

Lowering Triglycerides Correctly Can Improve Cardiovascular Outcomes
Mar 29, 2026
The Triglyceride Paradox: Why Lowering Triglycerides Hasn't Reduced Heart Disease
Most people get this wrong.
There are many ways to lower triglycerides, but most of them do not improve cardiovascular outcomes. However, there are a few things we can do to improve cardiovascular outcomes. We are going to dive deep into what works and what does not work.
For decades, elevated triglycerides have been thought to be a cardiovascular risk factor. It seemed logical: lower triglycerides, reduce heart attacks and strokes. But when researchers put this hypothesis to the test in large clinical trials, the results were surprisingly disappointing.
Multiple studies have now demonstrated that lowering triglycerides with medications like fibrates, niacin, fish oil, EPA, or other omega-3 fatty acids, does not reliably reduce cardiovascular events. In some cases, it even caused harm.
However, lowering triglycerides via lifestyle changes; weight loss, exercise, quitting alcohol, reversing or treating diabetes optimally, and other interventions, significantly improves cardiovascular outcomes. But the cardiovascular outcomes improve not because you lowered triglycerides, but because you started running, lifting weight, cut calories, and stopped drinking alcohol. But it's a lot more complicated than that.
The biggest effect on lower triglycerides appears to be weight loss, via any form of calorie restriction.
We also have modern therapeutics (and old ones) that help lower triglycerides extensively. Medications that directly lowered triglycerides did not affect cardiovascular outcomes, while those that caused weight loss, made a huge difference.
Let's take a look at the studies and data.
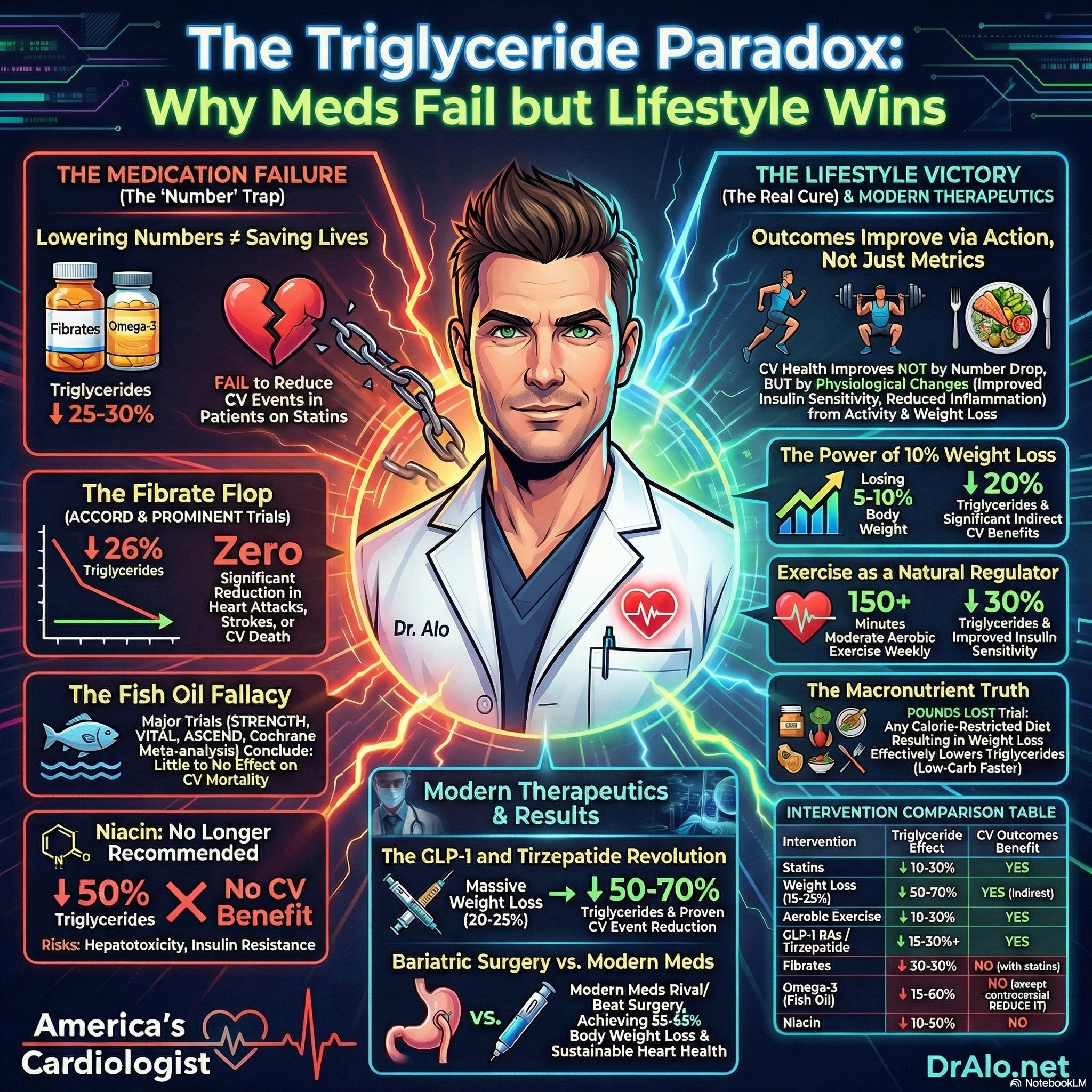
Infographic Summary Of Triglyceride Lowering Treatments And Outcomes:
First, let's discuss medications that were traditionally designed to treat triglycerides, and why they don't work.
