2026 Diabetes Treatment Guidelines Update: ADA vs NICE
Mar 28, 2026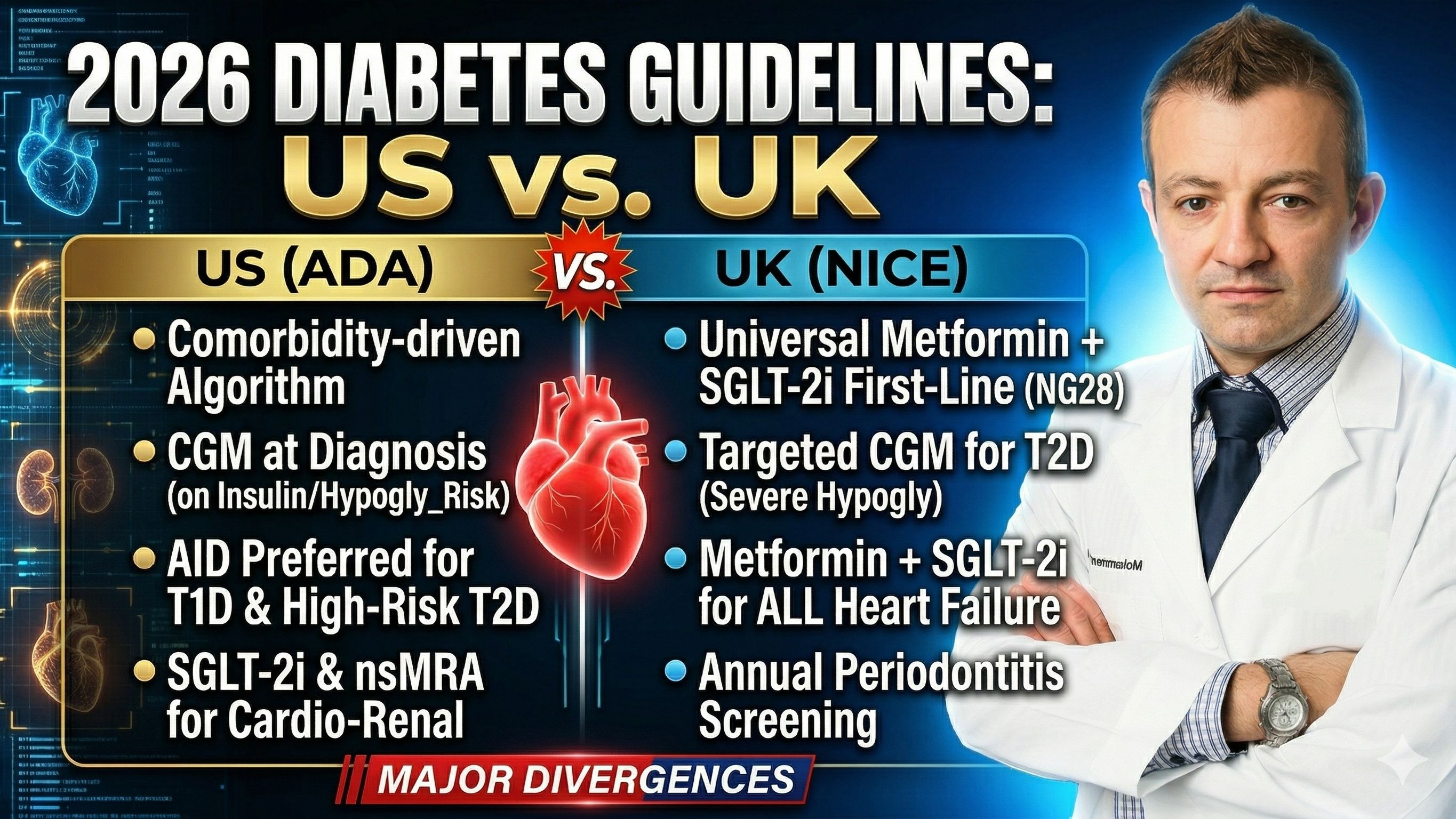
The US and UK Diabetes Treatment Guidelines 2026 Update
Two major diabetes guideline updates landed within weeks of each other at the start of 2026: the American Diabetes Association (ADA) Standards of Care in Diabetes 2026 and the UK’s NICE guideline NG28, updated in February 2026. Together, they represent the most comprehensive international refresh of diabetes management guidance in years.
