

Best Congestive Heart Failure Treatment: What the Evidence Shows
Jul 16, 2026
Best Congestive Heart Failure Treatment: What the Evidence Shows
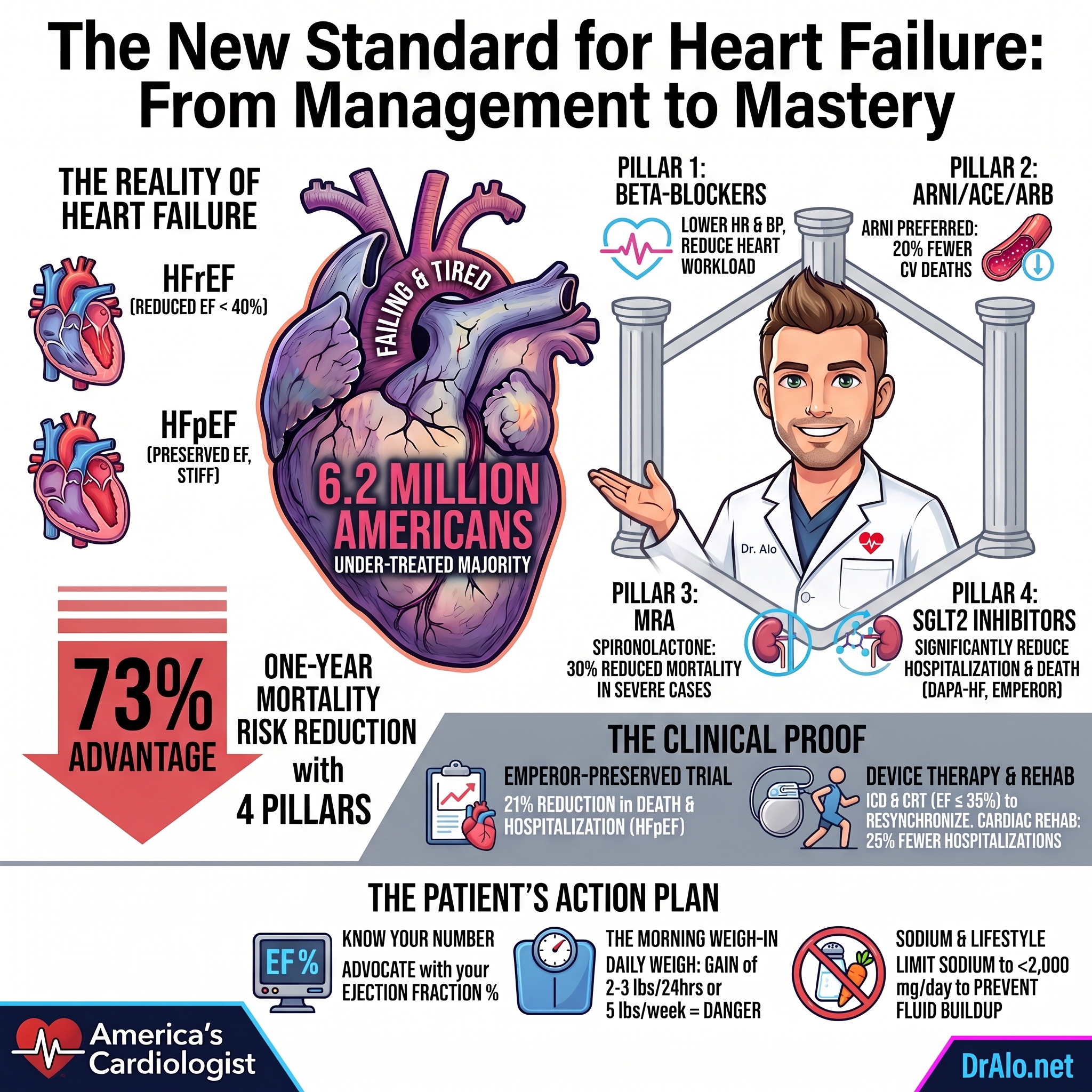
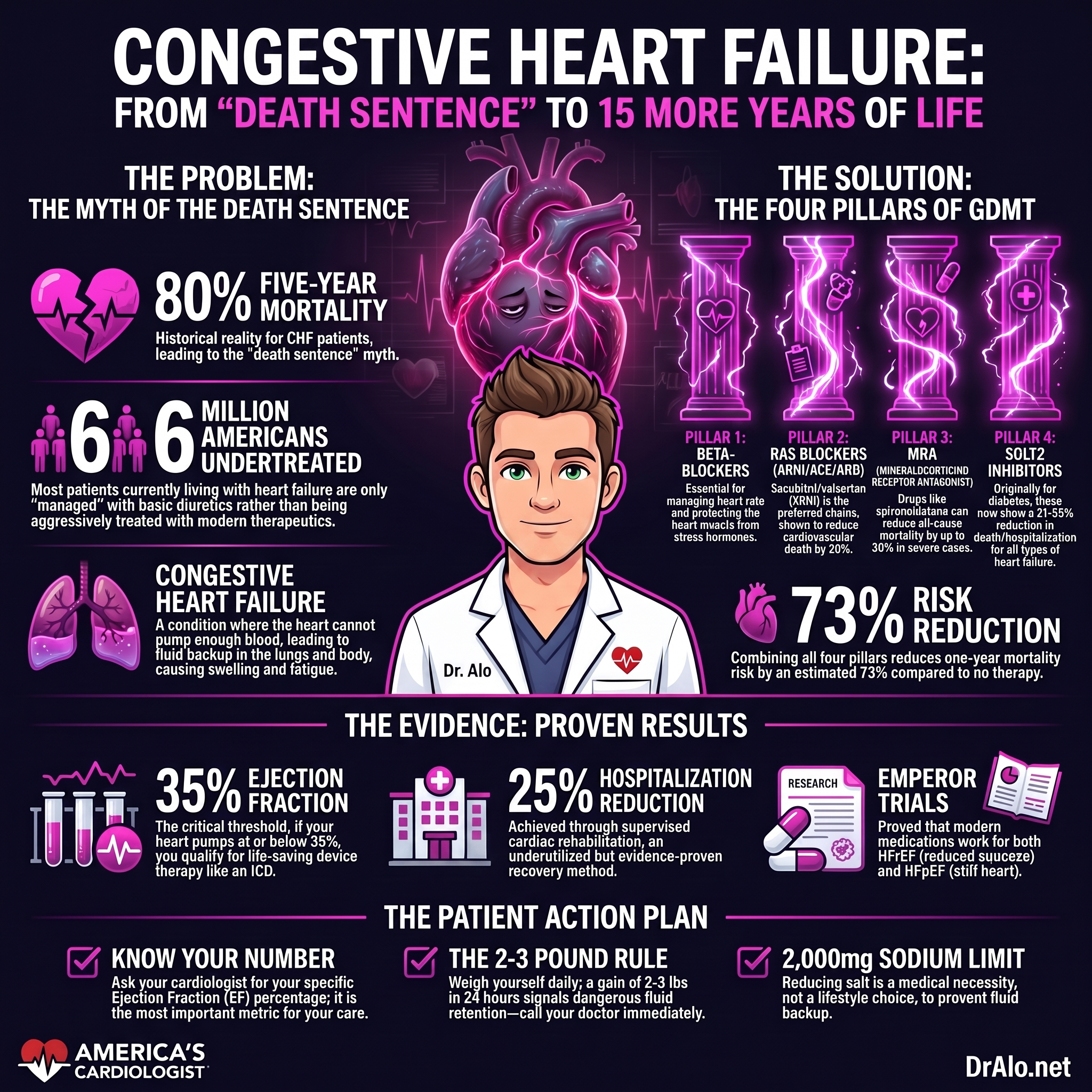
Congestive heart failure used to have an 80% five-year mortality rate. This means that in 5 years, 80% of those diagnosed with CHF would be dead. That is no longer the case. Modern medications and therapeutics have been able to add 9 to 15 years of quality life to CHF patient's lifespans. And it keeps getting better.