The Fibrate Failures
Fibrates were once considered promising drugs for cardiovascular risk reduction. In the pre-statin era, trials like the Helsinki Heart Study and VA-HIT showed that fibrates could reduce cardiovascular events when used as monotherapy. But the landscape changed dramatically once statins became standard therapy.
The ACCORD-Lipid trial tested whether adding fenofibrate to statin therapy would benefit patients with type 2 diabetes. Despite enrolling 5,518 patients and achieving a 25.6% reduction in triglycerides over 5 years, there was no significant reduction in the primary outcome of nonfatal MI, nonfatal stroke, or cardiovascular death (HR 0.92, 95% CI 0.79-1.08).
Similarly, the FIELD study in 9,795 participants with diabetes showed no significant benefit for coronary events despite a 29% triglyceride reduction.
The most recent and perhaps most definitive fibrate trial was PROMINENT, which tested pemafibrate, a selective PPAR-α modulator designed to maximize triglyceride lowering while minimizing side effects.
In 10,497 patients with diabetes and elevated triglycerides on statin therapy, pemafibrate achieved impressive biochemical results: a 26.2% reduction in triglycerides and 25.6% reduction in remnant cholesterol. Yet there was absolutely no reduction in cardiovascular events (HR 1.03, 95% CI 0.91-1.15).
What went wrong? The answer may lie in what else pemafibrate did: it increased LDL-C by 12.3% and apolipoprotein B by 4.8%. This translated to roughly a 10 mg/dL reduction in remnant cholesterol offset by a 10 mg/dL increase in LDL-C, meaning pemafibrate didn't actually reduce the total mass of proatherogenic apoB-containing particles.
As a side note, today we only recommend usage of fenofibrate due to it's safety profile.
Omega-3 Fatty Acids: A Similar Story (Fish Oil, EPA)
The omega-3 fatty acid (fish oils) trials have largely mirrored the fibrate experience.
The STRENGTH trial randomized 13,078 high-risk patients to 4 g/day of omega-3 carboxylic acids (EPA + DHA) versus corn oil placebo. The trial was terminated early for futility after a median follow-up of 42 months showed no difference in cardiovascular events: 12.0% in the omega-3 group versus 12.2% in placebo (HR 0.99, 95% CI 0.90-1.09).
Other trials told the same story.
The VITAL trial studied low-dose omega-3 fatty acids in primary prevention and found no significant reduction in major cardiovascular events.
The ASCEND trial in diabetic patients similarly showed no benefit.
A comprehensive Cochrane meta-analysis of 86 trials involving 162,796 participants concluded that increasing omega-3 intake resulted in little or no effect on all-cause mortality, cardiovascular mortality, or cardiovascular events.
See my long article, in depth article on Fish Oil Trials.
The REDUCE-IT Exception, Or Is It?
The one glaring exception to this pattern is the REDUCE-IT trial, which showed a dramatic 25% reduction in cardiovascular events with high-dose icosapent ethyl (purified EPA 4 g/day) versus placebo (HR 0.75, 95% CI 0.68-0.83).
This positive result led to FDA approval of icosapent ethyl for cardiovascular risk reduction.
But there's a catch, and it's a big one. REDUCE-IT used mineral oil as the placebo, and many experts believe this choice fundamentally compromised the trial's validity.
The Mineral Oil Controversy
In REDUCE-IT, the mineral oil placebo group experienced concerning changes that weren't seen in other omega-3 trials using different placebos.