In this article, I’ve synthesized both into a single, clinician-friendly algorithm, highlighting where they agree, where they differ, and what’s genuinely new. Throughout this article, recommendations are tagged as [ADA], [NICE], or [Both] so you can quickly see which guideline applies to your practice setting.
Diabetes can increase your risk of heart disease two to threefold and hence, cardiologists and other clinicians need to treat diabetes correctly and aggressively. We now have tools that can near completely reverse diabetes. There are so many new medications available, how do you know where to start?
Infographic Summary Comparing US and UK Diabetes Treatment Guidelines:

1. Screening and Diagnosis
Both guidelines support risk-based, individualized screening rather than universal population testing. The core populations to prioritize are:
- Adults with overweight or obesity plus at least one additional risk factor including; family history, physical inactivity, high-risk ethnicity, poor diet, hypertension, dyslipidemia, PCOS, prior gestational diabetes, prediabetes, or cardiovascular disease
- All adults aged 45 or older, regardless of weight
- Children aged 10 or older with overweight or obesity and two or more risk factors, screened at puberty onset
- Pregnant individuals: gestational diabetes screening at 24–28 weeks
New in ADA 2026
Screen individuals initiating immune checkpoint inhibitors, PI3Kα inhibitors, mTOR inhibitors, or high-dose glucocorticoids, a significant new addition for oncology and transplant patients. Annual OGTT from age 10 is the preferred screen for cystic fibrosis–related diabetes; A1C is acceptable when OGTT is not feasible.
Diagnostic Thresholds
The criteria are consistent across both guidelines:
|
Test |
Prediabetes |
Diabetes |
Source |
|
Fasting Plasma Glucose |
100–125 mg/dL |
≥126 mg/dL |
Both |
|
2-hr OGTT (75g) |
140–199 mg/dL |
≥200 mg/dL |
Both |
|
HbA1c / A1C |
5.7–6.4% (39–47 mmol/mol) |
≥6.5% (≥48 mmol/mol) |
Both |
|
Random Plasma Glucose |
— |
≥200 mg/dL + symptoms |
ADA only |
ADA Only — Type 1 Diabetes Staging
The ADA now formally recognizes T1D as a staged condition. A single confirmed IA-2 autoantibody now warrants monitoring equivalent to stage 2 disease, a new addition in 2026. Stage 3 requires prompt clinical evaluation when any autoantibody is present alongside symptomatic hyperglycemia.
2. Prevention and Delay
Both Guidelines
Structured lifestyle interventions targeting 5–7% weight loss remain the cornerstone of type 2 diabetes prevention. Physical activity should reach at least 30 minutes of moderate intensity on most days.
The ADA specifically names Mediterranean and low-carbohydrate eating patterns as having the strongest evidence base for T2D prevention. Technology-assisted programs, including smartphone apps, web-based tools, and telehealth, are confirmed as valid delivery formats.
New in ADA 2026 — Pharmacologic Prevention
Metformin should now be considered not just for prediabetes, but specifically to prevent hyperglycemia in high-risk patients initiating PI3Kα inhibitors (e.g., alpelisib, inavolisib) or high-dose glucocorticoids, two brand new indications added in 2026 . NICE does not address pharmacologic prevention of T2D in NG28.
3. Individualized Glycemic Goals
Both Guidelines
Glycemic targets must be individualized. Patient age, comorbidities, hypoglycemia risk, life expectancy, and personal preferences all matter. Neither guideline endorses a one-size-fits-all A1C target.
