

A Pill That Cuts LDL by 57 Percent: The Oral PCSK9 Inhibitor That Changes Everything
Jul 16, 2026
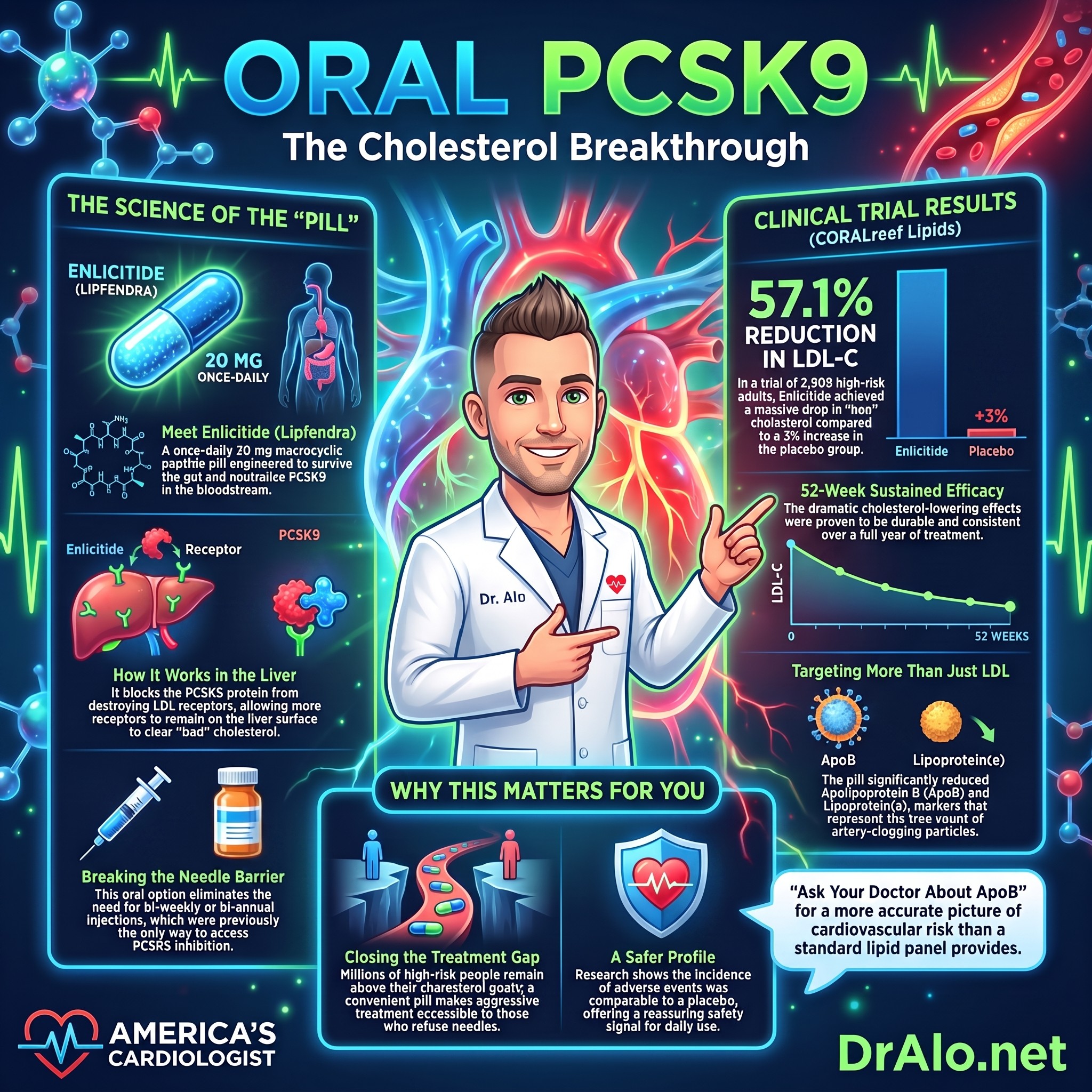
New Oral PCSK9 Breakthrough Enlicitide
A new oral PCSK9 inhibitor called enlicitide decanoate just produced results in a major randomized trial that rival injectable therapies, and the cardiovascular world needs to pay attention. High levels of low-density lipoprotein cholesterol (LDL-C), the “bad cholesterol,” are one of the most important modifiable drivers of heart attacks and strokes. For years, the most powerful non-statin tool we had for lowering it required an injection. That is no longer true.
On July 16, 2026, the U.S. FDA approved enlicitide (brand name Lipfendra) as the first and only once-daily oral PCSK9 inhibitor for lowering LDL-C in adults with hypercholesterolemia, including heterozygous familial hypercholesterolemia.