High-sensitivity C-reactive protein (hs-CRP), a marker of inflammation, increased from a median of 2.1 to 2.8 mg/L in the mineral oil group, while it actually decreased from 2.2 to 1.8 mg/L in the icosapent ethyl group. LDL cholesterol also increased by 10.2% in the mineral oil placebo arm versus only 3.1% in the treatment group.
These changes raised a critical question: Did icosapent ethyl reduce cardiovascular events, or did mineral oil increase them?
The STRENGTH trial, which used corn oil as placebo instead of mineral oil, provides compelling evidence for the latter interpretation.
STRENGTH found no cardiovascular benefit with omega-3 fatty acids, and notably, the corn oil placebo did not cause the increases in LDL-C and hs-CRP seen with mineral oil in REDUCE-IT.
Perhaps most damning is a secondary analysis from STRENGTH showing that even when patients achieved EPA levels comparable to those in REDUCE-IT, there was no cardiovascular benefit.
This suggests the benefit in REDUCE-IT wasn't due to EPA itself, but rather to harm from the mineral oil placebo.
Defending REDUCE-IT
The REDUCE-IT investigators have pushed back against this criticism. They note that an FDA exploratory analysis concluded that the changes in LDL-C and hs-CRP alone could not account for the positive cardiovascular outcomes.
They also point out that the placebo group event rate in REDUCE-IT (5.74% annually) was exactly as projected during the trial design phase and consistent with other cardiovascular outcome studies in similar high-risk populations.
Additionally, a study comparing mineral oil versus non-mineral oil placebo on coronary plaque progression using CT angiography found no significant differences. A review found no consistent pattern of harmful changes with mineral oil, and when changes occurred, they were generally small and not clearly clinically significant.
The 2021 ACC Expert Consensus acknowledges the controversy but concludes: "Although some of the observed benefits seen in REDUCE-IT could be attributed to the increase in LDL-C and hs-CRP associated with the mineral oil placebo, it is unlikely to explain the large relative risk (25%) and absolute risk reduction (4.8%) seen in REDUCE-IT."
In the newly published European and American Cholesterol Treatment Guidelines, they do not recommend fish oil supplementation. They recommend using prescription EPA in very rare cases and it's a 2b recommendation, meaning the evidence is very weak. In prior guidelines, it was a class 3 recommendation, meaning you should not use it at all.
Luckily, it's 2026 and we have far better ways of treating triglycerides in ways that actually reduce cardiovascular outcomes, that are not controversial.
ESSENCE-TIMI 73B Trial
The provided text describes the Essence–TIMI 73b imaging study, a clinical trial investigating how the drug olezarsen affects coronary plaque progression. Researchers used computed tomography angiography to monitor heart artery health in patients with elevated triglycerides who were already receiving standard treatments.
While the medication successfully triggered massive reductions in triglycerides (64%) and remnant cholesterol (70%), it notably failed to change the volume of noncalcified coronary plaque over the twelve-month period. The study authors suggest that these results may be due to the drug’s relatively modest effect on LDL-C and apolipoprotein B, which measures the total count of harmful particles.
Despite the 70% reduction in triglycerides, there was no reduction plaque volume, because LDL cholesterol did not change.
Consequently, the findings indicate that simply lowering triglycerides may not be enough to reverse or slow atherosclerosis within a one-year timeframe. Future long-term trials are necessary to determine if this therapy ultimately provides any measurable cardiovascular protection for patients.
Read the details of the ESSENCE 73B Trial
What Does It All Mean?
The weight of evidence suggests that triglyceride lowering via medications does not reliably reduce cardiovascular risk. Whether fibrates or omega-3 fatty acids, the story is remarkably consistent: triglycerides go down, but cardiovascular events don't.
The REDUCE-IT trial remains an outlier, and the mineral oil placebo controversy casts significant doubt on whether its results represent a true treatment effect. Until we have another trial of purified EPA using an inert placebo, the question will remain unresolved.
For now, clinicians should recognize that elevated triglycerides may be a marker of residual cardiovascular risk rather than a modifiable target. The focus should remain on proven therapies: statins for LDL lowering, blood pressure control, diabetes management, and lifestyle modification.
The triglyceride hypothesis, while biologically plausible, has not been validated by the clinical trial evidence.
With that said...
What If We Reduce Triglycerides With Weight Loss And Lifestyle Changes: A New Frontier In Triglyceride Treatment
What happens if we treat hypertriglyceridemia with lifestyle interventions?
What if we lose weight? Change our diets? Quit drinking? Address underlying kidney disease? Treat diabetes correctly?