Congestive heart failure is no longer a death sentence, but the wrong treatment plan makes it one. Over 6 million Americans are living with heart failure right now, and the majority are undertreated. I am going to tell you exactly what the best treatment for heart failure looks like in 2026, what the clinical trials prove, and what questions every patient needs to ask before leaving their cardiologist's office.
What Is Congestive Heart Failure and Why It Gets Worse
Congestive heart failure happens when the heart cannot pump enough blood to meet the body's demands. The word "congestive" refers to the fluid backup that results. When the heart pumps inefficiently, blood backs up into the lungs and body, causing shortness of breath, leg swelling, and fatigue. The heart tries to compensate by enlarging and beating faster. Over time, those compensatory mechanisms fail, and the condition spirals.
Heart failure comes in two primary forms. Heart failure with reduced ejection fraction, called HFrEF, means the heart squeezes poorly. A normal ejection fraction is 55 to 70 percent. In HFrEF, it falls below 40 percent. Heart failure with preserved ejection fraction, called HFpEF, means the heart squeezes adequately but stiffens and fails to relax properly. Both forms kill. Both require aggressive, targeted treatment.
The single biggest driver of heart failure is uncontrolled risk factors: high blood pressure, coronary artery disease, diabetes, and obesity. If you have ever wondered why people with similar cholesterol levels develop heart disease at different ages, the answer lies in the constellation of risk factors surrounding that number, not the number alone. I covered that biological question in detail in my breakdown of the Swedish AMORIS cohort study, which revealed how survivorship bias distorts our understanding of cardiovascular risk.
What the Research Shows About the Best Treatment for Heart Failure
The evidence base for heart failure treatment is one of the strongest in all of cardiology. We have decades of randomized controlled trials proving that specific drug classes reduce hospitalizations, reverse cardiac remodeling, and extend life. The treatment framework is called guideline-directed medical therapy, or GDMT. It is not optional. It is the standard of care.
GDMT for HFrEF is built on four drug classes. Together, cardiologists call them the "Four Pillars." Each pillar has independent mortality benefit. Stacking all four cuts the risk of death more than any single agent alone. The pillars are: a beta-blocker, a renin-angiotensin system blocker (either an ACE inhibitor, ARB, or the combined ARNI sacubitril/valsartan), a mineralocorticoid receptor antagonist (MRA), and an SGLT2 inhibitor.
The SGLT2 inhibitor category deserves special attention because it represents the most important advance in heart failure treatment in the last decade. These drugs were originally developed for type 2 diabetes, but their cardiovascular benefits extended far beyond blood sugar control. The DAPA-HF Trial (dapagliflozin) and the EMPEROR-Reduced Trial (empagliflozin) both demonstrated significant reductions in cardiovascular death and worsening heart failure in patients with HFrEF, regardless of whether those patients had diabetes.
EMPEROR-Preserved Trial (empagliflozin) then changed the landscape for HFpEF, a condition that had resisted effective pharmacological treatment for years. It showed a 21 percent reduction in the composite of cardiovascular death and heart failure hospitalization. For the first time, we had a drug with proven benefit across both major forms of heart failure.
Infographic Summary:
Why This Matters for Your Heart
Let me be direct with you. If you have been diagnosed with heart failure and your doctor has not discussed all four pillars of GDMT, you are not receiving optimal care. I see this every week in my practice. Patients arrive on a diuretic and a beta-blocker alone, with no ARNI, no MRA, no SGLT2 inhibitor. They are being managed, not treated aggressively enough to change their trajectory.
The fear of side effects drives undertreatment. Beta-blockers lower heart rate and blood pressure, so physicians hold back. ACE inhibitors cause cough in 10 to 15 percent of patients, so the whole class gets abandoned instead of switching to an ARB. MRAs raise potassium, so they get skipped. Every one of these concerns is manageable with proper monitoring. The cost of avoiding these drugs is measured in hospitalizations and years of life.
Device therapy is the second major category of heart failure treatment. Patients with HFrEF and an ejection fraction at or below 35 percent, despite optimal medical therapy, qualify for an implantable cardioverter-defibrillator (ICD). Those with electrical conduction delay, seen as a wide QRS on EKG, qualify for cardiac resynchronization therapy (CRT). CRT literally resynchronizes the two sides of the heart to pump together, and it improves ejection fraction in 60 to 70 percent of appropriate candidates.
