

Reducing Triglycerides By 64% Did Not Reduce Plaque Volume
Mar 31, 2026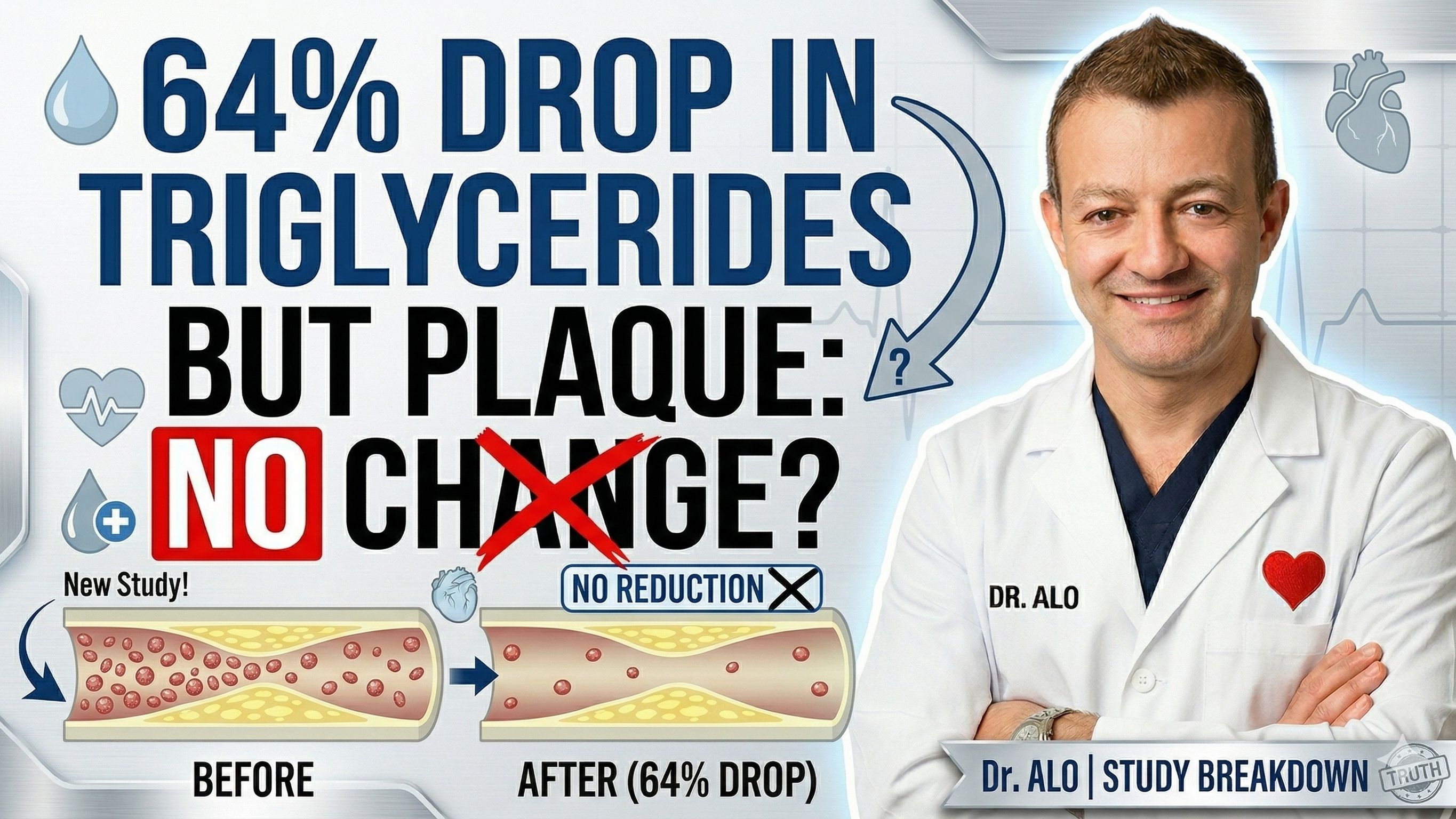
Reducing Triglycerides And Remnant Cholesterol By 70% Showed No Effect On Plaque
A brand-new trial just presented at ACC 2026 is turning heads in cardiology, and not necessarily for the reason you'd expect. Researchers gave patients a powerful new drug that cut their triglycerides by nearly two-thirds and slashed their remnant cholesterol by more than 70%. And yet, when they looked directly at the coronary arteries using CT imaging, the plaque didn't budge.
Zero difference compared to placebo.
This is a landmark result, and as your cardiologist, I want to break down exactly what it means for you.
Every day on social media, I am asked about lowering triglycerides and triglyceride ratios and why we don't treat triglycerides and why ratios don't matter. This is why. Lower triglycerides and remnant cholesterol by about 70% did not beat placebo, did not reduce plaque volume, and did not improve cardiovascular outcomes. Why? Because there was no concomitant reduction in LDL cholesterol.