Triglyceride History Lesson
Elevated triglycerides affect approximately one-third to one-fourth of the U.S. population and represent a significant contributor to cardiovascular disease risk. Not because the triglycerides are intrinsically atherogenic (they may be), but because they can give us clues to underlying disease and metabolic derangements.
While LDL cholesterol has long been the primary target of lipid-lowering therapy, we now understand that triglyceride-rich lipoproteins and their remnants are independently atherogenic and contribute to residual cardiovascular risk even in patients with well-controlled LDL cholesterol on statin therapy. This is why we recommend measuring apoB, it captures all atherogenic particles (95% of which are LDL particles).
Let's explore triglyceride-lowering strategies, from lifestyle modifications that can reduce triglycerides by up to 70%, to the latest pharmacological therapies with proven cardiovascular outcomes benefits.
Part 1:The Power of Weight Loss
Weight loss is considered the most effective lifestyle intervention for lowering triglyceride levels. The relationship between weight loss and triglyceride reduction follows a clear dose-response pattern: the more weight lost, the greater the triglyceride reduction. We now have very effective ways to reduce body weight!
The Numbers Behind Weight Loss
According to the 2021 ACC Expert Consensus Decision Pathway and the 2026 ACC/AHA Dyslipidemia Guidelines:
- A 5-10% reduction in body weight is associated with approximately a 20% decrease in triglycerides
- Per 1 kg of weight lost, triglycerides decrease by approximately 4 mg/dL with lifestyle interventions
- Triglycerides may be lowered by 50-70% in highly responsive individuals
- With rapid weight loss (1 kg per week), triglycerides can decrease by 30-40%
What About Losing 25% of Body Weight?
With the advent of highly effective GLP-1 receptor agonists and dual GIP/GLP-1 agonists like tirzepatide, weight losses of 20-25% are now achievable. Based on the dose-response relationship, a person weighing 100 kg (220 lbs) who loses 25 kg (55 lbs) could expect:
- Using the 4 mg/dL per kg estimate: approximately 100 mg/dL reduction in triglycerides
- Using the percentage-based estimates: potentially 50-70% reduction in triglycerides
The Look AHEAD study demonstrated that proportional to the amount of weight reduction across categorical ranges (≥2% to 5%, ≥5% to 10%, ≥10% to 15%, and ≥15%), blood triglyceride levels were progressively and significantly reduced by more than 60 mg/dL in those achieving the greatest weight loss.
Bariatric Surgery: The Ultimate Weight Loss Intervention
For patients with severe obesity, bariatric surgery produces dramatic and sustained improvements in triglyceride levels:
- Roux-en-Y gastric bypass (RYGB): Triglycerides reduced by approximately 61 mg/dL at 5+ years post-surgery, with prevalence of high triglycerides dropping from 23.7% to 4.9% at 7 years
- Sleeve gastrectomy: Triglycerides decreased by 29% at 5 years
- Adjustable gastric banding: More modest improvements, with high triglyceride prevalence dropping from 21.3% to 9.7% at 7 years
The Swedish Obese Subjects (SOS) study demonstrated that recovery from hypertriglyceridemia was approximately three-fold higher in the surgery group compared to conventional treatment at both 2 and 10 years.
Part 2: Dietary Approaches To Lowering Triglycerides
Which types of diets lower triglycerides more? Does it matter if you reduce carbohydrates or fats or proteins? What type of diet should we recommend?
Low-Carbohydrate Diets
Higher-fat, lower-carbohydrate diets are usually associated with greater triglyceride reduction compared to lower-fat, higher-carbohydrate diets. The evidence shows:
- Very low-carbohydrate diets (10% of calories from carbohydrates): −24 mg/dL reduction
- Low-carbohydrate diets (20% energy from carbs): 18% triglyceride reduction
- Lower-fat diets: No significant effect on triglycerides despite weight loss
High-Protein Diets
A higher-protein diet (31% of energy from protein) versus standard-protein (18% of energy) produces:
- Greater weight loss (−0.79 kg difference)
- Greater triglyceride lowering (−20 mg/dL)
In one study of individuals with metabolic syndrome, those on a high-protein diet had a 35% reduction in triglycerides versus a nonsignificant 5% reduction in the conventional diet group.
Intermittent Fasting
Intermittent fasting regimens produce triglyceride reductions of 16-42%, with the greatest decreases associated with the greatest weight loss. Alternate-day fasting (0.75 kg/week weight loss) produces greater benefits than periodic fasting (0.25 kg/week).