This allows us to get LDL cholesterol levels down to levels never seen before with oral medications, when combined with other medications. In my cardiology practice, we often need to get LDL cholesterol to below 40 mg/dL and sometimes lower. We could not do that with oral pills alone, and had to add injectable medications. That has all changed now. With a combination of three pills, most people can now get their LDL cholesterol into the single digits. When we combine rosuvastatin, ezetimibe, and this new medication, we can achieve a 95% reduction in LDL-C.
What Is PCSK9, and Why Does It Matter?
I want to be direct with you about what these drugs do. Your liver cells carry receptors on their surface called LDL receptors, and their job is to grab LDL-C particles out of your bloodstream and pull them into the liver for disposal. The more LDL receptors you have, the more LDL-C gets cleared from your blood.
PCSK9 (proprotein convertase subtilisin/kexin type 9) is a protein your liver produces that destroys those LDL receptors. When PCSK9 binds to a receptor, the receptor gets broken down inside the cell instead of being recycled back to the surface. Fewer receptors means more LDL floating in your blood, more plaque building in your arteries, and more risk of a heart attack or stroke.
PCSK9 inhibitors block that process. When you neutralize PCSK9, those receptors survive, get recycled to the cell surface, and keep pulling LDL out of circulation. The effect is dramatic, and LDL-C can drop by 50 to 60% or more.
Infographic Summary:
The Problem with Existing PCSK9 Inhibitors
Before enlicitide, the PCSK9 inhibitors on the market all required needles. Evolocumab (Repatha) and alirocumab (Praluent) are monoclonal antibodies: large, complex proteins injected under the skin every two to four weeks. A third option, inclisiran (Leqvio), uses small interfering RNA but still requires injections given by a healthcare provider twice a year.
These drugs are extraordinarily effective, and the outcomes evidence behind them, from trials like FOURIER for evolocumab and ODYSSEY Outcomes for alirocumab, is iron-clad. But a significant portion of eligible patients never start them, or discontinue within months. The reason is simple: injections, plus prior-authorization hurdles and cost. For many people, the needle alone is a deal-breaker. The result is that a large share of high-risk patients, including people who have already had a heart attack or stroke, still don’t reach their recommended LDL-C goals.
Enter Enlicitide: A Pill That Does What Injections Do
Enlicitide (developed as MK-0616) is a macrocyclic peptide: a small, ring-shaped molecule engineered to mimic the binding action of large antibodies, but in a form small enough to be absorbed through the gut. It’s taken as a 20 mg tablet once daily on an empty stomach, formulated with a permeation enhancer (sodium caprate) that helps it cross the intestinal lining and reach the bloodstream. Engineering a peptide that can survive the harsh environment of the GI tract, cross the intestinal wall, and neutralize a target protein in the blood is a genuinely remarkable pharmaceutical achievement.
Once absorbed, enlicitide binds circulating PCSK9 and prevents it from interacting with LDL receptors on liver cells. The end result is the same as the injectables: more LDL receptors, more LDL-C clearance, lower cholesterol, all from a pill.
What the Research Shows
The pivotal evidence comes from CORALreef Lipids, a Phase 3 multinational, double-blind, randomized, placebo-controlled trial that enrolled 2,909 adults. These were not low-risk patients. Every participant either had a history of a major atherosclerotic cardiovascular disease (ASCVD) event with an LDL of 55 mg/dL or higher, or was at risk for a first event with an LDL of 70 mg/dL or higher. The average LDL at baseline was 96.1 mg/dL, a population that needs serious lipid-lowering and often isn’t getting it.
Participants were randomized 2-to-1 to enlicitide 20 mg once daily or placebo for 52 weeks, with the primary endpoint being percent change in LDL-C from baseline to week 24. The result was decisive: enlicitide produced a mean LDL reduction of 57.1% at week 24, while placebo produced a 3.0% increase. The adjusted between-group difference was 55.8 percentage points lower with enlicitide (95% CI, 50.7 to 60.9 points; p < 0.001). That is not a modest effect. That is a treatment-level shift in cardiovascular risk. And the reductions held through week 52, confirming this is not a short-lived spike.