|
Population |
ADA A1C Goal |
NICE HbA1c Goal |
CGM TIR (ADA) |
|
Most non-pregnant adults (no hypoglycemia-risk meds) |
<7% (53 mmol/mol) |
48 mmol/mol (6.5%) |
>70% (70–180 mg/dL) |
|
On medicines associated with hypoglycemia |
<7% |
53 mmol/mol (7.0%) |
>70% |
|
Older adults (healthy) |
<7.0–7.5% |
Relax case-by-case |
>70% |
|
Older adults / frail / limited life expectancy |
<8.0–8.5% |
Relaxed — individualize |
>50% |
|
Perioperative (elective surgery) |
<8% within 3 months preop; 100–180 mg/dL intraop |
Not specified in NG28 |
TIR >50% or GMI <8% |
NICE
HbA1c should be measured every 3–6 months until stable on unchanging therapy, then every 6 months. If HbA1c rises to 58 mmol/mol (7.5%) or higher, reinforce lifestyle advice and intensify medicines with a target of (7.0%) 53 mmol/mol.
4. Diabetes Technology and CGM
Continuous Glucose Monitoring
ADA 2026 — Broad CGM Mandate
CGM is now recommended at diabetes onset for anyone on insulin, on agents that can cause hypoglycemia, or where CGM aids management. The evidence holds across all ages, incomes, and education levels. Three device categories are now recognized: real-time CGM (rtCGM), over-the-counter CGM (OTC-CGM), and professional CGM.
NICE NG28 — Targeted CGM for T2D
NICE takes a more targeted approach: offer isCGM to adults on multiple daily insulin injections who have recurrent or severe hypoglycemia, impaired hypoglycemia awareness, or a disability restricting standard finger-prick monitoring. Commissioners must actively monitor and address inequalities in CGM uptake by deprivation, ethnicity, and age.
Automated Insulin Delivery — ADA Only
The ADA made sweeping changes to AID recommendations in 2026:
- AID is now the preferred insulin delivery method for all people with type 1 diabetes
- AID is preferred for adults and children with T2D on multiple daily injections, CSII, or sensor-augmented pump therapy
- AID should be offered to all adults with T1D or T2D on insulin
- AID can be considered in T2D on basal insulin who are not meeting glycemic goals
- No C-peptide level, islet autoantibody status, or insulin duration is required before starting CSII or AID
- Children and adolescents must be supported in device use at school; adults aged 18 or over are entitled to reasonable workplace accommodations for device management
5. Pharmacologic Treatment — Type 2 Diabetes
Both Guidelines — Shared Foundations
Metformin remains central. SGLT-2 inhibitors are essential for cardiovascular and renal protection. GLP-1 RAs are prioritized for patients with established ASCVD or high CV risk. Never combine a GLP-1 RA with a DPP-4 inhibitor, no additive benefit. All treatment plans must incorporate healthy behaviors, diabetes self-management education, and attention to social determinants of health.
NICE NG28: A Major First-Line Shift
The most significant structural change in NICE NG28’s February 2026 update: metformin combined with an SGLT-2 inhibitor is now the standard first-line therapy for virtually all adults with type 2 diabetes, regardless of comorbidities. Modified-release metformin is preferred over standard-release for tolerability and adherence.
|
Patient Group |
NICE Initial Therapy |
If Metformin Contraindicated |
|
No relevant comorbidity |
Modified-release metformin + SGLT-2i |
SGLT-2i monotherapy |
|
Heart failure (any EF) |
Modified-release metformin + SGLT-2i |
SGLT-2i monotherapy |
|
Atherosclerotic CVD |
Metformin + SGLT-2i + subcutaneous semaglutide (Ozempic ≤1 mg/wk) |
SGLT-2i + semaglutide |
|
Early onset T2D (<40 yrs) |
Metformin + SGLT-2i + consider GLP-1 RA or tirzepatide |
SGLT-2i + consider GLP-1 RA or tirzepatide |
|
Obesity |
Metformin + SGLT-2i |