Does The Macronutrient Breakdown Of The Diet Really Matter?
Does the macronutrient composition of the diet matter as long as it causes weight loss? Does it matter if it is low carbohydrate or high protein, so long as you lose weight? Probably not. All that matters is that you actually lose weight and calorie restrict.
POUNDS LOST Trial (2010)
This landmark study evaluated 4 weight loss diets with varying macronutrient compositions (fat: 20% vs 40%; protein: 15% vs 25%; carbohydrate: 35-65%). After 2 years, weight loss was similar across all groups, and all diets decreased triglycerides similarly by 12% to 17%, irrespective of macronutrient composition. This supports the concept that triglyceride reduction is primarily weight-dependent.
If you really want to lower triglycerides, find a calorie restricted diet that you can actually stick to for a long time. That's the most important thing. The problem with higher fat, keto, and carnivore style diets is that you can raise LDL cholesterol significantly and worsen heart disease outcomes. The weight loss, in and of itself, does lower triglycerides.
We don't want to lower triglycerides while also raising LDL cholesterol. Especially, since there is no proven benefit to lowering triglycerides in isolation. If you are only focusing on lowering triglycerides for the sake of lowering triglycerides, you are missing the forest for the trees. There is no reason to lower triglycerides in isolation.
Part 3: Exercise and Physical Activity To Lower Triglycerides
Moderate-intensity aerobic exercise (≥150 minutes per week) reduces triglycerides by approximately 18.6 mg/dL (up to 30%). The benefits come from:
- Improved insulin sensitivity
- Maintenance of healthy weight
- Direct effects on triglyceride clearance through increased lipoprotein lipase activity
Part 4: Alcohol Consumption And Triglycerides
Alcohol restriction or elimination is recommended for all patients with elevated triglycerides. For those with triglycerides ≥500 mg/dL, complete abstinence is required to prevent acute pancreatitis.
Part 5: Pharmacological Therapies To Lower Triglycerides
When lifestyle modifications are insufficient, several medication classes can effectively lower triglycerides. However, it's crucial to understand that triglyceride lowering does not automatically translate to cardiovascular benefit.
Statins: The Foundation
While not primarily triglyceride-lowering agents, statins reduce triglycerides by 10-30% in a dose-dependent manner. More importantly, statins remain first-line therapy for ASCVD risk reduction in patients with hypertriglyceridemia due to their proven cardiovascular outcomes benefits.
Fibrates: Potent Triglyceride Lowering With No Improvement In Outcomes
Fibrates (fenofibrate, gemfibrozil) reduce triglycerides by 30-50% through:
- Stimulation of PPAR-alpha
- Activation of lipoprotein lipase
- Reduction of apolipoprotein C-III production
However, cardiovascular outcomes trials show no reduction in cardiovascular events when fenofibrate is added to statin therapy. Fibrates remain first-line for severe hypertriglyceridemia (≥500 mg/dL) to prevent pancreatitis.
Important safety note: Gemfibrozil should never be combined with statin therapy due to serious drug interactions. It's an older medication that should not be used in today's modern world. It also worsens the likelihood of having muscle aches from statins when combined with statins.
Fenofibrate is the safer option when combination therapy is needed.
Icosapent Ethyl (EPA): Questionable Outcomes (VASCEPA)
See the prior discussion, while this is approved for triglyceride lowering, it does not appear to confer benefit. There are much more effective medications and interventions in today's modern world.
Important: Over-the-counter fish oil supplements are NOT equivalent to prescription icosapent ethyl and have variable EPA/DHA content.
Omega-3 Acid Ethyl Esters (EPA + DHA) Lovaza, Omacor: Not Recommended
These products reduce triglycerides by 15-61% but can modestly raise LDL-C (though not apoB). Unlike icosapent ethyl, mixed EPA/DHA products have not demonstrated cardiovascular outcomes benefits in trials like STRENGTH.
Niacin: Should Never Be Used
Niacin reduces triglycerides by 10-50% (depending on formulation) but is considered a last-line agent due to:
- Poor tolerability (flushing, GI side effects)
- Increased insulin resistance
- Hepatotoxicity risk
- Makes HDL particles more atherogenic
- Inflammatory metabolites
No cardiovascular benefit when added to statin therapy
Ezetimibe
While primarily an LDL-C lowering agent (18-22% reduction), ezetimibe provides modest triglyceride lowering of 5-8%. It has proven cardiovascular benefit when added to statins (IMPROVE-IT trial).
Part 6: Diabetes Medications with Lipid Effects
Several diabetes medications have favorable effects on triglycerides, making them attractive options for patients with both diabetes and dyslipidemia.