Four Pillars Of Congestive Heart Failure:
✅ ARNI, ARB, ACEI
✅ SGLT2i
✅ Beta Blocker
✅ MRA
Researchers and cardiologists now refer to four classes of medication as the "four pillars" of heart failure therapy. Each one works through a different biological pathway, and together, their benefits stack on top of one another:
-
ARNI (sacubitril/valsartan) — Relaxes blood vessels and helps the body clear excess fluid by enhancing the heart's own protective hormones.
-
Beta-blocker (e.g., carvedilol, metoprolol succinate, bisoprolol) — Slows the heart rate and reduces the strain on the heart muscle, giving it time to recover.
-
MRA (e.g., spironolactone, eplerenone) — Blocks a hormone called aldosterone that causes harmful scarring and fluid retention in the heart.
-
SGLT2 inhibitor (e.g., dapagliflozin, empagliflozin) — Originally developed for diabetes, these drugs were found to dramatically reduce heart failure hospitalizations and death, even in people without diabetes.
Quadruple therapy reduces mortality 61-73% over just two years. (https://www.jacc.org/doi/10.1016/j.jacc.2025.08.054)
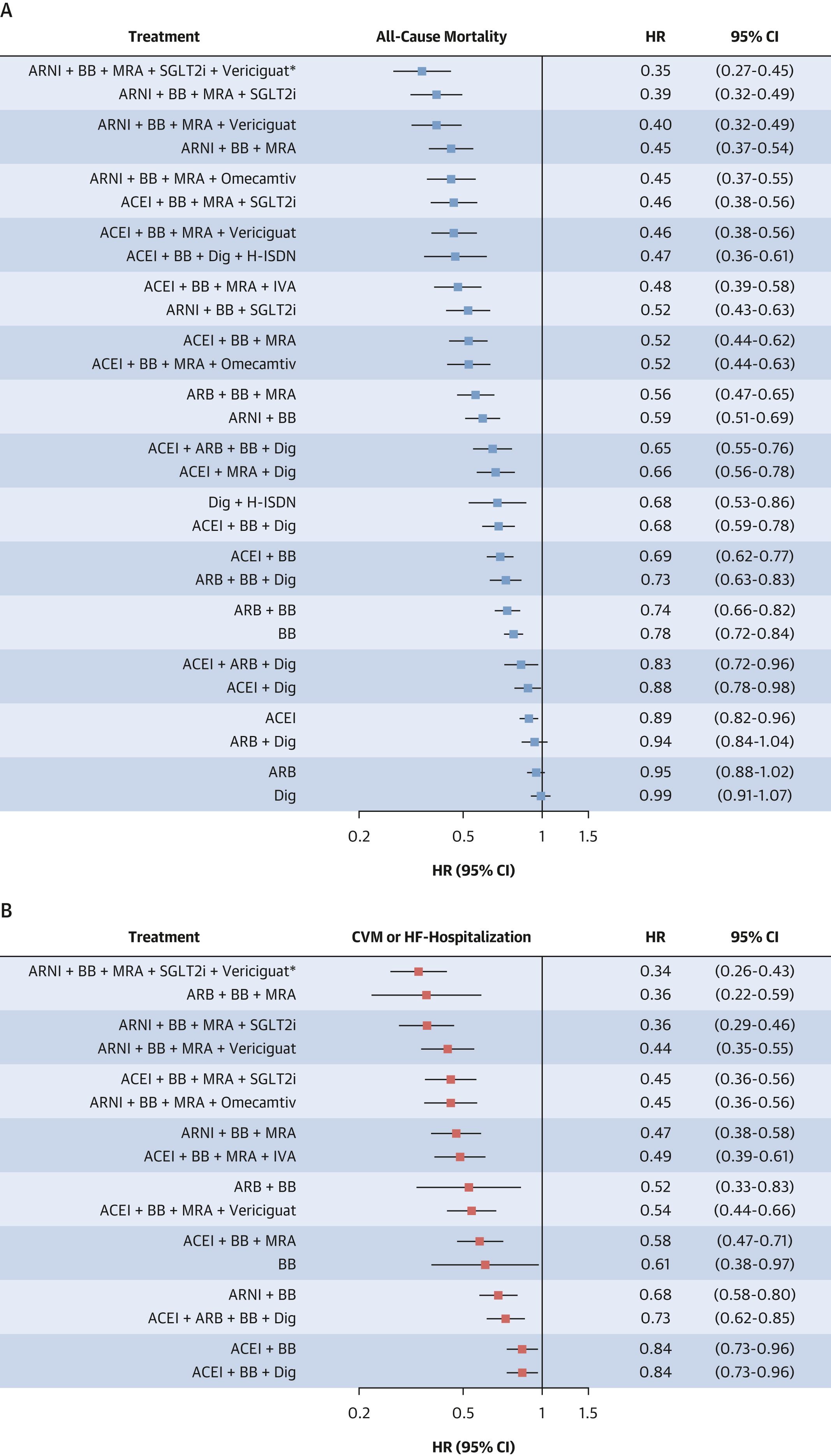
Forest plots summarizing the estimated HRs for all-cause mortality (A), cardiovascular mortality (B), and the composite of cardiovascular death or heart failure hospitalization (C) for all evaluated drug combinations in heart failure with reduced ejection fraction. Results are derived from the network meta-analysis, with placebo (PLBO) as the reference, and abbreviations are provided for each drug class. ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor/neprilysin inhibitor; BB = beta-blocker; Dig = digoxin; H-ISDN = hydralazine–isosorbide dinitrate; IVA = ivabradine; MRA = mineralocorticoid receptor antagonist; SGLT2 = sodium-glucose cotransporter 2 inhibitors. ∗The incremental benefit of quintuple therapy is exploratory and based on a single trial’s secondary endpoint.
The Evidence
- PARADIGM-HF Trial (sacubitril/valsartan): 20 percent reduction in cardiovascular death compared to enalapril alone in HFrEF patients. This was the trial that established the ARNI as the preferred renin-angiotensin blocker over ACE inhibitors.