Similar studies that showed a very steep reduction in LDL cholesterol, have shown plaque regression.
What Is Olezarsen, and Why Were People Excited About It?
Olezarsen is a new type of drug called an antisense oligonucleotide. It works by silencing a gene called APOC3, which normally puts the brakes on your body's ability to clear triglycerides from your blood.
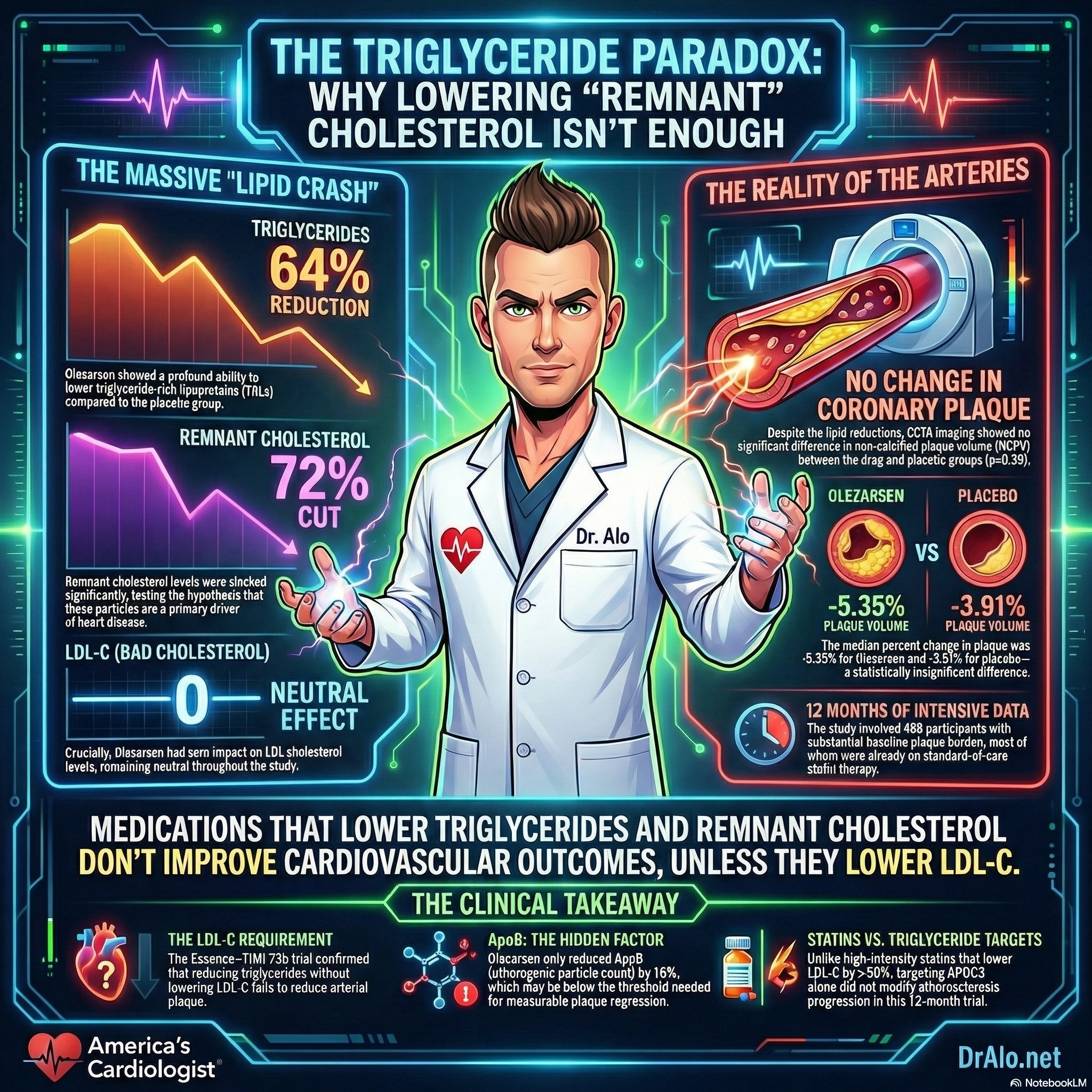
When you block APOC3, triglycerides fall dramatically. In the Essence-TIMI 73b trial, patients taking olezarsen saw their triglycerides drop by about 64% and their remnant cholesterol drop by nearly 72%, compared to placebo. Those are numbers that would make any cardiologist take notice.
The question the researchers wanted to answer: with that kind of triglyceride reduction, would coronary plaque shrink?
Infographic Summary:
How the Study Was Done
This was a rigorous, well-designed imaging substudy embedded in the larger Essence-TIMI 73b trial. Researchers enrolled 468 patients who had elevated triglycerides (at least 150 mg/dL, with a median around 249 mg/dL) and existing coronary plaque visible on a specialized heart CT scan called a coronary CT angiography (CCTA).