GLP-1 Receptor Agonists
GLP-1 RAs demonstrate the most comprehensive lipid-lowering profile among diabetes medications:
- Triglyceride reduction: 15-30%
- LDL-C reduction: 3-5 mg/dL
- Mechanisms: Reduced postprandial chylomicron production, increased insulin, reduced glucagon, inhibition of adipose tissue lipolysis
- Effects likely due to calorie restriction
Liraglutide specifically has been shown to reduce fasting triglycerides by approximately 30% through increased catabolism of VLDL and LDL particles. This is one mechanism that needs to be explored further. Clinically, we have seen significant reductions in triglycerides in patients on various GLP1 RAs.
Tirzepatide (GIP/GLP-1 Dual Agonist)
Tirzepatide shows even greater lipid improvements than GLP-1 RAs alone:
- Superior reductions in triglycerides and VLDL cholesterol compared to semaglutide
- Greater increases in HDL cholesterol
- These effects are proportional to the substantial weight loss achieved (up to 20-25%)
- Effects likely due to significant calorie restriction
In head-to-head comparison, tirzepatide 15 mg was associated with statistically significant greater improvements in triglycerides compared to semaglutide 2.4 mg.
We will need more studies on these medications. As it stands now, they do have potent triglyceride lowering effects.
SGLT2 Inhibitors
SGLT2 inhibitors have a mixed lipid profile:
- Triglyceride reduction: approximately 9 mg/dL
- LDL-C increase: 3-4 mg/dL (paradoxical)
- HDL-C increase: 2-3 mg/dL
The mechanism involves increased lipoprotein lipase activity (lowering triglycerides) but decreased LDL clearance. Despite the small LDL increase, SGLT2 inhibitors provide substantial cardiovascular and renal benefits through other mechanisms.
Other mechanisms may be due to calorie dumping. They cause urination of excess glucose and "calorie dumping". Diabetic patients on these can see appreciable weight loss. Similar to how metformin causes calorie dumping via fecal excretion.
Metformin
Metformin has modest triglyceride-lowering effects:
- Approximately 8-10% reduction in diabetic patients
- Mechanism: Increased VLDL-triglyceride clearance by brown adipose tissue
- Fecal excess calorie (glucose) excretion
Part 7: Weight Loss Medications Effects On Triglyceride Lowering
In clinical practice, we can sometimes achieve a 70-95% triglyceride lowering by combing weight loss medications with lifestyle changes.
Weight loss medications may include:
- Phentermine, Diethylpropion
- Wellbutrin
- Naltrexone
- Topiramate
- GLP1 RAs
- SGLT2i
- Metformin
The mechanism by which these medications lower triglycerides is due to massive amounts of weight loss. We are now able to beat gastric bypass surgery in terms of percentage of body weight lost. Gastric bypass has traditionally been able to cause a 35-40% body weight loss. With these newer medications and therapeutics, we are seeing 55-65% body weight losses, and they are maintaining the weight loss. Most bariatric surgery patients gain much of the weight back.
Using anti-obesity medications and newer weight loss strategies has caused a significant amount of weight loss, with concomitant severe reductions in triglycerides. There will likely be new guideline updates in the future to mirror these results.
We have already seen a 20-26% reduction in cardiovascular event rates with semaglutide, regardless of starting BMI in the Wegovy studies. See other articles on this blog.