- DAPA-HF Trial (dapagliflozin): 26 percent reduction in worsening heart failure or cardiovascular death in HFrEF. Benefit appeared within 28 days of starting the drug.
- EMPEROR-Reduced Trial (empagliflozin): 25 percent reduction in cardiovascular death and heart failure hospitalization in HFrEF. Effect was consistent regardless of diabetes status.
- EMPEROR-Preserved Trial (empagliflozin): 21 percent reduction in cardiovascular death and heart failure hospitalization in HFpEF. First major drug to show benefit in preserved ejection fraction heart failure.
- RALES Trial (spironolactone): 30 percent reduction in all-cause mortality in severe HFrEF. Established MRAs as a core pillar of therapy.
- MADIT-II Trial (ICD therapy): 31 percent reduction in all-cause mortality in post-myocardial infarction patients with ejection fraction at or below 30 percent treated with an ICD versus medical therapy alone.
- Combining all four pillars of GDMT reduces one-year mortality risk by an estimated 73 percent compared to no therapy, based on network meta-analysis data published in The Lancet in 2022.
What You Can Do
First, know your ejection fraction. If you have heart failure and cannot tell me your ejection fraction number, you do not have enough information to advocate for yourself. Ask your cardiologist directly. Get a copy of your echocardiogram report.
Second, ask your doctor whether you are on all four pillars of GDMT. If you have HFrEF and you are not on an ARNI, an MRA, and an SGLT2 inhibitor in addition to a beta-blocker, ask why. The answer may be legitimate, but you deserve an explanation.
Third, reduce your sodium intake to under 2,000 milligrams per day. Fluid retention worsens with high sodium. This is not a lifestyle preference. It is a medical necessity that reduces hospitalizations.
Fourth, weigh yourself every morning before eating, after using the bathroom. A weight gain of 2 to 3 pounds in 24 hours or 5 pounds in one week signals fluid accumulation. Call your care team before symptoms escalate. Early intervention prevents emergency department visits.
Fifth, exercise under supervision. Cardiac rehabilitation reduces heart failure hospitalizations by 25 percent. It is underutilized and underrefereed. Ask for a referral explicitly.