SGLT-2i monotherapy |
|
CKD eGFR >30 |
Metformin + SGLT-2i |
SGLT-2i monotherapy |
|
CKD eGFR 20–30 |
Dapagliflozin or empagliflozin + DPP-4i |
Dapagliflozin or empagliflozin + DPP-4i |
|
CKD eGFR <20 |
DPP-4i |
Pioglitazone or insulin |
|
Frailty |
Metformin + SGLT-2i only if volume depletion risk is low |
SGLT-2i if safe; otherwise DPP-4i |
ADA 2026: Comorbidity-Driven Algorithm
|
Priority Comorbidity |
ADA Preferred Approach |
|
ASCVD or high CV risk |
GLP-1 RA with demonstrated CV benefit ± SGLT-2i (Rec. 10.40c) |
|
HFpEF (symptomatic) |
Dual GIP/GLP-1 RA (tirzepatide) preferred; or GLP-1 RA with HF benefit. nsMRA for stage C HF with EF >40% (Rec. 9.9a, 10.44h) |
|
CKD |
SGLT-2i + nsMRA; GLP-1 RA for CV risk; simultaneous SGLT-2i + nsMRA now acceptable with UACR ≥100 mg/g + eGFR 30–90 on RAS inhibitor (new Rec. 11.9) |
|
MASLD / MASH |
GLP-1 RA with proven MASH benefit preferred; dual GIP/GLP-1 RA or pioglitazone for biopsy-proven MASH (Rec. 9.12–9.13a) |
|
Cancer treatment (new 2026) |
Metformin first-line for PI3Ki/mTOR inhibitor hyperglycaemia; assess for insulin in ICI-associated diabetes; adjust therapy around glucocorticoid regimen (Rec. 9.33–9.36) |
|
Post-transplant (new 2026) |
Insulin preferred post-op; DPP-4i for mild hyperglycaemia; GLP-1 RA long-term for cardiometabolic benefit (Rec. 9.37–9.38c) |
Key Divergences Between ADA and NICE
|
Topic |
ADA 2026 |
NICE NG28 |
Alignment |
|
First-line T2D |
Comorbidity-driven; no universal SGLT-2i mandate at first line |
Metformin + SGLT-2i for virtually all T2D adults from the start |
Complement |
|
GLP-1 RA naming |
Class-level recommendations |
Names semaglutide (Ozempic ≤1 mg/wk) specifically for ASCVD |
Complement |
|
Tirzepatide |
Broad — HFpEF, MASH, obesity, T1D |
Early-onset T2D and obesity only; not yet for ASCVD |
Complement |
|
HF subtyping |
Differentiates HFpEF vs HFrEF; tirzepatide for HFpEF + obesity |
Metformin + SGLT-2i for all HF regardless of EF |
Complement |
|
Cancer hyperglycaemia |
Detailed new 2026 algorithms for ICI, PI3Ki, mTOR, and steroids |
Not addressed in NG28 |
Complement |
|
MASLD / MASH |
Detailed guidance including fibrosis-based algorithms |
Not within scope of NG28 |
Complement |
6. Cardiovascular Risk and Comorbidity Management
Blood Pressure
Both Guidelines
Individualise BP targets. ACE inhibitor or ARB recommended in patients with albuminuria or CKD. General target for most adults with T2D: below 130/80 mmHg.
ADA 2026
Systolic BP below 120 mmHg is now encouraged for individuals at high cardiovascular or kidney risk. For older frail adults, a relaxed target of below 140/90 mmHg is acceptable. This is important if they are getting lightheaded or dizzy with lower readings, they may be hypotensive at home, but hypertensive at your office. . Antihypertensive threshold in pregnancy: ≥140/90 mmHg. Note: NICE NG28 defers hypertension management to its standalone hypertension guideline (NG136).
Heart Failure — New ADA Framework
- Stage B asymptomatic HF with high CV risk: GLP-1 RA with heart failure prevention benefit
- Stage C HFpEF with obesity: dual GIP/GLP-1 RA (tirzepatide) or GLP-1 RA with HF benefit
- Stage C HF with EF >40%: nonsteroidal MRA with proven benefit for reducing worsening heart failure events
Chronic Kidney Disease
Both Guidelines
SGLT-2 inhibitors are the cornerstone of kidney protection in T2D with CKD.
The ADA adds a notable new 2026 recommendation: simultaneous initiation of SGLT-2i and nsMRA can be considered in patients with T2D, UACR ≥100 mg/g, and eGFR 30–90 while on a RAS inhibitor. GLP-1 RA-based therapy can be initiated or continued in dialysis patients for cardiovascular risk reduction.