Part 8: Comprehensive Triglyceride Medication Lowering Comparison Table
The following table summarizes the effects of all major triglyceride-lowering interventions:
| Intervention | Triglyceride Effect | LDL-C Effect | HDL-C Effect | CV Outcomes Benefit |
|---|---|---|---|---|
| Weight loss (5-10%) | ↓ 20% | ↓ Modest | ↑ Modest | Yes (indirect) |
| Weight loss (15-25%) | ↓ 50-70% | ↓ Modest | ↑ 4-5 mg/dL | Yes (indirect) |
| Bariatric surgery (RYGB) | ↓ 40-61 mg/dL | ↓ 18-25 mg/dL | ↑ 14 mg/dL | Yes (observational) |
| Low-carb diet | ↓ 18-24% | Variable | ↑ | Yes (indirect) |
| Aerobic exercise | ↓ 18.6 mg/dL (up to 30%) | Neutral | ↑ | Yes |
| Statins | ↓ 10-30% | ↓ 30-55% | ↑ 1-2 mg/dL | Yes (primary therapy) |
| Ezetimibe | ↓ 5-8% | ↓ 18-22% | ↑ 3% | Yes (added to statin) |
| Fenofibrate | ↓ 30-50% | ↓ 20-31% | ↑ 10-15% | No (when added to statin) |
| Icosapent ethyl (EPA) | ↓ 20-33% | Neutral | ↓ 4-6% | Yes (REDUCE-IT) |
| Niacin | ↓ 10-50% | ↓ 15-25% | ↑ 15-35% | No (when added to statin) |
| GLP-1 RAs | ↓ 15-30% | ↓ 3-5 mg/dL | Neutral to ↑ | Yes (CVOTs) |
| Tirzepatide | ↓ Greater than GLP-1 RAs | ↓ Modest | ↑ Greater than GLP-1 RAs | Yes (SELECT) |
| SGLT2 inhibitors | ↓ 9 mg/dL | ↑ 3-4 mg/dL | ↑ 2-3 mg/dL | Yes (HF/renal) |
| Metformin | ↓ 8-10% | ↓ 5-9 mg/dL | ↑ 1-2 mg/dL | Uncertain |
Part 9: Putting It All Together - A Practical Approach To Lowering Triglycerides
For Severe Hypertriglyceridemia (≥500 mg/dL)
The primary goal is preventing acute pancreatitis:
1. Immediate lifestyle intervention (very low-fat diet, alcohol abstinence, weight loss)
2. First-line pharmacotherapy: Statin medications
3. Add metformin, anti-obesity medications (need to cause significant weight loss)
4. Intensify diabetes or pre-diabetes treatment
5. After significant weight loss, can add fenofibrate if triglycerides still high
6. Last resort can add prescription EPA (not fish oil or omega 3 supplements)
For Moderate Hypertriglyceridemia (150-499 mg/dL)
The primary goal is ASCVD risk reduction:
1. Lifestyle optimization (weight loss, low-carb diet, exercise, alcohol moderation)
2. First-line: Statin therapy (higher intensity for greater triglyceride lowering) can add ezetemibe to get further lipid lowering
3. If triglycerides remain elevated on maximally tolerated statin and ezetemibe AND patient has established ASCVD or diabetes with additional risk factors: Add metformin or intensify diabetes treatments with SGLT2i, GLP1s, etc
4. Add anti-obesity, weight loss medications
5. Consider GLP-1 RA or tirzepatide for patients with obesity and/or diabetes
6. Intensify diabetes or pre-diabetes treatment
7. After significant weight loss, can add fenofibrate if triglycerides still high
8. Last resort can add prescription EPA (not fish oil or omega 3 supplements)
Triglycerides And The Insulin Resistance And Diabetes Connection
In clinical practice, the number one cause of high triglycerides is undiagnosed or poorly controlled diabetes. Please note, that this may not always be the case, but you must test this pathway first.
Don't misunderstand. Pathophysiologically, the patient must have some underlying predisposition to hypertriglyceridemia in order to have elevated triglycerides from undiagnosed insulin resistance or uncontrolled diabetes. But hypertriglyceridemia does not occur to this extent, just because you have slightly uncontrolled diabetes. Plenty of people have severely elevated triglycerides, but very well controlled diabetes.
But if you have elevated triglycerides, and your diabetes is not well controlled, then the priority must be to get the diabetes under better control first and then reassess to see if you have a triglyceride problem.
Without these underlying hypertriglyceridemia genetics, you aren't going to see triglycerides in the 500+ mg/dL range. But this can also occur at triglyceride level, including below 500 mg/dL.
Clinical Approaches To Hypertriglyceridemia
The first step is to assess the patient's weight and BMI. Are they overweight? What's their diet like. If they are serious about weight loss and lifestyle, recommend a calorie restricted Mediterranean style diet. Using a tracking app to track calories is very helpful. If they are unsuccessful, or find it hard to lose weight, you can offer them anti-obesity medications. Start with metformin as a cornerstone since it also treats underlying insulin resistance (if it exists). We don't always know if it exists.
The next thing you should do when you see elevated triglycerides, is to look at fasting glucose, A1c, medication lists, family history of diabetes, and any other markers or patterns that may indicate some form of impaired fasting glucose, pre-diabetes, diabetes, or poorly controlled diabetes.
In many cases, another clinician has taken them off the metformin or deintensified treatment. You need ask why they were on it or why the medication was stopped.
In some cases, another clinician is not a diabetes expert and thinks that metformin may cause hypoglycemia or renal failure. It does neither of these.