These were real-world patients: 97% of them were already on lipid-lowering therapy, including nearly 79% on a statin. The drug or placebo was given for 12 months, and then the CT scan was repeated to measure whether the plaque volume had changed.
The primary target was noncalcified plaque volume (NCPV), the portion of plaque that is most dangerous and most likely to cause a heart attack.
The Results: Triglycerides Down, Plaque Unchanged
Here is what the researchers found after 12 months:
Triglycerides: Down 64% compared to placebo.
Remnant cholesterol: Down nearly 72% compared to placebo.
VLDL cholesterol: Down about 61% compared to placebo.
LDL cholesterol: No change. Essentially identical between the olezarsen and placebo groups.
ApoB: Down about 16% compared to placebo.
And the plaque? The noncalcified plaque volume did not change between groups (p=0.36). Low-attenuation plaque, the most dangerous lipid-rich vulnerable type, also showed no difference. Neither did calcified plaque, fibrous plaque, or total plaque. Across every measure, olezarsen performed identically to placebo.
Here Is the Critical Point: LDL and ApoB Are What Drive Plaque
This study puts a very clear stake in the ground. Triglycerides fell dramatically, but LDL cholesterol did not move at all. And the plaque didn't change.
Compare that to what we see with statins and PCSK9 inhibitors. Those drugs lower LDL by 50% or more and reduce ApoB, the true count of all atherogenic particles in your blood, by 40 to 60%. In trials like GLAGOV, SATURN, PACMAN-AMI, and PRECISE-IVUS, those therapies produced measurable and meaningful plaque regression. Mainly because they drove LDL cholesterol to very low levels.
Olezarsen did lower ApoB, but only by about 16%. The researchers themselves point out that this modest reduction may simply be too small to produce a measurable change in plaque over 12 months. The drug reduces triglycerides primarily by clearing VLDL particles, but because VLDL gets converted to LDL, LDL levels don't fall. So while you're reducing one type of atherogenic particle, you're not touching the most damaging one (LDL).
The bottom line: to regress coronary plaque, you have to drive down LDL and ApoB. Triglyceride lowering alone, even massive triglyceride lowering, does not appear to be sufficient.
Does This Mean Triglycerides Don't Matter?
Not exactly. This study doesn't prove triglycerides are harmless. It proves that lowering triglycerides without also lowering LDL and ApoB doesn't move plaque.
High triglycerides, particularly when combined with elevated remnant cholesterol, are associated with higher cardiovascular risk in observational studies. People with loss-of-function mutations in the APOC3 gene naturally have lower triglycerides and lower lifetime risk of coronary artery disease. That genetic data is real and compelling.
But association is not the same as causation. And this imaging trial gives us a 12-month, randomized, placebo-controlled answer: drug-mediated triglyceride lowering without a corresponding reduction in LDL did not change the plaque.
The researchers acknowledged that a longer study, or combining olezarsen with a PCSK9 inhibitor to also suppress LDL, could tell a different story. That combination is worth studying.
What This Means for You as a Patient
If you have high triglycerides and your doctor is talking to you about treatment, the most important question to ask is: what is happening to my LDL and my ApoB?
High triglycerides are often a signal that your overall lipid metabolism is out of balance. Many people with elevated triglycerides also have elevated ApoB and small, dense LDL particles that don't always show up on a standard LDL test. That's exactly why I prioritize ApoB testing in my practice.
The therapies with the strongest evidence for reducing plaque and reducing heart attacks remain: high-intensity statins, PCSK9 inhibitors, and ezetimibe. These drugs work because they directly lower LDL cholesterol and, critically, they lower ApoB. That is what drives plaque regression.
Lowering your triglycerides through lifestyle, meaning less alcohol, less refined carbohydrate, more exercise, and weight loss, is still worthwhile and important. But if your goal is to shrink the plaque in your coronary arteries, the evidence keeps pointing to one thing: get LDL and ApoB as low as possible.
I go through the proper way to treat triglycerides in a way that actually reduces cardiovascular risk.
Triglyceride Bottom Line
The Essence-TIMI 73b imaging study is the first randomized trial to test whether aggressive triglyceride lowering can change coronary plaque. The answer, for now, is no. Despite a 64% reduction in triglycerides and a 72% reduction in remnant cholesterol, olezarsen produced no measurable change in plaque volume compared to placebo over 12 months.
This does not mean the drug has no future, and it does not mean triglycerides are irrelevant. It does mean that reducing triglycerides is not the same as reducing plaque, and it is not a substitute for lowering LDL and ApoB.
The science of lipid management continues to evolve, and this trial is an important piece of that story. As always, I'll keep bringing you the evidence as it develops.
References:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.126.080012
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