Lipids
ADA 2026 — Updated Statin Guidance
Do not add fibrates, niacin, or dietary n-3 fatty acid supplements to statin therapy, they do not confer additional cardiovascular risk reduction.
It's important to note that none of these improve outcomes, and niacin in particular worsens outcomes and insulin resistance, see the niacin article.
Retinopathy, Neuropathy, and Foot Care
[Both] Annual dilated eye exam; refer immediately at diagnosis to local eye screening service. The ADA’s 2026 update discusses GLP-1 RA effects on eye health including potential impacts on diabetic retinopathy progression, glaucoma, and macular degeneration. Combination pharmacotherapy is now preferred for neuropathic pain. Emerging foot care technologies, including smart insole thermometry for pre-ulceration detection, are now discussed.
Periodontitis — NICE Only
NICE NG28
Advise all T2D patients at annual review that periodontitis risk is elevated and that treating periodontitis improves glycemic control. Ensure regular oral health reviews. This is a low-cost, high-impact intervention that is routinely missed in clinical practice.
7. Obesity and Weight Management
Both Guidelines
Annual BMI screening is required. Target at least 5–7% weight loss from baseline. GLP-1 RAs and SGLT-2 inhibitors both have beneficial weight effects that should inform drug selection. Stop GLP-1 RAs or tirzepatide if BMI drops below 18.5 kg/m². Both guidelines note GLP-1 RAs may improve fertility, ensure contraception counselling before prescribing.
ADA 2026 — New for Type 1 Diabetes
GLP-1 RA–based therapy and/or metabolic surgery are now recognized treatment options for obesity in people with type 1 diabetes, a significant new addition. Individualize obesity pharmacotherapy dose and titration to balance efficacy, benefits, and tolerability.
NICE NG28
GLP-1 RA or tirzepatide should be added as further therapy for T2D with obesity after at least 3 months of initial therapy if glycemic targets are not met. For primary weight management, the NICE overweight and obesity management guideline takes precedence.
8. Special Populations
Older Adults (65 and Over)
Both Guidelines
Relaxed glycemic targets and simplified regimens for frail or older adults. Avoid sulfonylureas and insulin where possible due to hypoglycemia and falls risk.
[ADA] New tools for 2026 include a geriatric syndrome screening table (Table 13.1 in the original text, see links below) and a stepwise deintensification framework (Figure 13.2). Protein intake of at least 0.8 g/kg body weight per day is now specifically recommended to preserve lean mass. CGM is recommended for older adults with T1D or T2D on insulin. Blood pressure target: below 130/80 mmHg when safely achievable; relaxed to below 140/90 mmHg for those with poor health or high risk of adverse effects.
NICE NG28
Specific frailty prescribing algorithm: assess frailty before initiating medicines; consider withholding SGLT-2i if volume depletion risk is high; DPP-4i is preferred as further therapy in frailty; minimize polypharmacy and ensure the smallest effective doses.
Children and Adolescents — ADA Only
- Section 14 was fully reorganised in 2026 to clearly differentiate T1D from T2D guidance
- Psychosocial screening from age 7–8 years: diabetes distress, depression, anxiety, fear of hypoglycaemia, disordered eating
- Physical activity: at least 60 min/day of moderate-to-vigorous activity; bone and muscle strengthening at least 3 times per week
- Updated FDA approval status and paediatric RCT data added for GLP-1 RAs, SGLT-2 inhibitors, and tirzepatide in T2D
- Structured transition programmes to adult care, with digital tools to support continuity
Diabetes in Pregnancy
Both Guidelines
Insulin is the safest glucose-lowering agent in pregnancy. Discontinue GLP-1 RAs and tirzepatide before conception.
[ADA] The 2026 update adds preconception glucose goals, not just A1C targets, to guide therapeutic adjustments. All CGM and AID guidance in pregnancy is now consolidated in Section 15. A1C at 6–12 months postpartum can be used as supplementary information for those unable to complete the postpartum OGTT, but does not replace it as the gold standard.