In some cases, the other clinician thinks you need to stop metformin to start and SGLT2i or GLP1. This is also incorrect. See my updated diabetes treatment guidelines article.
In some cases they add fenofibrate before they add metformin, thinking it is primarily a triglyceride problem, when in fact, it is a insulin resistance problem.
The first step is to make sure the patient is on statin therapy, regardless of starting LDL cholesterol level. They are usually high risk, and you probably want their LDL cholesterol below 70 mg/dL at the least. If they have had heart disease previously, you can aim lower, like 55 mg/dL or perhaps lower. See the updated Cholesterol Treatment Guidelines. This will cause an initial reduction in triglycerides as well.
If their A1c is not quite "pre-diabetes range", and has been slowly increasing over the years, you can start metformin. Even a small dose like 500 mg once or twice a day usually is enough. This is better than starting a more expensive option and metformin has better results. This is preferred to fenofibrate in most cases.
In many cases, this may be enough to solve the triglyceride problem.
If their triglycerides are quite high, you may need to add more medications.
If they are overweight, you can add anti-obesity medications. If they are diabetic, you can intensify diabetes treatment. Most modern diabetes medications do not cause hypoglycemia.
This is an overly simplified approach to hypertriglyceridemia. But this should work for 90-95% of cases. If you have questions, join my community to get more personalized advice.
Triglyceride Key Takeaways
1. Weight loss is the most powerful lifestyle intervention for triglyceride lowering, with potential reductions of 50-70% in highly responsive individuals.
2. Diet composition sometimes matters: Low-carbohydrate, high-protein diets produce greater triglyceride reductions than low-fat diets in the short term. Although, any calorie restricted diet achieves the same results long term. Focus on long term sustainability with a heart healthy diet.
3. Statins remain first-line for ASCVD risk reduction in patients with hypertriglyceridemia, despite being less potent triglyceride-lowering agents than fibrates.
4. Icosapent ethyl may be used in rare cases, but has questionable cardiovascular outcomes.
5. Fibrates do not reduce cardiovascular events when added to statin therapy and should be reserved for severe hypertriglyceridemia to prevent pancreatitis.
6. GLP-1 RAs and tirzepatide offer attractive options for patients with obesity and/or diabetes, providing weight loss, glycemic control, and favorable lipid effects including triglyceride lowering.
7. Over-the-counter fish oil supplements are not equivalent to prescription omega-3 fatty acids and should not be used as substitutes.
8. Niacin should never be used due to worse outcomes.
Video Explanation Of How To Lower Triglycerides To Improve Cardiovascular Outcomes:
References
-
2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients With Persistent Hypertriglyceridemia: A Report of the American College of Cardiology Solution Set Oversight Committee. Virani SS, Morris PB, Agarwala A, et al. Journal of the American College of Cardiology. 2021;78(9):960-993. doi:10.1016/j.jacc.2021.06.011.
-
Clinical Trial Design for Triglyceride-Rich Lipoprotein-Lowering Therapies: JACC Focus Seminar 3/3. Malick WA, Waksman O, Do R, et al. Journal of the American College of Cardiology. 2023;81(16):1646-1658. doi:10.1016/j.jacc.2023.02.034.
-
Cardiovascular Impact of Nutritional Supplementation With Omega-3 Fatty Acids: JACC Focus Seminar. Weinberg RL, Brook RD, Rubenfire M, Eagle KA. Journal of the American College of Cardiology. 2021;77(5):593-608. doi:10.1016/j.jacc.2020.11.060.
-
Effect of High-Dose Omega-3 Fatty Acids vs Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk: The STRENGTH Randomized Clinical Trial. Nicholls SJ, Lincoff AM, Garcia M, et al. JAMA. 2020;324(22):2268-2280. doi:10.1001/jama.2020.22258.
-
A Synopsis of the Evidence for the Science and Clinical Management of Cardiovascular-Kidney-Metabolic (CKM) Syndrome: A Scientific Statement From the American Heart Association. Ndumele CE, Neeland IJ, Tuttle KR, et al. Circulation. 2023;148(20):1636-1664. doi:10.1161/CIR.0000000000001186.
-
Effects of Icosapent Ethyl on Total Ischemic Events: From REDUCE-IT. Bhatt DL, Steg PG, Miller M, et al. Journal of the American College of Cardiology. 2019;73(22):2791-2802. doi:10.1016/j.jacc.2019.02.032.
-
Triglycerides and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2011.Guideline
-
Clinical Management of Obesity – Third Edition. The Obesity Society (2025). 2025.Guideline
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