At a Glance: CORALreef Lipids
- 57.1% mean LDL-C reduction with enlicitide at 24 weeks
- 55.8 percentage points greater reduction than placebo (p < 0.001)
- 2,909 adults enrolled, both high-risk and very-high-risk
- 96.1 mg/dL mean baseline LDL-C across the trial population
- 52 weeks over which the reductions were sustained
- 39.3% of participants were women
The Evidence
Here are the key data points from CORALreef Lipids:
| Participants (enlicitide / placebo) | 1,935 / 969 |
| Mean baseline LDL-C | 96.1 mg/dL |
| LDL-C change at week 24 (enlicitide) | 57.1% reduction |
| LDL-C change at week 24 (placebo) | 3.0% increase |
| Adjusted difference at week 24 | 55.8 points lower (p < 0.001) |
| LDL-C reductions at week 52 | Sustained (p < 0.001) |
| Non-HDL cholesterol at week 24 | Greater reduction |
| Apolipoprotein B at week 24 | Greater reduction |
| Lipoprotein(a) at week 24 | Greater reduction |
| Adverse-event incidence | No difference vs. placebo |
| Mean age | 63 years |
The apolipoprotein B finding deserves emphasis. ApoB is the protein that sits on every atherogenic lipoprotein particle: LDL, VLDL, and IDL. When ApoB drops, the total burden of artery-clogging particles drops. LDL cholesterol tells you the cholesterol content; ApoB tells you the particle count, and particle count is what drives plaque. Enlicitide reduced both, which means it is attacking atherosclerosis at multiple levels simultaneously.
The lipoprotein(a) reduction matters too. Lp(a) is a genetically determined cardiovascular risk factor that very few therapies touch meaningfully. A statistically significant reduction in Lp(a) adds another dimension of potential benefit beyond standard LDL lowering.
Why This Matters for Your Heart
A once-daily pill changes the conversation entirely. A patient who refuses an injection will take a pill. That is not a hypothetical. That is basic human behavior. By extending the reach of PCSK9 inhibition to millions of patients who would otherwise go undertreated, an oral option could finally start closing the enormous gap between the people who need aggressive lipid lowering and the people who actually receive it.
Why an oral PCSK9 inhibitor is a big deal
- Accessibility. Removing the needle removes the single biggest barrier to PCSK9 inhibitor use. For most patients, a daily pill is far more acceptable than self-injecting or visiting a clinic.
- Closing the treatment gap. Millions of high-risk people remain above their LDL-C goals despite available therapies. A convenient, effective oral option can help reach them.
- Broad lipid effect. Enlicitide lowered not just LDL-C, but also non-HDL-C, ApoB, and Lp(a), the markers that best capture true atherogenic particle burden.
What You Can Do
Ask your cardiologist or primary care physician to measure your ApoB, not just your LDL. A standard lipid panel misses part of the picture of your cardiovascular risk.
Know your numbers. An LDL below 70 mg/dL is the guideline target for high-risk patients, and below 55 mg/dL for very-high-risk patients, with below 40 mg/dL increasingly the goal in recent cardiovascular outcome trials.
If you’ve been told you need a PCSK9 inhibitor but avoided starting one because of the injection, an oral option is now available. Tell your doctor: you may be an ideal candidate, and that conversation is worth having now.
Do not stop your statin without talking to your cardiologist. Enlicitide was studied on top of existing therapy. It’s an addition to the treatment ladder, not a replacement for it, and it’s no substitute for a healthy diet and regular exercise, either.
Follow the outcomes data. CORALreef Lipids demonstrates powerful LDL lowering; what the field needs next is proof that this translates into fewer heart attacks and strokes. That trial, CORALreef Outcomes, is already underway.
The Bottom Line
The myth that effective PCSK9 inhibition requires an injection is now under direct scientific challenge. CORALreef Lipids, a Phase 3 trial with a 52-week follow-up window, shows that a once-daily oral pill can cut LDL by more than 57% over six months, with a safety profile comparable to placebo. The reductions extended to ApoB and lipoprotein(a), the two markers that tell us the most about true atherogenic particle burden.
We do not yet have hard cardiovascular outcome data for enlicitide. The FDA approval rests on its powerful effect on cholesterol, and the CORALreef Outcomes trial still has to show that lower numbers mean fewer events. But the mechanistic foundation is solid, the LDL reductions are comparable to injectable PCSK9 inhibitors, and the safety signal is reassuring.
If a daily pill could reduce your risk of a heart attack or stroke by lowering your LDL more than 55%, what is stopping you from having that conversation with your doctor today?
References
- Merck. LIPFENDRA (enlicitide) is the First and Only Once-Daily Oral PCSK9 Inhibitor Approved by the U.S. FDA. July 2026.
- A Placebo-Controlled Trial of the Oral PCSK9 Inhibitor Enlicitide (CORALreef Lipids). N Engl J Med. February 5, 2026.
- American College of Cardiology. CORALreef Lipids: Oral PCSK9 Inhibitor Enlicitide Reduces LDL-C in High-Risk Patients. February 2026.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