Sixth, if you have diabetes and heart failure, ask your cardiologist about SGLT2 inhibitors. If you have seen my content suggesting that GLP-1 receptor agonists like semaglutide benefit the heart, the evidence is real but nuanced. I address the full picture in my analysis of whether heart patients can take Ozempic, which is one of the most common questions I receive.
Data:
6.2 million: Number of Americans currently living with congestive heart failure, making it one of the most common cardiovascular diagnoses in the country.
73%: Estimated reduction in one-year mortality risk when all four pillars of GDMT are combined, compared to no pharmacological therapy.
21%: Reduction in cardiovascular death and heart failure hospitalization achieved by empagliflozin in HFpEF patients in the EMPEROR-Preserved Trial, marking the first proven therapy for preserved ejection fraction heart failure.
35%: The ejection fraction threshold below which patients qualify for ICD implantation to prevent sudden cardiac death, per current ACC/AHA guidelines.
25%: Reduction in heart failure hospitalizations associated with supervised cardiac rehabilitation programs, yet fewer than 1 in 5 eligible patients are ever referred.
2 to 3 lbs: The daily weight gain threshold that signals acute fluid retention in heart failure patients and requires immediate contact with a physician before symptoms worsen.
Infographic Summary:
Bottom Line
Congestive heart failure is a serious, progressive disease, but it responds to treatment in ways that most patients are never told. The best treatment for heart failure is not a single drug. It is a structured, evidence-based regimen built on four drug classes, reinforced by device therapy when appropriate, and supported by daily self-monitoring and supervised exercise. The myth that heart failure is simply managed and not reversed is outdated. Ejection fraction improves in a significant portion of patients who reach full GDMT doses. Hospitalizations drop. Quality of life returns. The evidence is not subtle, and the gap between what guidelines recommend and what most patients actually receive is the real crisis in heart failure care today. I want you to walk into your next cardiology appointment armed with one question: Am I on optimal guideline-directed medical therapy, and if not, what is standing in the way?
References
1. McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure (PARADIGM-HF). N Engl J Med. 2014;371(11):993-1004.
2. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction (DAPA-HF). N Engl J Med. 2019;381(21):1995-2008.
3. Berg DD, Jhund PS, Docherty KF, et al. Time to clinical benefit of dapagliflozin and significance of prior heart failure hospitalization in patients with heart failure with reduced ejection fraction. JAMA Cardiol. 2021;6(5):499-507.
4. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure (EMPEROR-Reduced). N Engl J Med. 2020;383(15):1413-1424.
5. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction (EMPEROR-Preserved). N Engl J Med. 2021;385(16):1451-1461.
6. Solomon SD, McMurray JJV, Claggett B, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction (DELIVER). N Engl J Med. 2022;387(12):1089-1098.
7. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure (RALES). N Engl J Med. 1999;341(10):709-717.
8. Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction (MADIT-II). N Engl J Med. 2002;346(12):877-883.
9. Cleland JGF, Daubert JC, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure (CARE-HF). N Engl J Med. 2005;352(15):1539-1549.
10. van Essen BJ, Ceelen DCH, Ouwerkerk W, et al. Pharmacologic treatment of heart failure with reduced ejection fraction: an updated systematic review and network meta-analysis. J Am Coll Cardiol. 2025;86(24):2513-2526.
11. Tromp J, Ouwerkerk W, van Veldhuisen DJ, et al. A systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. JACC Heart Fail. 2022;10(2):73-84.
12. Vaduganathan M, Claggett BL, Jhund PS, et al. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet. 2020;396(10244):121-128.
13. Greene SJ, Khan MS. Quadruple medical therapy for heart failure: medications working together to provide the best care. J Am Coll Cardiol. 2021;77(11):1408-1411.
14. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure. J Am Coll Cardiol. 2022;79(17):e263-e421.
15. American Heart Association. 2026 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation. 2026.
16. Molloy C, Long L, Mordi IR, et al. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev. 2024;3:CD003331.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine

















