This chart is not a medical intervention chart. None of these patients were given medication. These people all have genetic mutations that give them either protection or worse outcomes. This is Mendelian Randomization.
At the very top right, you see “LDLR”. These are people with a genetic mutation that renders the LDL receptor dysfunctional. This means that they are not able to clear (remove) LDL particles from circulation very well. This means that you will have very high levels of LDL-C. There are 6 common (and many rare) types of LDLR mutations, you can read about them at:
https://www.ncbi.nlm.nih.gov/books/NBK343488/table/lipid_hyperchol.T.the_six_classes_of_ldl/
At the bottom left of that chart are people born with a PCSK9 loss of function mutation (LOF) which means the gene is not active and the patients do not make much PCSK9. The PCSK9 gene regulates the production/nonproduction of PCSK9, which influences the lifespan of LDL receptors. This makes it so that the LDL receptor is not degraded and lives longer. LDL receptors will remove more LDL particles from circulation, thereby conferring protection and much lower LDL-C levels.
You’ll notice from the chart that PCSK9 LOF mutations are associated with hypobetalipoproteinemia with LDL-C that is 40 mg/dL lower than baseline and confers an event rate reduction of 90% or more compared to people without extremely low cholesterol.
Of course, you have many other genetic mutations in between these two extremes, and they confer different levels of risk reduction or increased risk.
This is the crux of Mendelian Randomization studies. People are genetically randomized to different levels of LDL-C. This gives us excellent data. These are also people who are quite healthy otherwise. Many do not have diabetes nor inflammation. The number of diabetics mirrors that of the general population, at about 9.1%. Neither diabetes nor inflammation is necessary for atherosclerosis.
More on this topic:
https://www.sciencedirect.com/science/article/pii/S1933287415004493
The Bigger Picture: Lower LDL, Fewer Events
Line up the trials across the years and the message never wavers. Back when atorvastatin (Lipitor) was the most potent statin available, it was already obvious that the lower the LDL-C, the lower the MACE. As newer and more potent therapeutics arrived, the line only got steeper.
The most recent data include the newest class of drugs, the PCSK9 inhibitors. In the ODYSSEY and OSLER trials, LDL-C fell by roughly 1.8 to 2.0 mmol/L (69 to 77 mg/dL), which translated into an over 50% reduction in MACE. The greater the reduction in LDL-C, the greater the reduction in events. And the data keep pouring in as more medications reach the market and more studies are completed.
Above is another chart showing increasing reductions in Major Adverse Cardiac Events (MACE), among different trials, using different statins and different doses with more potent LDL-C reduction.
The Bottom Line
We used to think about prevention in two boxes. Now we see a continuum that begins in childhood, long before the first plaque forms, and extends through every subsequent event. In primary prevention, the decision to start therapy should be guided by individualized risk, with the newest guidelines pushing us to consider lifetime risk and cumulative cholesterol exposure far earlier than we used to. In secondary prevention, the message is blunt: treat early, treat intensively, and do not hesitate to add non-statin therapies when goals are not met. Genetics show us the ceiling of what is possible, with lifelong low LDL-C cutting events by 90%, and modern medications increasingly let us approach that same territory on purpose.
The through-line could not be simpler. Whether the LDL-C comes down because of your genes, a statin, or a stack of modern therapeutics, lower is better, and earlier is better still.
If lifelong low LDL can cut heart attacks and strokes by 90%, why would you wait until after your first event to start lowering yours?
References
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia. J Am Coll Cardiol. 2026. https://doi.org/10.1016/j.jacc.2025.11.026
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA Dyslipidemia Guideline. Circulation. 2026. https://doi.org/10.1161/CIR.0000000000001312
- US Preventive Services Task Force, Mangione CM, Barry MJ, et al. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: USPSTF Recommendation Statement. JAMA. 2022;328(8):746-753. https://doi.org/10.1001/jama.2022.13044
- Chou R, Cantor A, Dana T, et al. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: Updated Evidence Report and Systematic Review for the USPSTF. JAMA. 2022;328(8):754-771. https://doi.org/10.1001/jama.2022.12138
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol: Executive Summary. J Am Coll Cardiol. 2019;73(24):3168-3209. https://doi.org/10.1016/j.jacc.2018.11.002
- Michos ED, McEvoy JW, Blumenthal RS. Lipid Management for the Prevention of Atherosclerotic Cardiovascular Disease. N Engl J Med. 2019;381(16):1557-1567. https://doi.org/10.1056/NEJMra1806939
- Koskinas KC, Siontis GCM, Piccolo R, et al. Effect of Statins and Non-Statin LDL-lowering Medications on Cardiovascular Outcomes in Secondary Prevention: A Meta-Analysis of Randomized Trials. Eur Heart J. 2018;39(14):1172-1180. https://doi.org/10.1093/eurheartj/ehx566
- O’Malley PG, Arnold MJ, Kelley C, et al. Management of Dyslipidemia for Cardiovascular Disease Risk Reduction: Synopsis of the 2020 Updated VA/DoD Clinical Practice Guideline. Ann Intern Med. 2020;173(10):822-829. https://doi.org/10.7326/M20-4648
- Meta-analysis of LDL-C reduction and cardiovascular endpoints, 1996 to 2023. Atherosclerosis. July 2024. https://www.atherosclerosis-journal.com/article/S0021-9150(24)01108-0/fulltext
- The relationship between achieved LDL-C and cardiovascular event reduction. Cleveland Clinic Journal of Medicine. https://www.ccjm.org/content/83/3/181
- Primordial Prevention of Atherosclerotic Cardiovascular Disease. Journal of Cardiopulmonary Rehabilitation and Prevention. 2022. https://journals.lww.com/jcrjournal/Fulltext/2022/11000/Primordial_Prevention_of_Atherosclerotic.2.aspx
- Population-based cohort data on lifetime risk factor burden. Circulation. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.115.014849
- The six classes of LDL receptor (LDLR) mutations. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK343488/table/lipid_hyperchol.T.the_six_classes_of_ldl/
- Mendelian randomization and LDL-C: genetic evidence for causality. ScienceDirect. https://www.sciencedirect.com/science/article/pii/S1933287415004493
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