Hospital and Perioperative Care — ADA New 2026
- A1C below 8% within 3 months of elective surgery improves postoperative outcomes; alternatively, 14-day GMI below 8% or time in range above 50% are acceptable
- Intraoperative glucose target: 100–180 mg/dL
- For patients discharged to non-home facilities, consider the facility’s diabetes management capabilities
- New clinical tables for DKA and HHS diagnostic criteria (Tables 16.1–16.2 in the original text, see links below)
NICE — Sick Day Rules
Every patient’s treatment plan must include clear sick day rules specifying whether to hold metformin and SGLT-2 inhibitors during illness or surgery, how to adjust insulin, and how to restart medications. Follow MHRA safety advice on ketone monitoring during SGLT-2i interruption.
9. Behavioural Health and Self-Management
Both Guidelines
Structured diabetes education at diagnosis and annually. Use non-judgemental language in all consultations. Integrate dietary, physical activity, and behavioural health advice with pharmacotherapy. Group education is the preferred format (NICE); an equal-standard individual option must be available.
ADA 2026
Screen annually for anxiety, diabetes distress, sleep health, and fear of hypoglycemia. Refer to a qualified behavioral health professional if distress is not resolved during the medical visit. Digital self-management tools and coaches should be considered as appropriate support options. Updated comprehensive prefasting risk assessment for patients who seek to fast during Ramadan.
NICE NG28
Dietary advice must be culturally sensitive and responsive to personal beliefs and willingness to change. Discourage patients from using foods marketed specifically for people with diabetes. Ensure regular oral health and dental reviews alongside other annual checks.
10. Ten Key Takeaways for 2026
- SGLT-2 inhibitor plus metformin is now first-line — at least in the UK.
NICE NG28 mandates this combination for virtually all adults with T2D from the start of treatment. The ADA agrees on its importance but approaches initiation through a comorbidity-driven lens.
- Start CGM at diagnosis, not as a last resort.
The ADA now recommends CGM at diabetes onset for anyone on insulin or at hypoglycemia risk. This is a meaningful shift away from the older “try finger-sticks first” approach.
- Automated insulin delivery is the new standard for type 1 diabetes.
AID systems are now preferred over standard pumps or injections. There is no C-peptide or autoantibody threshold required to start, remove that barrier.
- Cancer patients need glucose monitoring protocols.
The ADA added entirely new algorithms for hyperglycemia caused by immunotherapy, PI3K inhibitors, mTOR inhibitors, and steroids. These patients are increasingly in your clinic.
- Tirzepatide continues to expand its clinical footprint.
Both guidelines now endorse tirzepatide, the ADA broadly across HFpEF, MASH, obesity, sleep apnea, and T1D; NICE for early-onset T2D and obesity. Its role will only grow as post-marketing data accumulates.
- The nsMRA is now part of the standard toolkit.
The ADA recommends nonsteroidal MRA (finerenone) for stage C heart failure with EF above 40% and for CKD protection alongside SGLT-2i. If you’re not discussing this with your cardio-renal patients, start now.
- Stop adding fibrates or fish oil supplements to statins.
The ADA is now explicit: fibrates, niacin, and n-3 dietary supplements do not reduce cardiovascular events when added to statin therapy. Remove them from the regimen.
- Deintensify in frailty — both guidelines have frameworks for this.
The ADA’s new stepwise deintensification figure (Figure 13.2) and NICE’s frailty prescribing algorithm give you a structured way to reduce treatment burden when the risks outweigh the benefits.
- Check your patients’ teeth.
NICE NG28 mandates annual periodontitis screening in type 2 diabetes. Treating periodontal disease improves HbA1c. It is a simple, low-cost addition to the annual review that is routinely overlooked.
- Equitable access must be actively managed.
NICE mandates that commissioners and clinicians monitor SGLT-2 inhibitor and CGM uptake gaps by deprivation, ethnicity, and age, and actively work to close them. The most effective drugs must reach the highest-need patients.
References:
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes—2026. Diabetes Care 2026;49(Suppl. 1). https://doi.org/10.2337/dc26-SREV
- National Institute for Health and Care Excellence. Type 2 diabetes in adults: management [NG28]. Updated February 2026. www.nice.org.uk/guidance/ng28
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine